
| Review | Open Access |
|---|
Phenotypic Characterization of Multidrug Resistant Klebsiella Spp. Isolated from Pediatric Patients |
 |
|---|
![]() Azka Asghar1 , Atika Hashmi1* , Waqas Ali3, Ayesha Khalid4, Aqsa Ashiq5, and Abeeha Shahzad Khan5
Azka Asghar1 , Atika Hashmi1* , Waqas Ali3, Ayesha Khalid4, Aqsa Ashiq5, and Abeeha Shahzad Khan5
1Department of Biology, Lahore Garrison University, Pakistan
2Department of Laboratory Sciences, Sheikh Zayed Hospital, Lahore, Pakistan
3Department of medical Laboratory Sciences, University of Child Health Sciences, The Children’s Hospital, Lahore, Pakistan
4Department of Microbiology and molecular genetics, Punjab university, Lahore, Pakistan
5Department of medical Laboratory sciences, Superior university, Lahore, Pakistan
Background. Multidrug resistant (MDR) Klebsiella has become a global problem and its infections are difficult to eradicate due to the presence of β-lactamases. The current study aimed to identify multidrug resistant isolates in children due to their high prevalence in Lahore, Pakistan.
Methodology. In this study, 150 samples of blood, urine, pus, ascitic fluid, pleural fluid, Bronchoalveolar lavage (BAL), and CSF were collected from patients admitted in the University of Child Health Sciences, The Children’s Hospital, Lahore from November 2021 to April 2022. Then, different microbiological techniques including culturing, Gram staining, identification of different species by using API, antibiotic susceptibility testing as well as molecular techniques including PCR, were used to identify MDR Klebsiella spp. positive samples.
Results. Out of the 150 samples, 58 were found positive for Klebsiella spp. while 92 were negative for Klebsiella spp. Among these 58 strains, 48 came from urine samples, 8 from pus samples, and 2 from blood samples. Furthermore, 34 were collected from male and 24 from female patients. The age group of the sampled children was 6 to 10 years. Afterwards, these 58 isolates were screened for extended spectrum β-lactamase (ESBL), metallo β-lactamase (MBL) and AmpC. It was found that out of these 58 isolates, 12 were ESBL positive (20.68%), 11 were MBL positive (18.9%) and 20 were AmpC positive (34.48%). Among β-lactamase genes, NDM -1 (72.7 %), SHV (41.6%), TEM (8.3%) and CTX-M (25%) were detected.
Conclusion. The study concluded that the rate of MDR Klebsiella infection is high in children and it may be complicated for the clinicians to treat them.
Highlights
- Collection of Samples from The Children’s Hospital for the isolation of Klebsiella
- Screening by using microbiological techniques for microbe identification.
- Antimicrobial sensitivity testing on all Klebsiella positive samples. ESBL, MBL, and AmpC were phenotypically characterized.
- Identification of enzymes related to resistance on gene level.
1. INTRODUCTION
The prevalence of β-lactamases is increasingly being reported worldwide. β-lactams are commonly used broad-spectrum antibiotics with a high efficacy, cost-effectiveness, easy delivery, and low adverse effects. Irrational use and overuse of antibiotics has caused new strains of bacteria to emerge with multidrug resistance (MDR) patterns. Klebsiella spp. is a β-lactamase-producing bacteria causing respiratory infections and post-surgical complications in immunocompromised patients [1].
Klebsiella spp. is a gram-negative, rod-shaped, encapsulated bacteria that belongs to the family Enterobacteriaceae. It is a non-motile bacteria and can ferment lactose. About 78 serotypes of Klebsiella spp. have been determined [2]. High antibiotic intake has caused the rise of resistance among organisms, while multiple antimicrobial resistance has turned into a significant medical problem [3]. The epidemiology of resistant bacteria depends upon the geographical region, as well as population susceptibility. Occasionally, it changes from one population center to another within the same country due to the variability in the pattern of antibiotic usage and changes in the way of life [4].
