Impact of Parental Vaccination Status on Yellow Fever Vaccination in Children Aged 0–1 Years in the Democratic Republic of Congo: Mixed Sequential Explanatory Study
Abraham Mukongo Bulaimu Lukeba1,2*, Gerard Eloko Eya Matangelo1,Simon- Decap Mabakutuvangilanga Ntela22,3, Monique Rothan-Tondeur2,4,and Rita Georges Nohra2,5
1Section of Public Health, Medical Technical College of Kinshasa (ISTM-Kinshasa), Democratic Republic of Congo
2Nursing Sciences Research Chair, Education and Health Promotion Laboratory, LEPS, Sorbonne Paris North University,
Villetaneuse, France
3Section of Nursing Sciences, Medical Technical College of Kinshasa (ISTM-Kinshasa), Democratic Republic of Congo
4Public Hospitals Assistance of Paris (AP-HP), Nursing Sciences Research Chair, Paris, France
5Department of Nursing Sciences, Paris Cité University, ECEVE, INSERM, National Institute of Health and Medical Research, Paris, France
ABSTRACT
Background. Yellow fever occurs in the intertropical regions of Africa and South America. Vaccination is a simple, effective, and inexpensive means to reduce morbidity and mortality from infectious diseases. Presently, the world is witnessing a decrease in the number of children vaccinated each year in low-income countries and in the Democratic Republic of the Congo (DRC). This scenario is leading towards concrete consequences and even a resurgence of vaccine-preventable infectious diseases.
Methodology. This is a sequential and explanatory study conducted using a mixed-method approach. The quantitative component, of the retrospective, multicenter, analytical type, was carried out using data from the post-campaign yellow fever coverage study in 8 concerned provinces. Whereas the qualitative component, of the descriptive phenomenological type, was carried out through semi-directive interviews held with the heads of household of children aged 0–1 year in Tshuapa Province. Quantitative data was analyzed using SPSS (version 25) and qualitative data was analyzed using ATLAS-Ti 22 software.
Results. Quantitative analysis showed that there was a statistically significant influence of the household head's vaccination status on the routine vaccination of children aged 0–1 year, with a chi-square test indicating χ2 = 62.706 and p = 0.000. This means that children whose parents are immunized are more likely to be immunized as well. Despite this positive influence, the study revealed that 27.7% of immunized children had parents who were themselves immunized. This figure raises concerns about the effectiveness of awareness campaigns and parental decision-making on immunization. Qualitative analysis highlighted several factors influencing parental decision to vaccinate including parents' knowledge of vaccination, their positive experiences with it, and their sense of parental responsibility.
Conclusion. These results highlight not only the importance of household heads' vaccination status in the child immunization process, but also the need to address concerns related to immunized children, even in households where parents are immunized. Therefore, national authorities must develop effective strategies to improve immunization coverage and raise family awareness regarding the importance of vaccination.
- The current study attempted to close the data gap on the spread of yellow fever virus in the Democratic Republic of the Congo (DRC), revealed by the World Health Organization's (WHO’s) Weekly Epidemiological Record for 2021.
- In order to eradicate or reduce yellow fever outbreaks in the DRC to zero, the current study participated to educate and enlighten the Congolese population about the significance to understand routine EPI and yellow fever vaccination.
- The current study focused to strengthen the Expanded Program on Immunization (EPI) of the DRC by assisting the dissemination of information on altering household heads' and parents' behavior in order to guarantee vaccination of their children.
GRAPHICAL ABSTRACT
1. INTRODUCTION
Yellow fever is an acute viral hemorrhagic disease transmitted by the bite of an infected wild, domestic or semi-domestic mosquito of the genus Aedes (or Hemagogus or Sabethes from South America). This disease is prevalent in the intertropical regions of Africa and South America [1][2]. According to WHO’s estimates, each year, there are at least 200,000 cases of yellow fever and 30,000 deaths due to this epidemic worldwide [3]. As of early 2024, the WHO detailed that 13 nations in Africa have reported affirmed or plausible cases of yellow fever [4][5]. In addition, the WHO has raised concerns regarding the potential for yellow fever to spread in 13 nations in South and Central America, where conditions may permit widespread transmission [6].
Vaccination is the oral, intradermal or scarification administration of a vaccine into the body of a living organism, for preventive or curative purposes [7]. It is also defined as a method to prevent certain bacterial, viral or parasitic diseases by developing active immunity through the introduction of a vaccine into the body via oral or parenteral route [8]. Thus, the aim of vaccination is to prevent or restrict the onset of certain bacterial, viral or parasitic diseases by injecting a small quantity of pathogenic agent into a healthy organism in order to promote the development of immune cells.
Vaccination safely eliminates and controls life-threatening infectious diseases, preventing between 2 and 3 million deaths per year [2]. It is among the most cost-effective health investments, with proven strategies that are accessible to the most vulnerable and hard-to-reach populations [2]. WHO recommends through the EPI that all children be immunized before their first birthday against tuberculosis, diphtheria, pertussis, tetanus, polio, measles, hepatitis B, Haemophilus influenzae type b, pneumococcus, measles, and rubella, as well as in countries affected by yellow fever [9].
