
| Review | Open Access |
|---|
Influence of Energy Drinks on Different Cardiovascular Parameters of Healthy Young Adults: A Pilot Study |

|
|---|
![]() Fayzan Akhtar ,
Fayzan Akhtar ,
![]() Arifa Savanur ,
Arifa Savanur ,
![]() Quratulain Zia ,and
Quratulain Zia ,and
![]() Mudassir Rizvi*
Mudassir Rizvi*
Department of Physiology, University of Karachi, Main University Road Karachi
Background. Energy drink (ED) intake is associated with acute changes in cardiovascular indices. However, the amplitude of electrocardiographic (ECG) waves have been scarcely studied and gender difference has not been explored either. The current study aims to observe changes in ECG under the influence of ED with focusing on gender differences.
Methods. Twenty healthy participants with an average age of 22 years were enrolled in this study. Half of the participants were male and half were female. This study was conducted in the Department of Physiology, University of Karachi from July 2019 to October 2019. The participants were asked to drink 500 ml of ED. Later limb lead ECG was performed before (Before-ED) and 2 hours after (After-ED) intake. Recording and data analysis was done through Powerlab. Heart rate (HR) corrected QT interval (QTc), R wave, and T wave amplitudes and HR were calculated and analyzed.
Results. QTc was found to increase (10%) in After-ED as compared to Before-ED. In contrast, T wave was found to reduce (37%) in After-ED. These results were statistically significant (p < 0.05). These changes in QTc and T waves were similar in both male and female subjects. The HR did not change in males. In females, it increased from an average of 82 bpm in Before-ED to 92 bpm in After-ED and the difference was statistically significant (p < 0.05).
Conclusion. Acute intake of energy drinks produces acute changes in ECG with no gender difference. Thus, regular intake of these drinks should be avoided.
Highlights
- Acute changes are produced in ECG under acute intake of ED in young healthy subjects.
- T wave amplitude is reduced under an acute intake of ED.
- Gender difference is found in HR under an acute intake of ED.
Graphical Abstract
1. INTRODUCTION
Energy drinks (ED) are soft beverages containing a high percentage of caffeine and other additives, including carbohydrates amino acids such as taurine and herbal stimulants [1]. Their consumption is claimed to have positive physical and mental effects, such as improved alertness and mood, increased endurance and athletic performance, as well as weight loss [2]. The consumption of these drinks is higher in young adolescents and children in different population groups [3, 4]. In Pakistan, its prevalence in students is around 40-50% [5]. The amount of caffeine added in different EDs varies from less than 100gm/serving to as much as 500mg/serving [6], which is labeled as high caffeine as compared to tea and coffee. An intake of 400mg caffeine/day is considered as safe.
Caffeine produces a variety of physiological effects on different systems including the nervous system, cardiovascular system, excretory system such as diuresis, cardiac muscle stimulation, central nervous system stimulation, smooth muscle relaxation, stimulation of gastric acid secretion, and elevation of plasma free fatty acids and glucose. Excessive intake of these drinks can cause myocardial infarction [7]. On the other hand, consumption even in small amounts can acutely influence cardiovascular system in non-habitual subjects [8-10]. Variations in systolic and diastolic blood pressures, HR, QT interval, and QTc are frequently observed [8, 10, 11]. These effects are developed within an hour [[9] and subside after a few hours [12]. An increase in blood pressure is mostly consistent with ED consumption, as found in different studies [13]. However, conflicting data is available regarding heart rate and ECG parameters including QTc from increase to none to decrease [8, 9, 11, 12]. In addition to ED, caffeine consumption also shows a dose dependent decrease in HR [14]. Caffeinated ED changes blood pressure significantly but not the non-caffeinated ED [15]. Changes in these parameters, where observed, are of different magnitude [11, 16]. In addition, a lot of research is available regarding change in the duration of ECG. However, the effects of energy drinks on amplitudes in ECG waves have not been described.