Three major groups of β-lactamases including cephalosporin (AmpC), extended spectrum β- lactamases (ESBL) and carbapenamases such as metallogen β-lactamase (MBL) are of great concern in healthcare settings. The presence of ESBL, AmpC, and MBL in a single bacterial specie lessens the efficacy of β-lactam containing antibiotics, β-lactamase inhibitor and carbapenams, collectively [5]. The main function of ESBL is to degrade aztreonam and oxymino-cephalosporins even in the presence of β-lactamase inhibitors. ESBL is derived from point mutation in genes like blaSHV and blaTEM and identified after the emergence of third-generation cephalosporins [6].
Bacterial species producing AmpC and MBL enzymes show significant resistance to cephamycins and carbapenams, respectively [7]. Carbapenamases can be found in Enterobacteriaceae in various forms including expanded-spectrum oxacillinases and clavulanic-acid inhibitors (β-lactamases or metallo-β-lactamases). Carbapenams (imipenem and meropenem) are considered as first line therapy for the treatment of severe infections caused by ESBLs producing Enterobacteriaceae [8].
The influence of antimicrobial agents leads microbes to constantly seek new protective strategies known as "resistive mechanisms''. For instance, some Enterobacteriaceae can release ESBLs. ESBL compounds separate and annihilate a few normally used antibiotics including penicillins and cephalosporins, making these medications insufficient to treat diseases [9, 10]. Rather than taking oral antimicrobial agents at home, patients with these diseases may require hospitalization and intravenous carbapenem therapy [11, 12].
According to Gerardo Alvarez-Uria, cephalosporin-resistant K. pneumoniae shows the greatest yearly rise in clean water accessibility related to AMR. AMR is associated with poor sanitation conditions and non-availability of clean water [13, 14]. As per previous studies, Klebsiella has the tendency to be resistant anywhere around the globe. So, there is a need to address the widespread use of antibiotics and follow the guidelines of WHO to mitigate the crisis related with beta-lactam-resistant Klebsiella spp. and focus on new interventions regarding its treatment [15, 16].
There is a huge difference in the resistance mechanism of children and the adult population. The resistance rates to other antimicrobial agents, such as ceftazidime, amikacin, imipenem, ciprofloxacin, and aztreonam are also different in adults and children [17, 18]. Studies on children are scarce. So, the prevalence of MDR Klebsiella and the detection of β-lactamase genes in children in Lahore is focused in the current study.
2. MATERIALS AND METHODS
2.1. Study DesignThis cross-sectional study was conducted from November 2021 to April 2022 at the Department of Microbiology, University of Child Health Sciences, The Children’s Hospital, Lahore, Pakistan in collaboration with the Lahore Garrison University. The isolates of Klebsiella spp. were included, while the isolates of other bacterial spp. were excluded.
2.2. Sample CollectionClinical samples of blood, urine, pus, and other fluids were received from The Children’s Hospital, Lahore, Pakistan. The samples were collected from different departments of the hospital including its surgical ward, neurosciences ward, as well as hematology, oncology, gastroenterology, cardiology, OPD, emergency and medical units. Among these samples, 73 were urine samples, 32 were blood samples, and 45 were pus swabs and other fluids. These samples were sent to the microbiology section of the hospital for analysis.
2.3. Isolation of Klebsiella Spp.The collected samples were processed by using different culture media such as blood, MacConkey and cystein lactose electrolyte deficient (CLED) agar. The cultures were kept overnight in an incubator at 37°C for the propagation of bacterial cultures. These bacterial cultures were grown on different media and identified by colony morphology, Gram staining, analytical profile index (API) testing and other biochemical tests. Pink, mucoid lactose fermenting colonies on MacConkey agar and yellow mucoid colonies on CLED agar were processed for further analysis.
The respective API test kit was selected and the sample was inoculated in each well of the kit. Each well was used to perform a specific test. After adding the sample and reagents in the strip, it was incubated. Post incubation, the results were checked and every test was assigned a numeric code. Then this code was matched with the API manual guidebook or through other API documentation software. In this way, the identity of the bacteria was determined and reported.