WHO's Program for Immunization 2030 aims at reducing yellow fever outbreaks to zero by 2026 [10]. For national coverage, the Ministry of Public Health, Hygiene, and Prevention of the DRC and government partners (GAVI, WHO, UNICEF, PATH) planned to organize yellow fever preventive campaigns targeting individuals from 9 months to 60 years old, in 5 blocks of provinces, the first two of which took place between April 2021 and January 2022. The DRC is currently classified as an active outbreak country according to the WHO’s Epidemiology Report 2022 [11].
However, there is still a decrease in the number of children vaccinated each year in low-income countries and in the DRC, leading to concrete consequences and even a resurgence of vaccine-preventable infectious diseases [12][13][14]. Hence, based on the results of the yellow fever preventive campaigns in the DRC, the study aimed to explore and understand how the vaccination status of the household head or the custodian mother influences the routine vaccination of her children.
2. METHODOLOGY
This is a sequential and explanatory study involving a retrospective quantitative analytical analysis, followed by a qualitative study using the descriptive phenomenological approach. The results were used for the campaign conducted in 8 provinces to explore the relationship between the immunization status of the household head and/or the custodian mother as well as the routine immunization of children from 0–1-year-old.
The study involved households in provinces that had experienced the organization of the yellow fever preventive campaign during the period from April 2021 to January 2022, namely: Bas-Uele, Equateur, Haut-Uele, Mongala, Nord-Ubangi, Sud-Ubangi, Tshopo, and Tshuapa. The target population comprised the heads of household/caretaker and mother/guardian, who responded to the question about routine vaccination of their infants in each province concerned with yellow fever vaccination. The sample size consisted of data collected from 8 provinces of the DRC concerned by this study and beneficiaries of post-campaign coverage against yellow fever. This included 2224 heads of household/caretakers/guardians with at least a child aged 0–12 months drawn from the database of 16,344 individuals.
The variables of interest in the quantitative study were gender, age, province, vaccination status of the head of household/caretaker mother, and vaccination status of children in routine EPI. Their operational definitions are mentioned as follows:
Gender: Nominal variable (male/female).Age: Continuous variable (numeric), determining vulnerability to disease, as immune systems vary with age. Infants, young children, and elderly people are more susceptible to infection.
Province: Nominal variable (province name), any DRC province that benefited from the mass yellow fever vaccination campaign between April 2021 and January 2022.
Vaccination Status of Head of Household/Caretaker Mother: A nominal categorical variable (vaccinated/not vaccinated), which may influence children's vaccination decisions. Additionally, this may also serve as an indicator of health awareness and access to vaccination services in a household.
Vaccination Status of Children in Routine EPI: Nominal categorical variable (vaccinated/non-vaccinated), combined vaccination with yellow fever vaccine, and measles being the last vaccine to be given to children under one year of age according to the DRC vaccination calendar. Vaccinated means fully vaccinated in the context of this study.
2.1. Hypothesis
H0: The vaccination status of heads of household or custodial mothers has no positive or negative impact on the vaccination status of their children.H1: The vaccination status of heads of households or custodial mothers would have a positive or negative impact on the vaccination status of their children.
2.2. Processing and Analysis of Quantitative Data
2.2.1. File Cleaning and Data Processing. Prior to analysis, data processing was carried out at three levels:
- synchronization of the data of each head of household/caretaker/mother and her child.
- cleaning of the data concerning children whose head of household/caretaker/mother was under 14 years old and deletion of duplicates, and
- extraction of the database corresponding to the research question.
2.2.2. Data Analysis Method. The database in Excel was exported to SPSS 25® for statistical analyses. Afterwards, a triangulation of result was conducted using SPSS and R software by another researcher to determine the validity of the latter.
The chi-square test was used to verify the relationship between the vaccination status of heads of household/custodian mother on the routine vaccination of their children.
The choice of chi-square test in this study was motivated by the nature of data (the two variables are categorical and binary). In this study, the null hypothesis stated that there was no association between the vaccination status of the head of household and that of children. This fits in well with the research objective, which was to establish a direct relationship without involving other variables and without concern for the principle of cause and effect by seeking to model.
2.3. Qualitative Component
The qualitative component is a descriptive phenomenological study that allowed to explore the lived experiences of the participants on routine EPI vaccination of children from 0–12 months. This was done by observing and describing the meaning attributed to their experiences of immunization from birth [15][16][17][18][19][20][21]. The qualitative part of the study was conducted by holding interviews with heads of households in the Province of Tshuapa. This province was chosen due to its proximity to 8 provinces, its resources, and knowledge of the field. The target population comprised heads of households/caretakers/guardians who agreed to participate in individual semi-structured interviews (SSI) on the importance of routine EPI vaccination of infants (aged 0–1 year). Purposive non-random sampling was done to capture the experiences of heads of households or custodial mothers in Tshuapa Province who voluntarily agreed to participate in this study in order to learn about their experiences with routine immunization as well as yellow fever vaccination. Participants were recruited using a snowball method. First two days were utilized to identify participants and schedule appointments. The remaining days were reserved for interviews.