Gender differences exist among various cardiovascular parameters [17-19], as well as the effects of caffeine on cardiovascular parameters [20, 21]. In light of the above description, the current study aims to analyze gender differences regarding the effects of acutely consumed energy drinks on cardiovascular functions. Furthermore, HR and ECG parameters are assessed.
2. MATERIALS AND METHODS
This is a pre-post type of interventional study conducted in the Department of Physiology, University of Karachi from July 2019 to October 2019. Prior ethical approval was obtained from the departmental research committee and the procedure was conducted in accordance with the ethical standards of the latest version of Helsinki Declaration. A total of 20 young and healthy participants of the age group 20-25 years were recruited. Power analysis and sample size determination was done with G power 3.1.9.7. All participants signed the informed consent. They were all students of the department with no prior history of any cardiovascular condition. Half of them were male and half were female. Furthermore, they were non-smokers, non-alcoholic, and non-users of energy drinks. The participants were also asked not to take any caffeinated beverage 12 hours before the experimentation. An ED, namely sting, was used for their consumption. It is commercially available in a bottle of 500 ml and includes carbohydrates, several vitamins, ginseng, inositol, taurine, and caffeine. There is about 200 mg/l of caffeine present in it [22]. Baseline blood pressure and HR was tested before ED intake. ECG was recorded and analyzed by using limb lead associated with the physiological data acquisition system Powerlab, (ADInstruments, Australia). Four limb leads were attached with each limb and were connected with a bio amplifier through bio amplifier cable. Electrode gel was applied on skin surface where electrodes were attached. Chart software was used to acquire and analyze data. Bio amplifier settings were as follows: sampling rate: 200/sec, range: 2 mv, low pass filter; 50 Hz, and high pass filter: 0.5 Hz. These are recommended settings by the manufacturer. The measured cardiovascular parameters included QT interval, T wave amplitude, R wave amplitude, and HR.
All the subjects were asked to sit comfortably in supine position for 10 to 15 mins before the start of recording. After the rest period, electrodes were applied and baseline ECG was recorded. It was followed by the drinking of a half-liter bottle of sting as ED by all subjects. After one hour, ECG was recorded again.
Statistical analysis was done through MS Excel and SPSS. All records were shown as mean + SD. Means were compared with student t-test, while multiple comparisons were made through ANOVA using Bonferroni’s post hoc test. The obtained value, (0.05) was considered as significant.
3. RESULTS
3.1. Effects of ED on QTc IntervalAfter an hour of consuming ED, a marked change in QTc interval was observed, as shown in Figure 1. An increase of about 0.039 + 0.002 s (13 %) in QTc interval was observed in both gender and the difference was statistically significant (p = 0.000) before and after the drinking of ED. However, no gender difference was observed and the mean QTc interval remained the same in both males and females before and after having ED.
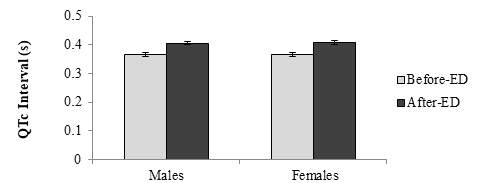
Figure 1: Heart rate corrected QT interval (QTc) before (before-ED) and after (After-ED) intake of ED in both genders. Error bars are showing standard error. (n = 10, statistical significance in males; p = 0.000, in females; p = 0.000)
3.2. Effects of ED on T wave AmplitudeThe amplitude of T wave was also found changed under the influence of ED in both males and females, as shown in Figure 2. There was a decrease of about 0.08 + 0.05 mV (66 %) in T wave amplitude in both gender and this difference was statistically significant (males: p = 0.019, females: p = 0.030). However, consistent with the QTc interval, no gender difference was found in T wave amplitude.
