Ahmed Shabbir Chaudhry1**, Muhammad Naeem Shehzad2**, Maryum Akhtar3, Muhammad Subaan Fareed4, Usman Adrees5, Muhammad Daood Khan6, Hassan Shabbir Chaudhry7, Zoha Rubab8, and Hafiz Ghulam Murtaza Saleem1 *
1Graduate School of Medicine, Department of Pathology, Osaka Metropolitan University, Osaka, Japan
2University Institute of Medical Laboratory Science, The University of Lahore, Lahore, Pakistan
3College of Life Sciences Northwest Normal University, Anning District, Lanzhou, Gansu, P.R. China
4Institute of Biochemistry and Molecular Biology, School of Basic Medical Sciences, Lanzhou University, W, Lanzhou, China
5Department of Biology, Lahore Garrison University, Lahore, Pakistan
6Department of Human Genetics and Molecular Biology, University of Health Sciences, Lahore, Pakistan
7Department of General Medicine and Surgery, Indus Hospital, Punjab, Lahore
8Department of Physical Therapy, Islamia University Bahawalpur, Pakistan.
** Authors contributed equally
* Corresponding Author: [email protected]
Physiological jaundice is the most common condition that requires medical attention and hospital readmission of neonates. About 60% of term and 80% of preterm babies develop jaundice in the first week of life. Furthermore, about 10% of breastfed babies stay with jaundice until the age of 1 month. In the current study, a total of 139 neonates were evaluated for physiological jaundice in which 89 (64%) were male neonates and 50 (36%) were female neonates. Blood samples were collected under aseptic conditions. All samples were performed on Roche/Hitachi COBASc, based on the spectrophotometric technique. The mean SD (15.867±5.57) was calculated for the total, direct, and indirect bilirubin in neonates who were divided into 3 groups based on the number of days, that is, 1-2, 3-5, and 6-22 days, respectively. For indirect bilirubin in the age group of 1-2, ±SD was 13.80±5.41 in males, whereas it was ±10.40 in females, while the p-value < 0.01 was significant. Hyperbilirubinemia is associated with bilirubin due to a higher mass of red blood cells. It was found that the total, direct, and indirect bilirubin significantly increased in the 1st to 5th day of life after birth with male neonates being more vulnerable to pathological jaundice as compared to female neonates.
Keywords: hyperbilirubinemia, neonates, rh incompatibility, physiological jaundice, g6pd
Neonatal hyperbilirubinemia is a frequent clinical issue that affects newborns, especially in the first week of life [1, 2]. It usually affects around 8% to 11% of all newborns, causing them to be readmitted to the hospital [3, 4]. Hyperbilirubinemia is defined as an increase in total serum bilirubin (TSB) beyond the 95th percentile for age (high-risk zone) during the first week of birth [5, 6]. It is a serious clinical issue in Asia, particularly in Southeast Asia [7, 8]. In the 7th day of stretch life, 60% of term and 80% of preterm infants contract jaundice, while around 10% of breastfeeding children are as yet embittered at the age of one month [9]. According to a recent study, neonatal jaundice accounted for 13.5% of all admissions in Pakistani neonatal clinics [10]. Another published data which accounted for two major regional Pakistani investigations (n=1624 and 6454 patients, respectively) showed that approximately 26% and 30% of all patients were newborns who required neonatal jaundice examination [11, 12]. Premature birth, ABO or Rh mismatch, and other relevant infections have all been identified as major causes of jaundice [13, 14]. Hence, neonatal health and survival in developing countries, such as Pakistan, is a major concern [15, 16].
Physiologic jaundice is additionally alluded to as non-pathologic jaundice [17, 18]. This is a gentle and transient illness for the most part that happens because of the contrasts in the metabolic breakdown of bilirubin in the neonatal period, prompting an increased bilirubin load [19, 20]. Extreme hyperbilirubinemia in newborns is characterized by neurological dysfunction and is specifically known as bilirubin-induced neurologic dysfunction (BIND) [21, 22]. Phototherapy, IV immunoglobulin, and exchange transfusion are the techniques used to prevent severe bilirubin encephalopathy, kernicterus, and severe hyperbilirubinemia. In conjugated hyperbilirubinemia [23, 24], which may prompt the ‘bronze baby syndrome’ with greyish-brown discoloration of the skin [25] serum, and urine, the utilization of phototherapy is not indicated [26, 27]. The incidence of physiologic jaundice normally happens on the 2nd to 4th day, then peaks between the 4th to 5th day, and is sorted in two weeks [28, 29]. This can be related to a higher mass of red blood cells in newborns which results in an increased production of bilirubin resulting in a diminished life expectancy [30]. In the current study, the variation of hyperbilirubin levels in male and female neonates (1 to 22 days) in Pakistan was examined for the presence of any gender-specific differences.