Data was collected through semi-structured interviews using an interview guide (Table 3). Faced with the difficulty of getting to the participants' respective homes, new information technology tools were used, in particular WhatsApp video calls with 3 smartphones, one of which was used by a facilitator to film the interviewee, two of which were used by the principal investigator (one to exchange information from a distance while collecting gestures, emotions, and pauses; and the other was used as a recorder to facilitate the post-interview auditions).
The appointments were scheduled by the facilitator who briefed the participants on the inclusion and non-inclusion criteria as well as presented free and informed consent form to the participants for signature. The analysis of the qualitative data was done with the Atlas.ti 22® software. The data analysis was based on Giorgi's method, which proposed four steps to guide in the analysis [15][20][22]. These steps are as follows:
- Listening the entire audios to get an idea of the whole situation
- Delimitation of the units of meaning
- Coding of meaning units into sensible statements of their lived experiences
- Categorization of meaning units to allow for a good synthesis
The rationale behind choosing phenomenology in this study is as follows:
Individual-centered Approach: Phenomenology was chosen over other qualitative methods, such as grounded theory, because it allows for deeper immersion in the participants' lived experiences. Grounded theory often focuses on developing theories from data, which may sometimes downplay the importance of individual experiences. Phenomenology, on the other hand, aims to understand how parents experience and interpret their reality, which is crucial when tackling sensitive subjects, such as vaccination.
Contextual Relevance: In the specific context of yellow fever vaccination in the DRC, it is essential to understand not only the decisions made, however, also the emotions and beliefs that underpin these decisions. Phenomenology has enabled the exploration of emotional and cultural dimensions, offering an enriched perspective that can guide public health interventions.
The use of phenomenological approach in this study strengthened the understanding of parental vaccination decisions by focusing on lived experiences and providing a rigorous analysis that values the voice of participants. This methodological choice was particularly suited to addressing complex public health issues in a specific cultural context. A second analysis of the data was conducted by a team of two researchers, with the objective of triangulation. The application of data triangulation by a second team of researchers for this study was an essential methodological process to ensure the validity and reliability of results.
This final guide contains the questions that guided the interviews (each interview began with a reminder of consent, followed by a greeting, and ended with a thank you for participating)
Table 1. Individual Semi-Directive Interview Guide| Objectives | Questions | Booster Questions |
|---|---|---|
| Collect socio-demographic data | Can you introduce yourself? |
|
| Collect Yellow Fever vaccine data |
Are you vaccinated against Yellow Fever? |
|
| Understand the importance or role of routine EPI vaccination and who influences this vaccination |
Why do we vaccinate babies? |
|
| Know the level of knowledge about Yellow Fever |
Do you know the yellow fever disease ? |
|
| Get the knowledge on the Immunization Schedule |
How are you tracking your child's immunizations ? |
|
| To have the proposals and suggestions | What advice can you give to other parents and caregivers? |
|
2.4. Data Triangulation
Triangulation Process: Triangulation was achieved by involving a team of two researchers who carried out a second analysis of the qualitative data. This made it possible to compare the results initially obtained by the team, thus reinforcing the robustness of the conclusions drawn. This was particularly useful to determine the consistency and completeness of the data, ensuring that interpretations were not biased by the perspectives of a single analyst.
Cross-checking: The codes and categories resulting from the initial analysis were subjected to a cross-checking process between the two teams. This process identified and validated the emerging themes, ensuring that participants' lived experiences were accurately represented and interpreted. By comparing the analyses, the researchers were able to discuss potential discrepancies in data interpretation.
2.5. Resolution of Discrepancies
Resolution Methods: In the event of discrepancies between the two teams' analyses, several strategies were implemented. Meetings were organized between the two research teams to discuss differences in interpretation and to explore the underlying reasons for these discrepancies. These collaborative discussions helped refine the codes and categories, resulting in a synthesis that more accurately reflected the participants' lived experiences.
Final Consensus: The aim was to reach consensus on the final interpretations, which not only strengthened the methodological rigor of this study, however, also enriched the understanding of factors influencing yellow fever vaccination. This collaborative process made it possible to integrate different perspectives, increasing the depth and richness of results.
Finally, data triangulation by a second team of researchers played a vital role in improving the validity and reliability of the vaccination study results.
The cross-checking of codes and categories, as well as the collaborative resolution of discrepancies ensured that the conclusions were based on a rigorous and comprehensive analysis of parents' experiences of their children's yellow fever vaccination.
2.6. Ethical Aspects
This study was carried out after the approval of the National Health Ethics Committee of the DRC (n°398/CNES/BN/PMMF/2022 of 05/10/2022). A free and informed consent form explaining the purpose, confidentiality, and voluntary participation was presented to the participants. The data collected during this study remained strictly confidential and did not mention the names of the participants.
The individual interviews and guide were completely anonymous and a code was assigned to each participant upon inclusion in the study (P1, P2, through Pn).
The conversations were recorded and then anonymized. The recordings were only heard by the principal investigator in charge of the study and were destroyed after hearing. The identities of participants were never revealed.
3. RESULTS
Total Population: A total of 16,344 individuals participated in the survey of yellow fever vaccination coverage in 8 provinces of the DRC between April 2021 and January 2022.