2.4. Antibiotic Susceptibility TestingKirby-Bauer disc diffusion method was used to determine the susceptibility and resistance profile of Klebsiella spp. Muller-Hinton agar media plates were used for the sensitivity test. McFarland 0.5 turbidity standard was followed to prepare a bacterial suspension and an equally distributed lawn of bacteria was made on the agar plate. Two agar plates were subjected to antibiotic discs using a disc dispenser (OXOID) and kept in incubator at 35±1°C overnight. The antibiotics discs used in the current study were cefoxitin, ceftazidime, cefepime, ceftriaxone, cefuroxime, imipenem, meropenem, gentamicin, amikacin, ciprofloxacin, cefotaxime, piperacillin-tazobactam, amoxicillin-clavulanate acid, cefoperazone, sulfamethoxazole, tobramycin, and levofloxacin. The zones of inhibition created by these discs were measured in mm. The isolated Klebsiella spp. were declared as resistant or susceptible according to the manual of Clinical and Laboratory Standards Institute (CLSI) 2009.
2.5. Phenotypic Screening of ESBL, MBL and AmpCThe clavulanate-induced activity enhancement of cefotaxime or ceftazidime indicated the presence of ESBL production. To detect ESBL production, CLSI confirmatory tests were performed by placing ceftazidime and cefotaxime alone and in combination with ceftazidime-clavulanate and cefotaxime-clavulanate respectively on inoculated Muller-Hinton Agar plates. For carbapenamases, the zones of inhibition produced by imipenem-EDTA discs and imipenem alone were compared after 16 to 18 hours of incubation at 35°C. The isolates were considered as MBL producers if the zone of inhibition created by imipenem + EDTA disc was measured as ≥ 5 mm. AmpC production was detected by 3-aminophenyl Boronic acid (APB) disk potentiation test, while 5μl of APB stock solution was added to cefotaxime (CTX), ceftazidime (CTZ), and cefoxitin (FOX) disks. An increase of ≥ 5mm in the zone of CTX and/or CTZ and/or FOX disk, either alone or in combination with APB was considered as a sign of AmpC production.
2.6. Identification of β-lactamase GenesMolecular identification of Klebsiella spp. was done by using polymerase chain reaction (PCR) test to detect ESBL, MBL and AmpC genes.
2.7. Statistical AnalysisDescriptive statistics were calculated and SPSS software was used.
3. RESULTS
In the current study, a total of 150 samples were processed in the Microbiology Laboratory of The Children’s Hospital, Lahore. On culturing, 150 strains were positive to bacterial infection. Of the 150 isolates, 58 (38.7%) were Klebsiella positive and the remaining 92 (61.3%) were positive to Escherichia coli, Acinetobacter spp., Pseudomonas aeruginosa, Proteus mirabilis, and Enterobacter spp. Gender-wise distribution indicated that 58.7% samples were collected from male and 41.3% were collected from female patients. Age-wise, Klebsiella infection was the most common in the age range of 6-10 years.
3.1. Macroscopic and Microscopic Characteristics of Klebsiella Spp.The texture of the growth was examined. There were large, grey-white, mucoid and non-hemolytic colonies on blood agar. While, yellow to bluish mucoid colonies were observed on CLED agar and pink colonies were visible on MacConkey agar (Figure 1).
3.2. Gram StainingIn Gram staining, the microscopic picture showed Gram-negative, rod shaped (bacilli), singly arranged and pink colour bacteria (Figure 2).

Figure 1. Colonies of Klebsiella spp. on Blood Agar, MacConkey Agar and CLED Agar
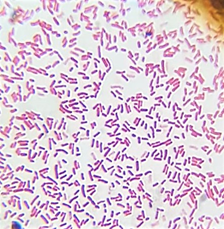
Figure 2. Gram Staining of Klebsiella spp. at 100X.
3.3. Biochemical Characteristics of Klebsiella Spp.Biochemical testing is the second step used by the scientists for the rapid identification of microorganisms based on their color production. The results of Simmon’s citrate test, urease and triple sugar iron (TSI) tests were positive, while the result of the indole test was mostly recorded as negative, although it may be positive for a few species of the bacteria (Figure 3).