2.1. Study Design
This was a retrospective study conducted over an eight-month period (from December 2018 to July 2019) at the University of Lahore Teaching Hospital. The sample size was n=139.
2.2. Reagents and Materials
Reagents and materials included phosphate 25 mmol/l, detergent, stabilizers, pH. 1.0 and 3.5 dichlorophenol diazonium salt: > 1.35 mmol/l.
2.3. Inclusion Criteria
Breast-fed babies with greenish-yellow stool, drowsiness, pale stool, bottle-fed babies with a greenish-mustard color stool, newborns with colorless urine, and poor sucking or feeding babies with dark urine were the particular subjects taken into consideration while sampling. No limitations were placed on the gender or geographic region of the participants.
2.4. Exclusion Criteria
The following factors, namely asphyxia, Rh incompatibility, and life-threatening congenital malformations were excluded. Newborns of women with a history of drug intake or gestational diabetes affecting the fetal liver were also excluded.
2.5. Sample Collection
Baby’s heels were gripped in a relatively firm grip with a non-dominant hand. The forefinger was placed below the ankle’s puncture site at the arch of the foot. According to the instructions of A.R. Surgical Instruments, an automated incision device was put against the heel. The device was removed from the puncture site shortly after blood droplets were collected using a capillary tube or blood bottle. The sample was taken from the nursery ward to the laboratory via a capillary tube. In the current study, precautions were taken to ensure the stability of the specimen, which was either serum or Li-heparin plasma. The specimen was stored at 15-25°C for 1 day, 2-8°C for 7 days, and (-15) -(-25)°C for up to 6 months to maintain its stability.
2.6. Diazo Method
The total bilirubin in the presence of an appropriate solubilizing agent is coupled with a 3.5 dichlorophenyl diazonium ion in a strongly acidic medium. The intensity of the color of the red azo dye produced is directly proportional to the total bilirubin concentration and can be measured photometrically. This is an in vitro test for the quantitative determination of total bilirubin in human serum and the plasma of both adults and neonates on Roche/Hitachi COBAS c 311 F. Hoffmann-La Roche AG Switzerland/ Boehringer Mannheim Germany/, (Spectrophotometer) systems [31].
2.7. Ethical Approval
Ethical approval with the REC number 15 was taken on 12-11-2018 from the ethical committee of the University Institute of Medical Laboratory Technology, University of Lahore.
2.8. Statistical Analysis
SPSS (v.22.0) software was used for statistical analysis.
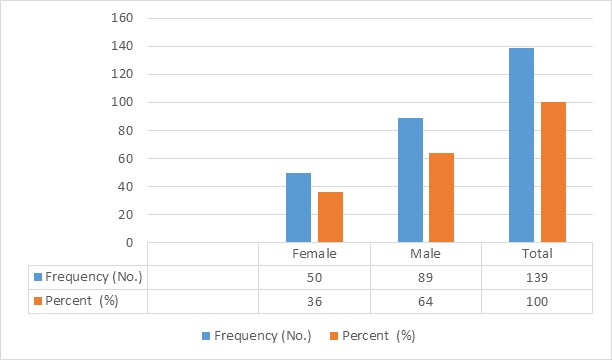
A total of 139 subjects were enrolled in the current study. The number of neonate male babies 89 (64%) was higher than female babies 50 (36%) (Figure 1). Neonates were divided into 3 groups based on their age in terms of number of days, that is, 1-2, 3-5, and 6-22 days. In age group 1-2, there was 1 (2%) female baby and 6 (6.7%) male babies. In age group 3-5, there were 32 (64%) female babies and 48 (53.9%) male babies. While there were 17 (34%) female babies and 35 (39.3%) male babies in age group 6-22, as shown in Table 1.