Heads of Households Sample: Among this population, 2,224 were heads of household or custodial mothers with at least one child aged 0-12 months. Of this population, 55% were females and approximately 45% were males. The average age of the heads of households/caretakers was 33±11.50 years. The provinces with the highest number of heads of households/caretakers with babies waiting for their first birthdays were Equateur with 27%, Haut Uele 19% followed by Tshopo 16% (Table 2).
Regarding the vaccination status of the heads of households or custodial mothers in 8 provinces covered by the study, 78.5% of the heads of households or custodial mothers in 8 provinces were vaccinated and 21.5% were not (Table 2). For the vaccination status of children in routine EPI, 68.2% of children in 8 provinces were regularly vaccinated in routine EPI and about 31.8% did not follow routine vaccination (Table 2). The evaluation of relationship between the immunization status of heads of households and/or custodial mothers and the routine immunization of infants in 8 provinces targeted by this study informed that 53.2% of children with their custodial mother as the head of household who was not immunized were immunized. It should also be noted that 27.7% of unvaccinated children were heads of households or vaccinated custodial mothers (Table 3). However, the results showed that there was a relationship between the immunization status of the heads of households or custodial mothers and routine EPI immunization (72.3%) (Table 3). This relationship is statistically significant. This is because the analysis showed a significant relationship between the vaccination status of the heads of households or custodial mothers and the regular immunization of children, with a chi-square test indicating χ2=62.706 and p=0.000. Consequently, these results showed that the null hypothesis was not accepted (H0). The alternative hypothesis (H1) was accepted. Therefore, there is a statistically significant relationship between vaccination of the heads of households or custodial mothers and routine EPI vaccination (Table 3).
Table 2. Results of the Descriptive Analysis of Quantitative Data|
Variables |
Frequency (N=2224) |
Percent % |
M |
SD |
|
|---|---|---|---|---|---|
|
Sex of |
Female |
1227 |
55.2 |
||
|
Male |
997 |
44.8 |
|||
|
Age |
33.45 |
11.50 |
|||
|
Province |
Bas Uele |
297 |
13.4 |
||
|
Equateur |
600 |
27.0 |
|||
|
Haut Uele |
424 |
19.1 |
|||
|
Mongala |
229 |
10.3 |
|||
|
Nord Ubangi |
267 |
12.0 |
|||
|
Sud Ubangi |
30 |
1.3 |
|||
|
Tshopo |
349 |
15.7 |
|||
|
Tshuapa |
28 |
1.3 |
|||
|
Vaccination status of Head of Household or Custodian Mother |
Vaccinated |
1745 |
78.5 |
||
|
Not Vaccinated |
479 |
21.5 |
|||
|
Vaccination status of EPI child routine |
Vaccinated |
1516 |
68.2 |
||
|
Not Vaccinated |
708 |
31.8 |
|||
|
|
vaccination for children 0-1 year old |
Total |
x2 |
p |
||
|---|---|---|---|---|---|---|
|
Vaccinated |
Not Vaccinated |
|||||
|
immunization status head |
Vaccinated |
1261 (72,3%) |
484 (27,7%) |
1745 (100%) |
62.706 |
0.000 |
|
Not Vaccinated |
255 (53,2%) |
224 (46,8%) |
479 (100%) |
|||
|
Total |
1516 (68,2%) |
708 (31,8%) |
2224 (100%) |
|||
3.1. Study Population
A total of 10 custodial mothers from Tshuapa Province, with a child aged 0-12 months, voluntarily agreed to participate in individual SSIs for this study during the period October 6-11, 2022. Of the 10 participants, only one was a grandmother (custodian of the child) and the other 9 were mothers of their children. Two mothers had a university education and one was still pursuing university education. Half of the participants were not employed and all interviews were conducted in the participants' homes.
All custodial mothers were vaccinated and 6 out of 10 children were fully vaccinated including yellow fever vaccination. Moreover, 2 children were partially vaccinated due to their age (less than 9 months), 2 children were not fully vaccinated and were waiting for the last measles and yellow fever vaccines to be caught up. The age of custodial mothers ranged from 19-49 years and the average age was 30±10.55 years.
3.2. Emerging Themes
From the analysis of interviews of 10 study participants, the main themes that emerged were as follows (Figure 1).
Figure 1Themes and Codes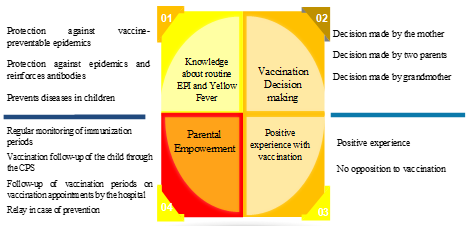
3.2.1. Knowledge about Routine EPI and Yellow Fever VaccinationThe majority of participants emphasized routine EPI vaccination and recognized that vaccination protects against vaccine-preventable epidemics, as indicated by some of the verbatims:
- P5: “The vaccine is necessary.”
- P3: “I know the importance of vaccination, it allows to protect the child against diseases that can attack them.”
- P1: “Children are vaccinated according to their age in order to prevent them from being hit by future epidemics.”
- P9: “So, um, it's just for protection.”