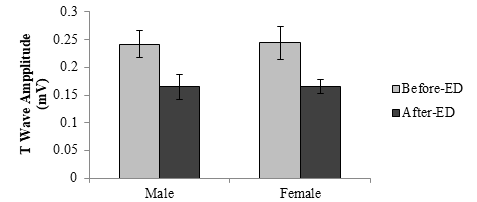
Figure 2: Amplitude of T wave before (before-ED) and after (After-ED) intake of ED in both genders. Error bars are showing standard error (n = 20, statistical significance; in males; p = 0.019, in females; p = 0.030)
3.3. Effects of ED on QRS Complex AmplitudeR wave of QRS complex showed an increase of 0.50 + 0.04 mV (14 %) in males and 0.10 + 0.01 mV (31 %) in females, as shown in Figure 3. However, this difference was not statistically significant (p = 0.876). The same pattern was observed in both male and female subjects and no gender difference was found.
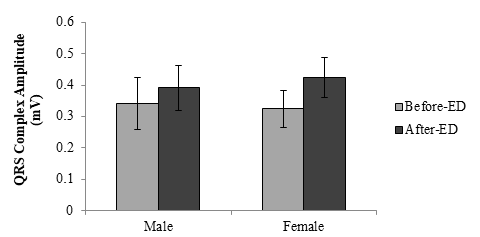
Figure 3: Amplitude of R wave of QRS complex before (before-ED) and after (After-ED) intake of ED in both genders. Error bars are showing standard error (n = 10, statistical significance; in males; p = 0.275, in females; p = 0.646)
3.4. Effect of Energy Drinks on HRThe only parameter in which gender difference was observed was HR. In males, no change in HR was found after an hour of ED consumption, as shown in Figure 4. In females, an increase of 10+4 bpm (11%) in HR was observed under the influence of ED and the difference was statistically significant (p = 0.019).
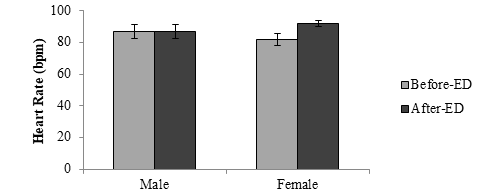
Figure 4: Heart rate before (before-ED) and after (After-ED) intake of ED in both genders. Error bars are showing standard error (n = 20, statistical significance; in males; p = 1.000, in females; p = 0.019)
4. DISCUSSION
Several recent studies showed the acute effects of caffeinated ED on different cardiovascular parameters, including blood pressure and ECG. In the current study, changes in HR as well as time and voltage dependent characteristics of ECG were studied, while focusing on gender difference. The current results showed an increase in QTc interval and a marked reduction in T wave amplitude due to ED consumption but without any gender difference. Previous studies showed that change in QTc was observed at high doses of 800-1000ml of EDs but not in low doses of less than 300ml [12, 13, 23]. Thus, the current results obtained with 500ml volume of ED consumption are consistent with previous studies. Considering the fact that these experiments were performed on healthy individuals with a single intake of ED, any change in ECG would be temporary and would not be a sign of any pathological condition. However, baseline changes in ECG in healthy individuals can manifest later in life as severe pathological conditions [24]. Thus, a continuous use of these drinks can increase the risk of cardiac abnormalities [25]. In addition, these changes should not be considered as beat to beat variations in ECG. The obtained results show a significantly increased QTc interval, but these values did not reach the pathological range, which is greater than 440 ms in men and 460 ms in women [26]. In addition, several experimental evidences are available which show a link between different ingredients of ED and change in the QTc interval. QTc represents the ventricular action potential. Its prolongation of the acquired type is well described under the effects of several medications where QTc increases due to electrolyte imbalances [26]. Electrolyte imbalances include hypokalemia, hypocalcaemia, and hypomagnesaemia. Caffeine in a high concentration in serum has a negative correlation with serum potassium [27]. In addition, medicines which increase QTc interval block the inward rectifier potassium channel (IKr) [28]. Moreover, ginseng is also related with reversible QTc prolongation [29]. Recently, in isolated heart preparation, the term of QTc was demonstrated under the influence of caffeine and taurine [30]. Thus, further research is required.