3.4. API (Analytic Profile Index) TestingFurther specie-level identification of the bacterial colonies was performed by using the API test method. The scores for positive test results were added and the resulting seven-digit code was entered in an online API software. The picture below shows 20E API results for Klebsiella spp. Each mini-well of the API kit was incubated at 36°C. After incubation, the results were observed and a code was generated based on the biochemical reactions. Then, the code was noted for the identification of bacterial species. The identification manual or the API software was used for the confirmation of concern specie (Figure 4).

Figure 3. (A) Simmon’s Citrate Shows Positive Reaction (Blue Colour). (B) TSI (Triple Sugar Iron) Shows Positive Reaction (Yellow Colour). (C) Urease Test Shows Positive Reaction (Pink Colour). (D) MIO (Motility Indole Ornithine) Shows Negative Reaction After Adding 1 Drop of Kovac’s Reagent (No Pink-Coloured Ring Formation).

Figure 4. Positive Reactions of Klebsiella spp. on API Testing
3.5. Antibiotic Susceptibility TestingThe 58 samples of Klebsiella spp. were observed to show resistance as 95.5% against amoxicillin-clavulanate acid, 98.2% against ciprofloxacin, 3.44% against gentamicin, 3.44% against tobramycin, 1.8% against meropenem, 0% against imepenem, 1.8% against amikacin, 96.6% against ceftriaxone, 98.2% against piperacillin-tazobactam, 98.2% against levofloxacin, and 100% against ceftazidime, cefotaxime, sulfamethoxazole, cefoperazone, and cefepime (Figure 5). The antibiogram susceptibility pattern is shown below in Table 1.
Table 1. Antibiogram susceptibility pattern of Klebsiella spp.
|
Target Bacteria |
Antibiogram Disc |
Total No. of Isolates |
Disc Potency |
% |
M±SD |
V |
||
|---|---|---|---|---|---|---|---|---|
|
R |
I |
S |
||||||
|
Klebsiella spp. |
Ciprofloxacin |
58 |
5µg |
98.2 |
1.8 |
0 |
33.26 (55.18) |
2104.38 |
|
Amoxicillin-clavulanate acid |
10/20 µg |
95.5 |
1.5 |
0 |
32.22 (54.7) |
2993 |
||
|
Gentamicin |
10µg |
3.44 |
8.62 |
82.75 |
31.60 (44.36) |
1968.6 |
||
|
Tobramycin |
10µg |
3.44 |
0 |
96.6 |
33.34 (54.8) |
3003.6 |
||
|
Meropenem |
10µg |
1.8 |
3.44 |
94.8 |
33.34 (53.22) |
2833 |
||
|
Imipenem |
10µg |
0 |
0 |
100 |
0 (0) |
0 |
||
|
Amikacin |
10µg |
1.8 |
0 |
98.2 |
33.33 (56.18) |
3156.5 |
||
|
Ceftriaxone |
30µg |
96.6 |
3.41 |
0 |
33.33 (54.81) |
3004.5 |
||
|
Cefotaxime |
30µg |
100 |
0 |
0 |
0(0) |
0 |
||
|
Piperacillin-tazobactam |
100/10µg |
98.2 |
1.8 |
0 |
33.33 (56.18) |
3156.5 |
||
|
Ceftazidime |
30µg |
100 |
0 |
0 |
0 (0) |
0 |
||
|
Sulfamethoxazole |
23.75µg |
100 |
0 |
0 |
0 (0) |
0 |
||
|
Cefepime |
30µg |
100 |
0 |
0 |
0 (0) |
0 |
||
|
Levofloxacin |
5µg |
98.2 |
1.8 |
0 |
33.33 (56.18) |
3156.5 |
||
|
Cefoperazone |
30µg |
100 |
0 |
0 |
0 (0) |
0 |
||
Note. V= Variance Coefficient, R= resistant, I= intermediate, S= sensitive
3.6. ESBL Confirmatory TestTo detect ESBL production, CLSI confirmatory tests were performed by placing ceftazidime and cefotaxime on inoculated Muller-Hinton agar plates. The CLSI test, performed using a combination of discs, was interpreted as ESBL positive when the zone of inhibition was observed as ≥5 mm. A total of 12 (20.7%) isolates were positive for ESBL and 46 (79.3%) isolates were negative (Figure 6).