- P10: “Vaccination protects the children against Tetanus. It keeps the family and the child safe.”
Two custodial mothers did not have sufficient information about vaccination and were dubious about the importance of routine child immunization.
Following the content of interview hearings, half of the participants showed some symptoms of yellow fever that they remembered:
- P2: “Fever, fatigue, yellow hands, yellow urine.”
- P6: “I know about yellow fever. In our country we call it Hepatitis, its symptoms are the yellow color of eyes, yellow urine, and the whole body of the child can become yellow too.”
- P1: “Yes, I was vaccinated. I know the yellow fever disease, the eyes are colored, the whole body is also colored.”
- P10: “The eyes become yellow. I forgot the rest of the signs.”
In hearing participant interviews, two custodial mothers indicated that they did not know the symptoms of yellow fever:
- P9: “I don't know the signs.”
3.2.2. Vaccination Decision-makingThe decision to vaccinate the child was influenced by the custodial mother for 9 participants and only one participant reported that the decision to vaccinate the child was a joint decision between the two parents. This decision was made by the mother or both parents based on knowledge of the importance of vaccination [23].
- P2: “I make this decision as a mother.”
- P7: “I am the one who takes care of the child's vaccination, my husband does not go to the CPS to decide on the child's vaccination. He never objected to it.”
- P4: “I am the one who decides on the vaccination of my baby, he had the first vaccine at birth, then the second after 45 days, I am waiting for the next vaccine.”
- P5: “Until then, I am the one who decides on the child's vaccination.”
- P1: “It is both of us who decide on the vaccination of our children.”
3.2.3. Positive Experience with ImmunizationPositive experience with vaccination was reported by 7 custodial mothers and the other 3 were primiparous and did not report a positive or negative experience. Their accounts were found in the following verbatim:
- P6: “Measles, known in the Congo as 'KITUTU', was eradicated with vaccination.”
- P2: “Positive experience, since I started to vaccinate my children from birth, my children do not get sick regularly, and they do not get fevers in any way. Vaccination allows them to fight against epidemics.”
- P1: “As a testimony, a child not vaccinated against polio or measles is easily attacked by these epidemics. In our household, no one is opposed to the vaccination of children.”
- P7: “Good experience, vaccinated children live very well, I have always encouraged parents to get their children vaccinated.”
- P8: “No one in our household is opposed to vaccinating children. No one from outside or family member can give us negative injunctions. Vaccination is a good experience.”
- P9: “I have no bad experience because vaccination protects children, so far for me it is a good thing.”
3.2.4. Parental Empowerment
All participants stated that they strictly adhered to the vaccination schedule for their children.
- P2: “I'm used to following it closely. I try not to forget the vaccination dates up to the age of 9 months.”
- P3: “I'm used to keeping track of my child's immunizations. I use the vaccination calendar and appointments given at the hospital.”
- P5: “I regularly follow the vaccination appointment dates, they are marked in the follow-up card.”
- P6: “I follow the dates given to us at the hospital, the first dose, followed by the second after 45 days, and so on. If you lose your card, you have to pay 5000FC to get another one.”
- P8: “I follow up from birth, the child is given the first vaccine, then the second after 1 month, and for the rest, I have a vaccination card and appointment.”
- P10: “I used to follow up on my baby's vaccination according to the dates fixed at the hospital. If it's the 15th of month, they'll tell you to come afterwards, for instance the 15th of next month. The dates were marked in the card and I used to follow that regularly.”
Two participants commented on not using the relay if they forgot. This is due to the awareness of the importance of vaccination:
- P10: “No, I can't forget.”
- P8: “I cannot forget the days of appointment, even if this month. I was not away for financial reasons, the next appointment I will always recover.”
One participant said that if she forgot, her husband should take over if he was careful. Otherwise, she would make up for it:
- P6: “To be reminded by my partner.”
4. DISCUSSION
Out of a sample of 2224 heads of households/custodian mothers with at least one child from 0–1-year-old, 55% were women and about 45% were men. This proportion remained close to the results found in the post-campaign survey of coverage against yellow fever in 7 provinces of the DRC, that is, 45.86% of men against 54.14% of women [24].
Regarding the vaccination status of children in routine EPI, 68.2% of children in 8 provinces were regularly vaccinated in routine EPI and about 31.8% did not follow routine vaccination including 27.7% of unvaccinated children with vaccinated parents (Table 2). This proportion of vaccinated children remains low and below 80% required by WHO. However, it exceeds the safety threshold of 60% vaccine coverage and remains below the 80% threshold to suppress local transmission [25].