Table 1. Age-wise Frequency and Percentage of Male and Female Neonates
|
Gender |
Age (years) |
Frequency (N) |
Percentage (%) |
|
Female |
1-2 |
1 |
2 |
|
3-5 |
32 |
64 |
|
|
6-22 |
17 |
34 |
|
|
Total |
|
50 |
100 |
|
Male |
1-2 |
6 |
6.7 |
|
3-5 |
48 |
53.9 |
|
|
6-22 |
35 |
39.3 |
|
|
Total |
|
89 |
100 |
Table 2. Age-wise Frequency of Neonates According to Total Indirect and Direct Bilirubin
|
Age Group |
Bilirubin Total |
p-value |
Direct Bilirubin |
p-value |
Indirect Bilirubin |
p-value |
|||
|
Male |
Female |
Male |
Female |
Male |
Female |
||||
|
(No.) |
(No.) |
(No.) |
(No.) |
(No.) |
(No.) |
||||
|
1-2 |
(6) |
(1) |
.620 |
(6) |
(1) |
.421 |
(6) |
(1) |
<0.01 |
|
3-5 |
(48) |
(32) |
.526 |
(48) |
(32) |
.211 |
(48) |
(32) |
<0.01 |
|
6-22 |
(35) |
(17) |
.369 |
(35) .746±.510 |
(17) |
.607 |
(35) |
(17) |
<0.05 |
Table 3. Frequency of Total, Direct, and Indirect Bilirubin in Different Neonatal Age Groups
|
Age Group |
Bilirubin Total |
Direct Bilirubin |
Indirect Bilirubin |
|||
|
Normal (6.0-9.0 mg/dl) No. (%) |
High (>9.0mg/dl) No. (%) |
Normal (0.0-0.3mg/dl) No. (%) |
High (>0.3mg/dl) No. (%) |
Normal (5.7-8.7mg/dl) No. (%) |
High (>8.7mg/dl) No. (%) |
|
|
1-2 |
4(57.1) |
3(42.9) |
3(42.9) |
4(57.1) |
0 |
7(100) |
|
Total |
7 |
100 |
7 |
100 |
7 |
100 |
|
3-5 |
24 (30) |
56(70) |
21(26.3) |
59(73.8) |
27(33.8) |
53(66.3) |
|
Total |
80 |
100 |
80 |
100 |
80 |
100 |
|
6-22 |
25 (48.1) |
27(51.9) |
13(25) |
39(75) |
29(55.8) |
23(44.2) |
|
Total |
52 |
100 |
52 |
100 |
52 |
100 |
Figure 1. Frequency and Percentage of Neonates
3.1. Age-wise Analysis of Total, Indirect, and Direct Bilirubin in Neonates
3.1.1. Total Bilirubin and Direct Bilirubin. The mean standard deviation (±SD) and p-value were calculated for total and direct bilirubin for all three age groups, as shown in Table 2. The p-value of both age groups concerning total and direct bilirubin wasn’t significant (p-value > 0.05), as shown in Table 2.
The ±SD and p-value of the age group 1-2 for indirect bilirubin were calculated. The ±SD was 13.80±5.41 in male babies, whereas it was ±10.40 in female babies with a significant p-value < 0.01. In the age group 3-5, the ±SD was 13.51±2.70 in male babies, while it was 13.51±2.70 in female babies with the p-value < 0.05. It was followed by ±SD 11.74±3.48 in male babies and 11.28±2.81 in female babies in the age group 6-22 with p-value < 0.05 (Table 2).
3.1.2. Total Bilirubin and Direct Bilirubin Percentage. The percentage of total bilirubin was calculated concerning age groups. The age group 3-5 days showed the highest value 56 (70.0%) among all other groups, as shown in Table 3.
The age group 3-5 days showed the highest percentage of direct bilirubin 59 (73.8%) as compared to other respective groups, as shown in Table 3.
The age group 1-2 days showed all the 7 (100%) neonates with high values. In the age group 3-5 days, 53 (66.3%) neonates showed a high value, whereas 27 (33.8%) showed a normal value. In the age group 6-22 days, 23 (44.2%) neonates showed a high value and 29 (55.8%) showed a normal value.
Hyperbilirubinemia is one of the pervasive clinical conditions in the field of neonatology [3, 32]. Neonatal hyperbilirubinemia is stated as the common clinical condition which arises during the neonatal period, particularly in the first week of life [33, 34]. Hyperbilirubinemia occurs when TSB level exceeds the 95th percentile for age (high-risk zone) during the first week of birth [35, 36]. Identifying infants with risk factors is a crucial first step in effectively managing the infants with or at the risk of severe hyperbilirubinemia [24, 37]. In the current study, the frequency and percentage of male and female neonates susceptible to hyperbilirubinemia during the early weeks of life was analyzed, as shown in Figure 2.