Figure 5. (A) Antimicrobial Susceptibility Testing of Klebsiella spp., in Which All the Antibiotics are Resistant (B) In Which Some Antibiotics are Resistant and Some are Sensitive. (C) In Which All the Antibiotics are Sensitive

Figure 6. ESBL Confirmatory Test. A Key-Hole Effect is Produced
3.7. MBL Confirmatory TestThe zones of inhibition created by imepenem-EDTA discs and imepenem alone were observed and compared after 16 to 18 hours of incubation at 35°C. The isolates were presumed as MBL producers if the zone of inhibition created by the imepenem + EDTA disc was measured as ≥ 5 mm, as shown in Figure 7. A total of 11 (19.0%) isolates were positive for MBL and 47 (89.0%) isolates were negative.
3.8. AmpC Confirmatory TestAn increase in the diameter of the zone of inhibition of about ≥ 5mm for cefoxitin (FOX) disk alone and in combination with APB was documented and considered as indicative of AmpC production, as shown in Figure 8. A total of 20 (34.5%) isolates were positive for AmpC and 38 (65.5%) isolates were negative.

Figure 7. (A) Imipenem Alone, the Zone is Resistant. (B) Imipenem + EDTA, the Zone Size Increases upto ≥ 5 mm.

Figure 8. (A) Cefoxitin Alone, the Zone is Resistant. (B) Cefoxitin + APB (3-Aminophenyl Boronic Acid), the Zone Size Increases upto ≥ 5 mm
3.9. Identification of β-lactamase GenesMultigene optimax thermal cycler (Labnet, USA) was used to perform the PCR test to detect the drug resistant gene in the isolated DNA. All the Klebsiella spp. samples were processed at the Department of Microbiology, University of Child Health Sciences, The Children’s Hospital, Lahore. The results showed the presence of the resistive gene. The desired samples were analyzed for the detection of ESBL, MBL and AmpC genes with primers shown in Table 2.
Table 2. Sequences of different genes
|
Primers |
Sequences |
Temp. (°C) |
Amplicon Size (bp) |
|---|---|---|---|
|
NDM |
ATGGAATTGCCCAATATTATG CACTCAGCGCAGCTTGTCGGC |
66 |
813 |
|
TEM |
GAGTATTCAACATTTCCGTGTC TAATCAGTGAGGCACCTATCTC |
62 |
800 |
|
SHV |
ATGCGTTAT ATTCGCCTGTG TTAGCGTTGCCAGTGCTC |
60 |
867 |
|
CTX-M |
GCGTGATACCACTTCACCTC TGAAGTAAGTGACCAGAATC |
60 |
300 |
4. DISCUSSION
In this study, 58 strains of Klebsiella species were isolated from 150 clinical samples and tested for the production of different types of β-lactamases, such as ESBL, MBL, and AmpC enzymes. Out of these 58 isolates, 43 (74.1%) were found to be resistant because of β-lactamase enzymes, while 15 (25.9%) were not resistant. The same study conducted at Babol University of Medical Sciences revealed a slightly lower prevalence of resistant strains with β-lactamase enzymes equivalent to 64.4% of the Klebsiella spp. isolates [19]. In the year 2010, the prevalence of the resistant strains of Klebsiella because of β-lactamase was reported as 64.1%, which increased to 74.1% in 2021, highlighting the increasing trend of AMR globally.
The high prevalence of this resistant strain emphasizes the upcoming threat in terms of difficulty in treating patients. The presence of resistant genes detected on a molecular level in this study confirmed its alignment with the global trends. The prevalence of resistant genes suggests the limited options left in terms of antibiotic selection for treatment, which is a growing challenge in the management of diseases.
This study highlights the need to focus on the prevention of medication overuse, self-medication and the reduction of environmental factors involved in exacerbating the spread of AMR. It also highlights other genetic factors involved in the horizontal transfer of AMR, all of which eventually contribute in the persistence and dissemination of resistance gene within the community. Moreover, to reduce or combat the increasing threat of AMR, surveillance and monitoring mechanisms are needed to track the evolution and spread of resistant genes along with the rising trend of antibiotic consumption.