It was also noted that, since 2019, global measles vaccination coverage (MCV1) has decreased from 86% to 81% in 2021 during the COVID-19 period, its lowest known rate since 2008 [26]. The continued decline in routine vaccine coverage from 2020 to 2021 is due to many factors, including pressure on health systems due to COVID-19 and the supply of COVID-19 vaccines. The situation has led to disruptions in supply chains, human resources and financing. In some countries, increased misinformation and reluctance to vaccinate are probably also contributing to the drop in the number of cases. Unless urgent measures are taken to restore vaccination programs, the risk of epidemics of vaccine-preventable diseases is likely to persist [27]. Nevertheless, the Yellow fever vaccination coverage in our study, 68.2% of children aged 0 - 1 year in 8 provinces in DRC remain significantly lower than the coverage routine EPI for children aged 12 to 23 months in South Africa, Ethiopia, and Cameroon. These countries have vaccination rates of 76.8%, 94%, and 96.3%, respectively [28, 29, 30]. However, in Nigeria, the national coverage routine PEV in 2014 was 30.6% [31], and in Uganda, it was less than 50% in 2014 [32]. These results are far superior to the multivariate analysis of a study conducted on vaccination coverage among Quebec children which indicated that 23% of parents hesitated to vaccinate their children [33]. The results of the bi-variate analyses showed that, the null hypothesis was not considered. There was a statistically highly significant influence between the vaccination status of the heads of households or mother caretakers on the routine EPI vaccination of children aged 0–12 months. Thus, there was a relationship between the immunization status of the heads of households or custodial mothers and routine EPI vaccination (χ²=62.706; p=0.000) (Table 3).
This result of the bi-variate analysis showed that there was a statistically significant relationship between the vaccination of the parents and that of children (Table 3). Thus, an explanation was sought in the qualitative part by interviewing some custodial mothers in Tshuapa Province about their experiences with routine EPI vaccination of their children aged 0–1 year.
A total of 10 custodial mothers from Tshuapa, with a child aged 0 to 12 months, voluntarily agreed to participate in individual semi-directive interviews for this study during the period from October 6th–11th, 2022. From the analysis of the interviews, the main themes that emerged included the importance of knowledge of routine EPI and yellow fever vaccination, decision to vaccinate, positive experience with vaccination, and parental empowerment (Figure 1).
In this study, following the interview hearings, half of the participants talked about some symptoms of yellow fever that they remembered. The majority of participants emphasized routine EPI vaccination and recognized that vaccination protects against vaccine-preventable epidemics. These results were consistent with those found in the study conducted in the Luiza Health Zone in Central Kasai, DRC, which reported that 8 out of 10 mothers of children aged 0–11 months were aware of the importance of full infant immunization [29]. On the other hand, the study conducted in Niamey on the determinants of the immunization status of infants under 12 months of age admitted in two hospitals indicated that the advantages and the principle of immunization were known by the majority of mothers in both hospitals [34].Indeed, several authors [35] noted the impact of parents' level of education on the decision to vaccinate their children [29].
The decision to vaccinate children was influenced by the custodial mother for 9 participants and only one participant reported that the decision to vaccinate children was a joint decision between the two parents. This decision was made by the mother or both parents based on knowledge of the importance of vaccination. This can be justified by the results of other studies which showed that the use of Antenatal Consultation and Pre-school Consultation services and maternal education were associated with complete vaccination of children [28, 32, 36, 37, 38, 39, 40].
4.1. Positive Experience with Vaccination
Positive experience with vaccination was reported by 7 custodial mothers and the other 3 were primiparous and did not report any positive or negative experience. Indeed, a study was conducted in Mali in two health districts, namely Kabalabougou and Sangarebougou of Bamako on poliomyelitis. The study revealed that the decision of mothers of children under one year of age in these two health areas was impacted by their positive perception of vaccination [41].
4.2. Parental Empowerment
The results of this study showed that parents take responsibility for their children's vaccination. Participants also reported that they strictly adhered to the vaccination schedule for their children. In contrast, the results found in Flanders, Belgium, revealed that the recommended MMR1 vaccination schedule was not adhered to by many of the infants' mothers [42].
Three participants said that they did not use relay in case of forgetfulness. This was due to the awareness of the importance of vaccination. The study conducted in Banqui in the Central African Republic emphasized that sensitization and awareness of the importance of vaccination and compliance with the EPI vaccination schedule by parents, as well as retraining of health personnel in vaccination, would reduce missed opportunities for vaccination among children aged 0–11 months [43].
It should be noted that the interviews were conducted in only one province due to the lack of resources and time, which did not really provide the lived experiences of parents in these 8 provinces. All the participants who accepted freely and voluntarily were vaccinated mothers and the majority of children were also vaccinated. Resultantly, this study did not raise reasons for non-vaccination which could be due to the parents’ refusal of getting their infants vaccinated. This represents a limitation to the current study since these hesitations and total oppositions often lead towards a decrease in family and environmental protection against vaccine-preventable diseases [44] and to an insufficiency of the vaccine coverage [45].
4.3. Conclusion
The main objective of this study was to explore whether the parental vaccination status on yellow fever vaccination influenced the routine vaccination of children aged 0–1 year. Moreover, the study also aimed to understand their lived experiences pertaining to the importance of routine vaccination for children.
The current study indicated that 53.2% of children with a non-immunized custodial mother or head of household were immunized. Although, the decrease in immunization coverage in the DRC was noted in recent years [3, 4]. Furthermore, the study also showed that the proportion of unvaccinated children with vaccinated parents was 27.7%. This proportion is of concern for the DRC.