Change in T wave amplitude after ED or caffeine intake is scarcely documented in literature [31]. T wave originates due to the heterogeneous repolarization of different areas of ventricles which, in turn, depends on variations in activation time and the duration of action potential [32]. In healthy individuals, T wave amplitude is correlated with several factors including gender, HR, blood CO2 concentration, and exercises [33-35]. T wave is also correlated with aging, that is, with age it undergoes flattening [36]. T waves with a low amplitude are correlated as well with cardiovascular mortality [37]. In addition, repolarization in ventricles is also sensitive to temperature and ionic balances [32]. High calorie intake also reduces T wave amplitude. However, certain conflicting evidences are also reported in the literature which negate the role of caffeine [38] or ginseng in ECG changes [39, 40]. Thus, for different ingredients of EDs, detailed investigations are required to determine reasonable factors which produce ECG changes acutely [1].
4.1. LimitationsThe recording of ECG with only limb leads was a significant limitation of this study. This is because limb leads and chest leads show cardiac electrical activity with different angles. Hence, further research with the use of both chest and limb leads is recommended to confirm the results.
4.2. ConclusionIn conclusion, an acute intake of energy drinks produces such acute changes in ECG which are otherwise related with pathological conditions, including prolong QTc and reduced T wave amplitude. These effects are independent of gender differences. The reasons for these changes may be temporary ionic disturbances and temporary autonomic imbalance, among others. It could be predicted with these results that regular intake of these drinks may have detrimental effects on cardiac health in both males and females.
AUTHOR CONTRIBUTION
Fayzan Akhter: conceptualization, acquisition investigation, writing - original draft. Arifa Savanur: methodology, project administration, supervision, review & editing. Quratulain: methodology, project administration, supervision, review & editing. Mudassir Rizvi: conceptualization, formal analysis, project administration, supervision, review & editing.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
Data supporting the findings of this study will be made available by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
Generative AI Disclosure Statement
The authors did not used any type of generative artificial intelligence software for this research.
REFERENCES
- Jagim AR, Harty PS, Tinsley GM, et al. International society of sports nutrition position stand: energy drinks and energy shots. J Int Soc Sports Nutr. 2023;20(1):e2171314. https://doi.org/10.1080/15502783.2023.2171314
- Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks--a growing problem. Drug Alcohol Depend. 2009;99(1-3):1–10. https://doi.org/10.1016/j.drugalcdep.2008.08.001
- Reid JL, McCrory C, White CM, et al. Consumption of caffeinated energy drinks among youth and young adults in Canada. Prev Med Rep. 2017;5:65–70. https://doi.org/10.1016/j.pmedr.2016.11.012
- Zucconi S, Volpato C, Adinolfi F, et al. Gathering consumption data on specific consumer groups of energy drinks. EFSA Support Publ. 2013;10(3):e394E. https://doi.org/10.2903/sp.efsa.2013.EN-394
- Aslam HM, Mughal A, Edhi MM, et al. Assessment of pattern for consumption and awareness regarding energy drinks among medical students. Arch Public Health. 2013;71(1):e31. https://doi.org/10.1186/2049-3258-71-31
- Higgins JP, Tuttle TD, Higgins CL. Energy beverages: content and safety. Mayo Clin Proc. 2010;85(11):1033–1041. https://doi.org/10.4065/mcp.2010.0381
- Pallangyo P, Bhalia SV, Komba M, et al. Acute Myocardial infarction following the consumption of energy drink in a 28-year-old male: a case report. J Invest Med High Impact Case Rep. 2023;11:1–15. https://doi.org/10.1177/23247096231168811