The greater presence of Klebsiella spp. in urine than blood or pus corresponds with the findings of previous studies. These studies showed that the pathogenic bacteria target sites are specific and the probability to find the pathogen exceeds if the right sample is collected from the right place.
In the current study, phenotypic detection showed the frequency of ESBL gene equal to 12 (20.7%), MBL gene equal to 11 (19.0%) and AmpC gene equal to 20 (34.5%), among all positive cultures. A similar study conducted at the Aga Khan Hospital on ESBL containing AMR showed 7.2% ESBL containing Klebsiella among all the positive samples of enterobacteriacae. While the current study found 27.9% ESBL among all positive samples of Klebsiella antimicrobial resistant strains. In another study conducted in Lahore, 26.1% of the clinical samples tested positive for ESBL-producing Klebsiella spp. This shows a significant prevalence of the antibiotic-resistant bacteria in the area, which is a cause for concern in terms of healthcare and antimicrobial resistance [20].
In the current study, the co-existence of enzymes was checked. It was found that 2 (4.6%) isolates co-produced MBL+ESBL, followed by 1 (2.3%) that co-produced AmpC+ESBL, and 1 (2.3%) that co-produced AmpC+MBL. All of the three enzymes were present in 1 (2.3%) Klebsiella isolate. Another study also confirmed the co-production of these enzymes in 20.87% of enterobacteriacae isolates. It mentioned that among the isolates tested, approximately 20.87% were found to produce all three types of enzymes simultaneously [21]. This co-existence of multiple antibiotic resistance mechanisms in the same bacterial isolate is a matter of concern because it might contribute in increasing the resistance of these particular bacteria, limiting treatment options and increasing the risk of infections that are difficult to control. It also emphasizes the importance of prudent antibiotic use and continued research into new antibiotics and alternative treatment strategies. In most of the studies, the co-production of ESBL and AmpC was noticed [22, 23].
Various genes in β-lactamases were detected on the basis of the molecular analysis that showed the three genes of ESBL, namely SHV (41.6%), CTX-M (25.0%), and TEM (8.3%). These results are comparable with previous studies. A study conducted in Iraq showed a high prevalence of SHV gene (86.04%) for ESBL production [24]. The presence of genes in AmpC producing Klebsiella spp. strains from another study indicates, 35.2% of strains had the CIT gene and 61.7% had the EBC gene. It's important to note that the prevalence of specific genes in bacterial populations can vary based on several factors, including geographic location, time period, and the specific methods used for detection and analysis [25].
Another study found the gene NDM-1 β-lactamase producing bacteria in environmental samples. There are implications of this finding for the health of people relying on public water and public sanitation facilities. The prevalence of NDM-1 β-lactamase in this study also highlights the probability of finding these bacteria in environmental samples, including public water and sanitation facilities. Furthermore, international surveillance of clinical isolates and environmental samples also needs to be conducted [26].
4.1. Conclusion
In developing countries like Pakistan, antibiotic resistance has reached alarming levels. The effect of antibiotics is inhibited by various resistance mechanisms developed by the bacteria. This study revealed clinical, molecular, laboratory, and demographic features of MDR Klebsiella spp., the co-existence of enzymes and the presence of various β-lactamases, all of which is helpful for clinicians to better judge the clinical scenarios and make recommendations for the selective use of antibiotics. A significant prevalence of MDR Klebsiella among children highlights the poor dose management of antibiotics by patients and a weakened immune system. Hence, there is a need to improve the hygiene of children and encourage the lesser use of medication for minor complaints. To prevent the spread of resistant strains, specific targeted antimicrobial agents need to be used. Out of the 43 MDR Klebsiella samples, 5 showed more than 1 enzyme’s activity. This indicates the potential complexity of resistance mechanisms, highlighting the need of stringent monitoring and a targeted therapeutic line of action.