The qualitative study showed that the importance of parental knowledge about immunization and yellow fever, positive experience with immunization, the decision to immunize, and parental accountability are among the factors that could influence the decision of heads of households and/or custodial mothers about routine child immunization. Therefore, the EPI and the Ministry of Health as well as Hygiene and Prevention of the DRC should take these factors into account in the immunization campaigns. Additionally, parental awareness sessions should be arranged and emphasis must be placed on these topics during Antenatal and Pre-school Consultation Services which could increase national immunization coverage.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Yellow fever. Ministère du travail, de la santé et des solidarités de la France Web site. https://sante.gouv.fr/soins-et-maladies/maladies/maladies-infectieuses/la-fievre-jaune.
- Yellow fever. Pan American Health Organization Web site. https://www.paho.org/en/topics/yellow-fever.
- Yellow fever - African Region (AFRO). WHO Web site. https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON510.
- Carlson R. Yellow fever outbreaks cause 11% case fatality rate. Vax Before Travel Web site. https://www.vax-before-travel.com/yellow-fever-outbreaks-cause-11-case-fatality-rate-2024-03-20.
- Yellow fever risk areas. Fit for Travel Website. https://www.fitfortravel.nhs.uk/advice/disease-prevention-advice/yellow-fever/yellow-fever-risk-areas.
- Définition de vaccination. Centre National de Ressources Textuelles et Lexicales Web site. https://www.cnrtl.fr/definition/vaccination.
- Nissen C. The age limits of healthy childhood and youth. Trib Santé. 2023;77(3):27–38. https://doi.org/10.3917/seve1.077.0027.
- UNICEF. Multiple indicator cluster survey, 2017–2018, survey results report. Kinshasa, Democratic Republic of Congo, MICS-Palu 2018. https://www.unicef.org/drcongo/media/3646/file/cod-mics-palu-2018.pdf.
- Organisation Mondiale de la Santé. Agenda for immunization 2030: a global strategy to leave no one behind. https://www.who.int/fr/publications/m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind.
- Lindsey NP, Horton J, Barrett AD, et al. Yellow fever resurgence: an avoidable crisis? NPJ Vaccines. 2022;7(1):137. https://doi.org/10.1038/s41541-022-00552-3.
- Vaccination in low-income countries: pandemic has led to decline in coverage but signs of recovery are emerging. ReliefWeb Web site. https://reliefweb.int/report/world/vaccination-dans-les-pays-faible-revenu-la-pandemie-entraine-une-baisse-de-la-couverture-mais-des-signes-de-reprise-commencent-poindre.
- Dropping vaccination rates in Democratic Republic of Congo could lead to resurgence of deadly diseases. UNICEF Web site. https://www.unicef.org/drcongo/communiques-presse/baisse-taux-vaccination-resurgence-maladies-mortelles.
- Ribau C, Lasry JC, Bouchard L, et al. Phenomenology: a scientific approach to lived experiences. Rech Soins Infirm. 2005;81(2):21–27.
- Broomé RE. Descriptive phenomenological psychological method: an example of a methodology section from doctoral dissertation. https://tinyurl.com/fwf7d4v6.
- Giorgi AP, Giorgi BM. The descriptive phenomenological psychological method. In: Camic PM, Rhodes JE, Yardley L, eds. Qualitative Research in Psychology: Expanding Perspectives in Methodology and Design. American Psychological Association; 2003:243–273.
- Giorgi A. Psychology as a Human Science: A Phenomenologically Based Approach. University Professors Press; 2020.
- Giorgi A. Sketch of a psychological phenomenological method. In: Phenomenology and Psychological Research. Duquesne University Press; 1985:8–22.
- Giorgi A. The Descriptive Phenomenological Method in Psychology: A Modified Husserlian Approach. Duquesne University Press; 2009.
- Wertz FJ. The descriptive phenomenological method in psychology: a modified Husserlian approach. J Phenomenol Psychol. 2010;41(2):269–276.
- Giorgi A. Convergence and divergence of qualitative and quantitative methods in psychology. Duquesne Stud Phenomenol Psychol. 1975;2:72–79. https://doi.org/10.5840/dspp197528.
- Reasons to vaccinate. CDC Web site. https://www.cdc.gov/vaccines/parents/why-vaccinate/vaccine-decision.html.
- Gérard EEM, Bien-Aimé MM, Marcelin NM, et al. Post-Yellow fever vaccination coverage survey in the provinces of Mongala, Tshuapa, Bas-Uele, Haut-Uele, Nord-Ubangi, Sud-Ubangi and Tshopo of the Democratic Republic of Congo in 2021. Glob Sci J. 2022;10(2):1584–1600.
- World Health Organization. Global strategy for the elimination of yellow fever epidemics (EYE) 2017–2026. https://apps.who.int/iris/handle/10665/272955.
- Minta AA, Ferrari M, Antoni S, et al. Progress towards regional measles elimination – worldwide, 2000–2021. Center for Disease Control and Prevention. https://www.cdc.gov/mmwr/volumes/71/wr/mm7147a1.htm.
- Rachlin A, Danovaro-Holliday MC, Murphy P, Sodha SV, Wallace AS. Routine vaccination coverage – Worldwide, 2021. MMWR Morbid Mortal Weekly Rep. 2022;71(44):1396–1400. https://doi.org/10.15585/mmwr.mm7144a2.