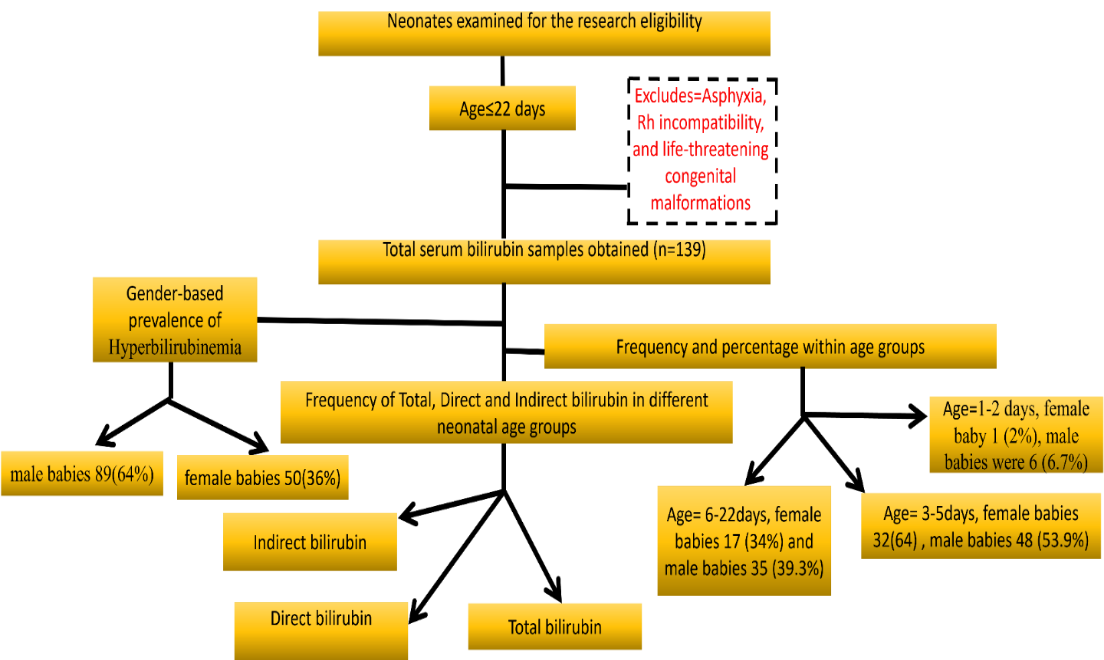
Figure 2. Schematic Illustration of the Study
It was found that approximately 5% of patients were admitted during the first 24 hours of their lives. According to a previous study [38] conducted in other cities across the country, peak bilirubin levels were not linked to feeding commencement or type [39, 40]. The majority of problems with newborns occurred within the first 24 hours of life. It was also found that male newborns were more affected, which is also consistent with other studies conducted at different institutions in Pakistan [39]. Another study in Peshawar showed that the majority of male newborns were admitted during the first 24 hours of life, similar to the current findings that showed male neonates as more vulnerable to hyperbilirubinemia [41]. The current study’s sample size was 139 which is higher than most of the studies conducted in Pakistan [38].
The current findings align with the previously published data, including a study conducted at Eku Baptist Community Hospital in Delta State, Nigeria. In particular, the results regarding TSB levels of 6.0-9.0 mg/dl on the 2nd day (14.233±5.57) are consistent with the data reported by Agarwal et al. and Awasthi et al, as shown in Table 2 [42, 43]. In the current study, the 1st day TSB level of 6mg/dl in 4 neonates (57.1%) was observed, which is similar to the findings of another study [44]. The results also demonstrated a significant correlation between the indirect bilirubin level and hours (p < 0.01 and p < 0.01) within the first 48 hours. This is in line with the typical presentation of jaundice, which typically arises from high levels of unconjugated or indirect bilirubin in serum, with a serum level of less than 7mg/dl from the 2nd to the 6th day and less than 7mg/dl beyond the 6th day. The findings align with the results presented in Table 3 [45, 46]. Jaundice that emerges within 24 hours due to an increase in serum bilirubin above 0.3mg/dl/day, peak values above the predicted normal range, lasting clinical jaundice for more than two weeks, and conjugated bilirubin (dark urine stained clothes) is classified as physiological jaundice [47–49].
4.1. Limitations and Strength
This is the first study in Pakistan that showed variation in bilirubin levels in male and female newborns. The sample size was significantly larger than that of other similar studies. Although statistically significant, a slight variation in bilirubin levels between male and female babies may look clinically insignificant. However, the findings revived the interest in a previously explored issue, namely the super female infant, albeit with new applications.
In the current study, the examination of potential gender-specific differences in blood albumin concentrations of neonates and its potential influence on the susceptibility of the central nervous system to elevated serum bilirubin levels would have been useful. However, certain limitations were encountered during the study, such as a single-center design and a short study period. Additionally, hematocrit levels were not taken into account and peak bilirubin levels were not linked to feeding commencement or type.
It should also be noted that the study population consisted of hospitalized neonates who received prompt medical care. In Pakistan, a significant proportion of births take place at home (65%) and this may lead to a selection bias, potentially masking the true extent of the problem. The risks associated with maternal factors such as primiparity and place of delivery can be addressed through improved maternal and public health education. Therefore, further studies are needed to address the research gaps in this area.
4.2. Conclusion
The current study found that total direct and indirect bilirubin levels increased unequivocally from the 1st to the 5th day, with male neonates being more susceptible to pathological jaundice as compared to female neonates. The significance of this research lies in its contribution to a larger and more complex understanding of the physiological and pathological phenomena associated with the male gender, particularly with regards to the susceptibility and protection of male newborns. The influence of gender on neonatal illness and its outcomes remains an important topic of investigation. Hence, further research, including randomized controlled trials, are needed to fully understand the mechanisms involved.