4.2.Policy Implications
Collaboration between healthcare facilities, researchers, and policymakers is necessary to develop and implement strategies that can help mitigate the antibiotic resistance crisis. This may include promoting antibiotic stewardship programs, investing in research for new antibiotics, and enhancing infection prevention and control measures in healthcare settings. For the successful treatment of patients, β-lactamases should be detected and reported as early as possible. Moreover, a proper surveillance system is also needed for impeding antibiotic resistance.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Koirala S, Khadka S, Sapkota S, Sharma S, Kandel S, Ghimire A, Thapa B. Prevalence of CTX-M β-lactamases producing multidrug resistant Escherichia coli and Klebsiella pneumoniae among patients attending Bir hospital, Nepal. Biomed Res Int. 2021;2021:9958294. https://doi.org/10.1155/2021/9958294
- Wyres KL, Lam MM, Holt KE. Population genomics of Klebsiella pneumoniae. Nat Rev Microbiol. 2020;18(6):344–359. https://doi.org/10.1038/s41579-019-0315-1
- Pal M, Kerorsa GB, Marami LM, Kandi V. Epidemiology, pathogenicity, animal infections, antibiotic resistance, public health significance, and economic impact of Staphylococcus aureus: a comprehensive review. Am J Public Health Res. 2020;8(1):14–21. https://doi.org/10.12691/ajphr-8-1-3
- Yang J, Long H, Hu Y, Feng Y, McNally A, Zong Z. Klebsiella oxytoca complex: update on taxonomy, antimicrobial resistance, and virulence. Clin Microbiol Rev. 2022;35(1):e00006-21. https://doi.org/10.1128/CMR.00006-21
- Russo A, Fusco P, Morrone HL, Trecarichi EM, Torti C. New advances in management and treatment of multidrug-resistant Klebsiella pneumoniae. Expert Rev Anti Infect Ther. 2023;21(1):41–55. https://doi.org/10.1080/14787210.2023.2151435
- Gharavi MJ, Zarei J, Roshani-Asl P, Yazdanyar Z, Sharif M, Rashidi N. Comprehensive study of antimicrobial susceptibility pattern and extended spectrum beta-lactamase (ESBL) prevalence in bacteria isolated from urine samples. Sci Rep. 2021;11(1):578. https://doi.org/10.1038/s41598-020-79791-0
- Roy S, Chowdhury G, Mukhopadhyay AK, Dutta S, Basu S. Convergence of biofilm formation and antibiotic resistance in Acinetobacter baumannii infection. Front Med. 2022;9:793615. https://doi.org/10.3389/fmed.2022.793615
- Asempa TE, Abdelraouf K, Nicolau DP. Metallo-β-lactamase resistance in Enterobacteriaceae is an artefact of currently utilized antimicrobial susceptibility testing methods. J Antimicrob Chemother. 2020;75(4):997–1005. https://doi.org/10.1093/jac/dkz532
- Onduru OG, Mkakosya RS, Aboud S, Rumisha SF. Genetic determinants of resistance among ESBL-producing Enterobacteriaceae in community and hospital settings in east, central, and Southern Africa: a systematic review and meta-analysis of prevalence. Can J Infect Dis Med Microbiol. 2021;2021:5153237. https://doi.org/10.1155/2021/5153237
- Tao S, Chen H, Li N, Wang T, Liang W. The spread of antibiotic resistance genes in vivo model. Can J Infect Dis Med Microbiol. 2022;2022:3348695. https://doi.org/10.1155/2022/3348695
- Osman EA, Yokoyama M, Altayb HN, Elbadwi HS, Hassan SS, Nagm Eldin AA, Elamin BK, Ibrahim NA, Ahmed MAA, Elkhidir IM, Elnosh MMA, Saeed A. Klebsiella pneumoniae in Sudan: multidrug resistance, polyclonal dissemination, and virulence. Antibiotics. 2023;12(2):233. https://doi.org/10.3390/antibiotics12020233
- Ibrahim ME. Risk factors in acquiring multidrug-resistant Klebsiella pneumoniae infections in a hospital setting in Saudi Arabia. Sci Rep. 2023;13(1):11626. https://doi.org/10.1038/s41598-023-38871-7