- Mbengue MAS, Sarr M, Faye A, et al. Determinants of complete immunization among Senegalese children aged 12–23 months: evidence from the demographic and health survey. BMC Public Health. 2017;17(1):630. https://doi.org/10.1186/s12889-017-4493-3.
- Ngalamulume AK, Banayi LK, Ndimba BS, Kalemba M, Zambi KM. Explanatory factors for low vaccination coverage in children aged 0 to 11 months in the Luiza Zs, DRC: risks and perception of mothers. Int J Soc Sci Sci Stud. 2022;2(6):1402–1421.
- Immunization coverage. WHO Web site. https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
- Fadnes LT, Jackson D, Engebretsen IM, et al. Vaccination coverage and timeliness in three South African areas: a prospective study. BMC Public Health. 2011;11(1):404. https://doi.org/10.1186/1471-2458-11-404.
- Lakew Y, Bekele A, Biadgilign S. Factors influencing full immunization coverage among 12–23 months of age children in Ethiopia: evidence from the national demographic and health survey in 2011. BMC Public Health. 2015;15:728. https://doi.org/10.1186/s12889-015-2078-6.
- Bekondi C, Zanchi R, Seck A, et al. HBV immunization and vaccine coverage among hospitalized children in Cameroon, Central African Republic and Senegal: a cross-sectional study. BMC Infect Dis. 2015;15(1):267. https://doi.org/10.1186/s12879-015-1000-2.
- Djafar MA, Moumouni K, Aboubacar S, et al. Determinant of the vaccination status of infants under 12 months hospitalized in two national hospitals of Niamey. J Pédiatrie Puériculture. 2022;35(1):21–28. https://doi.org/10.1016/j.jpp.2021.12.007.
- Bicaba A, Rawlings B, Ouedraogo B. The Acceptability and Feasibility of Introducing the Standard Days Method (SDM) of Family Planning in Reproductive Health Clinics in Burkina Faso West Africa. Final Report. USAID; 2005.
- Asfaw AG, Koye DN, Demssie AF, et al. Determinants of default to fully completion of immunization among children aged 12 to 23 months in South Ethiopia: unmatched case-control study. Pan Afr Med J. 2016;23:100. https://doi.org/10.11604/pamj.2016.23.100.7879.
- Abadura SA, Lerebo WT, Kulkarni U, Mekonnen ZA. Individual and community level determinants of childhood full immunization in Ethiopia: a multilevel analysis. BMC Public Health. 2015;15:972. https://doi.org/10.1186/s12889-015-2315-z.
- Antai D. Inequitable childhood immunization uptake in Nigeria: a multilevel analysis of individual and contextual determinants. BMC Infect Dis. 2009;9(1):181. https://doi.org/10.1186/1471-2334-9-181.
- Wiysonge CS, Uthman OA, Ndumbe PM, Hussey GD. Individual and contextual factors associated with low childhood immunisation coverage in sub-Saharan Africa: a multilevel analysis. PLoS One. 2012;7(5):e37905. https://doi.org/10.1371/journal.pone.0037905.
- Zaidi SMA, Khowaja S, Dharma VK, et al. Coverage, timeliness, and determinants of immunization completion in Pakistan: evidence from the Demographic and Health Survey (2006–07). Hum Vaccines Immunother. 2014;10(6):1712–1720. https://doi.org/10.4161/hv.28621.
- Sangare Y, Kone K, Diarra A, et al. Etude comparative des déterminants psychosociaux de la vaccination anti-poliomyélite à Kabalabougou et Sangarebougou. Rev Malienne Sci Technol. 2020;1(23):46–55.
- Lernout T, Theeten H, Hens N, et al. Timeliness of infant vaccination and factors related with delay in Flanders, Belgium. Vaccine. 2014;32(2):284–289. https://doi.org/10.1016/j.vaccine.2013.10.084.
- Bobossi-Serengbé G, Fioboy R, Ndoyo J, Nakouné E. Missed opportunities for immunization in children of 0 to 11 months in Bangui. J Pédiatrie Puériculture. 2014;27(6):289–293. https://doi.org/10.1016/j.jpp.2014.08.010.
- MacDonald NE, Dubé E. Nouvelle ressource permettant de résumer les données sur la vaccination provenant du Centre canadien de ressources et d'échange sur les données probantes en vaccination (CANVax). Relevé Mal Transm Au Can. 2020;46(1):17–21. https://doi.org/10.14745/ccdr.v46i01a03f.
- Bégué P. Le refus des vaccinations. Aspects actuels en 2012 et solutions en santé publique. Bull Académie Natl Médecine. 2012;196(3):603–618.
- MacDonald NE, Dubé E. Nouvelle ressource permettant de résumer les données sur la vaccination provenant du Centre canadien de ressources et d’échange sur les données probantes en vaccination (CANVax). Relevé Mal Transm Au Can. 2020;46(1):17–21. http://doi.org/10.14745/ccdr.v46i01a03f.
- Bégué P. Le refus des vaccinations. Aspects actuels en 2012 et solutions en santé publique. Bull Académie Natl Médecine. 2012;196(3):603–618.