- García A, Romero C, Arroyave C, Giraldo F, Sánchez L, Sánchez J. Acute effects of energy drinks in medical students. Eur J Nutr. Sep 2017;56(6):2081–2091. https://doi.org/10.1007/s00394-016-1246-5
- Caliskan SG, Kilic MA, Bilgin MD. Acute effects of energy drink on hemodynamic and electrophysiologic parameters in habitual and non-habitual caffeine consumers. Clin Nutr ESPEN. 2021;42:333– 338. https://doi.org/10.1016/j.clnesp.2021.01.011
- Gualberto PIB, Benvindo VV, Waclawovsky G, Deresz LF. Acute effects of energy drink consumption on cardiovascular parameters in healthy adults: a systematic review and meta-analysis of randomized clinical trials. Nutr Rev. 2023;82(8);1028–1045. https://doi.org/10.1093/nutrit/nuad112
- Elitok A, Öz F, Panc C, et al. Acute effects of Red Bull energy drink on ventricular repolarization in healthy young volunteers: a prospective study. Anatol J Cardiol. Nov 2015;15(11):919–922. https://doi.org/10.5152/akd.2015.5791
- Basrai M, Schweinlin A, Menzel J, et al. Energy drinks induce acute cardiovascular and metabolic changes pointing to potential risks for young adults: a randomized controlled trial. J Nutr. 2019;149(3):441–450. https://doi.org/10.1093/jn/nxy303
- Hajsadeghi S, Mohammadpour F, Manteghi MJ, et al. Effects of energy drinks on blood pressure, heart rate, and electrocardiographic parameters: an experimental study on healthy young adults. Anatol J Cardiol. 2016;16(2):94–99. https://doi.org/10.5152/akd.2015.5930
- Temple JL, Dewey AM, Briatico LN. Effects of acute caffeine administration on adolescents. Exp Clin Psychopharmacol. 2010;18(6):510–520. https://doi.org/10.1037/a0021651
- Phan JK, Shah SA. Effect of caffeinated versus noncaffeinated energy drinks on central blood pressures. Pharmacother: J Human Pharmacol Drug Ther. 2014;34(6):555–560. https://doi.org/10.1002/phar.1419
- Grasser EK, Yepuri G, Dulloo AG, Montani J-P. Cardio- and cerebrovascular responses to the energy drink Red Bull in young adults: a randomized cross-over study. Eur J Nutr. 2014;53(7):1561–1571. https://doi.org/10.1007/s00394-014-0661-8
- Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;37(5):1199–11208. https://doi.org/10.1161/01.hyp.37.5.1199
- Prabhavathi K, Selvi KT, Poornima KN, Sarvanan A. Role of biological sex in normal cardiac function and in its disease outcome - a review. J Clin Diagn Res. Aug 2014;8(8):eBe01–4. https://doi.org/10.7860/jcdr/2014/9635.4771
- Moss AJ. Gender differences in ECG parameters and their clinical implications. Ann Noninvasive Electrocardiol. 2010;15(1):1–2. https://doi.org/10.1111/j.1542-474X.2009.00345.x
- Temple JL, Ziegler AM. Gender differences in subjective and physiological responses to caffeine and the role of steroid hormones. J Caffeine Res. 2011;1(1):41–48. https://doi.org/10.1089/jcr.2011.0005
- Temple JL, Ziegler AM, Graczyk A, Bendlin A, Sion T, Vattana K. Cardiovascular responses to caffeine by gender and pubertal stage. Pediatrics. 2014;134(1):e112–119. https://doi.org/10.1542/peds.2013-3962
- Tien T. Sting energy drink ingredients and nutrition facts. Grocery Asia Web site. https://egrocery.asia/sting-energy-drink-ingredients.html. Updated September 12, 2021.
- Shah SA, Szeto AH, Farewell R, et al. Impact of high volume energy drink consumption on electrocardiographic and blood pressure parameters: a randomized trial. Journal of the Am Heart Association. 2019;8(11):e011318. https://doi.org/10.1161/JAHA.118.011318
- Erelund S, Karp K, Wiklund U, Hörnsten R, Arvidsson S. Are ECG changes in heart-healthy individuals of various ages related to cardiac disease 20 years later? Ups J Med Sci. 2021;126(1):e6064. https://doi.org/10.48101/ujms.v126.6064
- Lasheras I, Seral P, Alonso-Ventura V, Santabárbara J. The impact of acute energy drink consumption on electrical heart disease: a systematic review and meta-analysis. J Electrocardiol. 2021;65:128–135. https://doi.org/10.1016/j.jelectrocard.2021.01.020
- Al-Akchar M. Long QT Syndrome. StatPearls Publishing; 2022.