- Lam MM, Wick RR, Watts SC, Cerdeira LT, Wyres KL, Holt KE. A genomic surveillance framework and genotyping tool for Klebsiella pneumoniae and its related species complex. Nat Commun. 2022;12(1):4188. https://doi.org/10.1038/s41467-021-24448-3
- Salam MA, Al-Amin MY, Salam MT, Pawar JS, Akhter N, Rabaan AA, Alqumber MAA. Antimicrobial resistance: a growing serious threat for global public health. Healthcare. 2023;11(13):1946. https://doi.org/10.3390/healthcare11131946
- Jian Z, Zeng L, Xu T, Sun S, Yan S, Huang L, Tang Y, Wu X, Huang X. Antibiotic resistance genes in bacteria: occurrence, spread, and control. J Basic Microbiol. 2021;61(12):1049–1070. https://doi.org/10.1002/jobm.202100201
- Wood SJ, Kuzel TM, Shafikhani SH. Pseudomonas aeruginosa: infections, animal modeling, and therapeutics. Cells. 2023;12(1):199. https://doi.org/10.3390/cells12010199
- Zhou J, Song S, Xue S, Zhu Y, Xu B, Ma J, Chen J, Chen J, Huang M. Study of the epidemiological and mechanistic differences between carbapenem-resistant Klebsiella pneumoniae infections in children and adults. Infect Drug Resist. 2024;17:2625–2639. https://doi.org/10.2147/IDR.S466054
- Salawudeen A, Raji YE, Jibo GG, Desa MNM, Yee LC, Mohidem NA, Musa NA, Yusof N, Mat Azis N, Ibrahim N. Epidemiology of multidrug-resistant Klebsiella pneumoniae infection in clinical setting in South-Eastern Asia: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2023;12:142. https://doi.org/10.1186/s13756-023-01346-5
- Ma J, Gao K, Li M, Zhang X, Wang Y, Ma J, Zhao J, Liu Y, Liu Y, Wang Q. Epidemiological and molecular characteristics of carbapenem-resistant Klebsiella pneumoniae from pediatric patients in Henan, China. Ann Clin Microbiol Antimicrob. 2024;23:98. https://doi.org/10.1186/s12941-024-00757-5
- Moussa M, Chakra MA, Dellis A, Moussa Y, Papatsoris A. Pharmacotherapeutic advances for recurrent urinary tract infections in women. Expert Opin Pharmacother. 2020;21(16):2011–2026. https://doi.org/10.1080/14656566.2020.1795128
- Junaid K, Ejaz H, Asim I, Younas S, Yasmeen H, Bukhari SAA, Qamar MU. Heavy metal tolerance trend in extended-spectrum β-lactamase encoding strains recovered from food samples. Int J Environ Res Public Health. 2021;18(9):4718. https://doi.org/10.3390/ijerph18094718
- Shahzad S, Willcox MD, Rayamajhee B. A review of resistance to polymyxins and evolving mobile colistin resistance gene (mcr) among pathogens of clinical significance. Antibiotics. 2023;12(11):1597. https://doi.org/10.3390/antibiotics12111597
- Ababu A, Endashaw D, Fesseha H. Isolation and antimicrobial susceptibility profile of Escherichia coli O157:H7 from raw milk of dairy cattle in Holeta District, Central Ethiopia. Int J Microbiol. 2020;2020:6626488. https://doi.org/10.1155/2020/6626488
- Srinivash M, Krishnamoorthi R, Mahalingam PU, Rajendran M, Nithyanandam S, Selvaraj P, Kaliyaperumal V. Nanomedicine for drug resistant pathogens and COVID-19 using mushroom nanocomposite inspired with bacteriocin—a review. Inorg Chem Commun. 2023;152:110682. https://doi.org/10.1016/j.inoche.2023.110682
- Janda JM, Abbott SL. The changing face of the family Enterobacteriaceae (order: “Enterobacterales”): new members, taxonomic issues, geographic expansion, and new diseases and disease syndromes. Clin Microbiol Rev. 2021;34(2):e00174-20. https://doi.org/10.1128/CMR.00174-20
- Aslam B, Khurshid M, Arshad MI, Muzammil S, Rasool M, Yasmeen N, Shah T, Chaudhry TH, Rasheed MK, Shahid A, Li X, Ma X, Fatima S, Ali MA, Haque A, Baloch Z. Antibiotic resistance: one health one world outlook. Front Cell Infect Microbiol. 2021;11:771510. https://doi.org/10.3389/fcimb.2021.771510