- Tsuji T, Morita S, Saito T, Nakagawa Y, Inokuchi S. Serum potassium level as a biomarker for acute caffeine poisoning. Acute Med Surg. 2020;7(1):e568. https://doi.org/10.1002/ams2.568
- Nachimuthu S, Assar MD, Schussler JM. Drug-induced QT interval prolongation: mechanisms and clinical management. Ther Adv Drug Saf. 2012;3(5):241–53. https://doi.org/10.1177/2042098612454283
- Torbey E, Abi Rafeh N, Khoueiry G, Kowalski M, Bekheit S. Ginseng: a potential cause of long QT. J Electrocardiol. 2011;44(3):357–358. https://doi.org/10.1016/j.jelectrocard.2010.08.007
- Ellermann C, Hakenes T, Wolfes J, et al. Cardiovascular risk of energy drinks: Caffeine and taurine facilitate ventricular arrhythmias in a sensitive whole-heart model. J Cardiovasc Electrophysiol. 2022;33(6):1290–1297. https://doi.org/10.1111/jce.15458
- Uddin M, Hossain M, Ahmad M, Ahmed N, Rashid M. Effects of Caffeinated beverage consumption on electrocardiographic parameters among healthy adults. Modern Appl Sci. 2014;8(2):69–77. https://doi.org/10.5539/mas.v8n2p69
- Arteyeva NV. Dispersion of ventricular repolarization: temporal and spatial. World J Cardiol. 2020;12(9):437–449. https://doi.org/10.4330/wjc.v12.i9.437
- Arbel Y, Birati EY, Shapira I, Topilsky Y, Wirguin M, Canaani MDJ. T-wave amplitude is related to physical fitness status. Ann Noninvasive Electrocardiol. 2012;17(3):214–218. https://doi.org/10.1111/j.1542-474X.2012.00512.x
- Rutherford JJ, Clutton-Brock TH, Parkes MJ. Hypocapnia reduces the T wave of the electrocardiogram in normal human subjects. Am J Physiol-Regulat Integ Compar Physiol. 2005;289(1):R148–R155. https://doi.org/10.1152/ajpregu.00085.2005
- Langley P, Di Bernardo D, Murray A. Quantification of T wave shape changes following exercise. Pacing Clin Electrophysiol. 2002;25(8):1230–1234. https://doi.org//10.1046/j.1460-9592.2002.01230.x
- Simonson E. The effect of age on the electrocardiogram. Am J Cardiol. 1972;29(1):64–73. https://doi.org/10.1016/0002-9149(72)90417-1
- Holkeri A, Eranti A, Haukilahti MAE, et al. Prognostic significance of flat T-waves in the lateral leads in general population. J Electrocardiol. 2021;69:105–110. https://doi.org/10.1016/j.jelectrocard.2021.10.001
- Farber J, Dikdan S, Ruge M, Johnson D, Shipon D. Relationship between Caffeine consumption and young athletes’ comorbidities, exercise-related symptoms, and baseline electrocardiogram. Sports Health. 2023;10(3):448–456. https://doi.org/10.1177/19417381231168828
- Shah SA, Occiano A, Nguyen TA, et al. Electrocardiographic and blood pressure effects of energy drinks and Panax ginseng in healthy volunteers: a randomized clinical trial. Int J Cardiol. 2016;218:318–323. https://doi.org/10.1016/j.ijcard.2016.05.007
- Fletcher EA, Lacey CS, Aaron M, Kolasa M, Occiano A, Shah SA. Randomized controlled trial of high‐volume energy drink versus Caffeine consumption on ECG and hemodynamic parameters. J Am Heart Assoc. 2017;6(5):e004448. https://doi.org/10.1161/JAHA.116.004448