
| Review | Open Access |
|---|
Clinical Characteristics, Causes, and Treatment Outcomes of Hydrocephalus in Children Under Six: A Retrospective Study from a Single Center in Quetta, Baluchistan |
 |
|---|
![]() Nadia Ewaz Ali*, Humera Javed, Bibi Asma, Samia Ishtiaq, Saira Iqbal, and Nabeela Tariq
Nadia Ewaz Ali*, Humera Javed, Bibi Asma, Samia Ishtiaq, Saira Iqbal, and Nabeela Tariq
Sardar Bahadur Khan Women University, Quetta, Pakistan
Background. Hydrocephalus is defined by an abnormal build-up of Cerebrospinal Fluid (CSF) within the brain's ventricles. The long-term effects of hydrocephalus can range considerably and are frequently unpredictable. Due to its life-threatening nature, particularly in newborns and toddlers, the treatment of hydrocephalus is of utmost importance. The exact epidemiology of infantile hydrocephalus in Pakistan is unknown. This retrospective cohort study intended to examine the clinical importance of hydrocephalus patients under 6 years. Furthermore, it also addressed the potential gaps in medical knowledge on the local epidemiology, risk factors, and therapeutic methods of this condition at a tertiary care centre of Quetta Baluchistan, Pakistan.
Results. A total of 29 hydrocephalus patients (18 congenital and 11acquired) were included in the study. A comprehensive questionnaire was designed to collect the demographic and clinical information of the patients. After statistical analysis, it was determined that gender and age distribution between the two groups, congenital and acquired hydrocephalus, was similar, showing no significant differences (p=0.196, p=0.867). The most common symptoms were irritability, drowsiness, and a head growing through seizures. Moreover, sun-setting eyes also appeared commonly. Post-natal diagnosis and imaging (CT and MRI) dominated the diagnostic methods of congenital hydrocephalus. Whereas brain MRI accounted for most cases with acquired hydrocephalus. The origin of acquired hydrocephalus was frequently unknown, aqueduct stenosis was the primary cause of congenital hydrocephalus. Medical treatment, ventriculoperitoneal (VP) shunting, and ETV (Endoscopic Third Ventriculostomy) were similar in all groups. The most frequent side effect for medications and VP shunts was irritation, while the most frequent side effect for ETV operations was sore throat.
Conclusion. This study underlined the importance of early diagnosis, proper treatment, and continuous follow-up in hydrocephalus patients. Though the treatment approaches in accordance with clinical practices, the frequency of complications has necessitated continued medical care to achieve the best possible outcomes. Further research into the local epidemiology and more effective therapeutic approaches is very important to enhance care for hydrocephalus patients in the region.
Highlights
- A higher incidence of congenital hydrocephalus in infants under 6 years in Quetta, Baluchistan, with maternal health issues identified as a key contributing factor.
- Emphasized the need for further exploration of potential gender-related factors as no gender disparity found.
- Continuous medical care and follow-up were crucial due to complications like irritability, infections, and fever.
1. INTRODUCTION
Hydrocephalus is a condition in which Cerebrospinal Fluid (CSF) accumulates inside the brain and causes head enlargement associated with other serious complications [1]. CSF is a colourless fluid that is mainly produced by the ventricular system of brain called choroid plexus. It moves through the 3rd and 4th ventricles. Some amount of CSF also travels through subarachnoid space and gets absorbed into the subarachnoid granulations [2]. It may accumulate due to several reasons, such as barriers to its regular flow, excessive production or problems with its absorption. Since it is frequently present at birth, hydrocephalus in infants without a clear external cause is typically referred to as ‘congenital hydrocephalus’. The type of hydrocephalus that develops as a side effect of another ailment, such as bleeding, an infection, or a tumour, is termed as ‘acquired’ [3].
A Chinese survey revealed that there are 20.3% congenital hydrocephalus births for every 10,000 people [4]. According to a study conducted in Ghana, its incidence is 57.3% higher than that of the other birth abnormalities [5]. Furthermore, another study found a higher risk of hydrocephalus in infants born with neural tube defects, such as meningocele, meningomyelocele, and encephalocele [6]. According to an estimate by a hospital in Peshawar, Pakistan, out of 1062 deliveries, 22.6 were hydrocephalus [7]. Its frequency in Pakistan is estimated to be 2.5:1 and is most common among lower to middle socioeconomic strata.
Hydrocephalic patients have some common symptoms, such as vomiting, behavioural changes, drowsiness, headaches, stiff neck or back ache. This inappropriately increases the occipitofrontal circumference anterior fontanelle, splayed cranial sutures, scalp vein distension, sun-setting, decreased conscious level, neck retraction or rigidity, as well as acute strabismus [8].
Diagnostic testing primarily involves brain imaging. An infant with an open fontanel can be examined for ventriculomegaly by cranial ultrasonography. However, an MRI study is usually warranted (preferred over CT because an MRI does not expose a fetus to radiation and provides for more information) to identify the anatomy and cause of increased intracranial pressure. Cine MRI CSF flow imaging may even shed light on patient’s specific changes in CSF hydrodynamics. For particular cases, especially when a potential site of obstruction is unknown, these tests may provide guidance about surgery and offer a vehicle to evaluate response to therapy [9, 10].
This condition is caused by different factors, such as injury, trauma, and medication (intake of antidepressants, antidiabetic). Furthermore, it can also be associated with certain birth deformities, such as spina bifida [8]. The most frequent cause of congenital hydrocephalus has been linked with aqueduct stenosis, neural tube defects, encephaloceles, and meningomyeloceles [11]. Patients of various ages have been diagnosed with both prenatal and postnatal kinds, where the size of the ventricles and the location of blockage are mostly determined by invasive procedures called ventriculography and pneumoencephalography [12]. Surgery is the most common form of treatment for hydrocephalus and shunts come in a variety of kinds depending upon the type and severity of the condition. Medications, such as Acetazolamide and furosemide are used to treat hydrocephalus [13]. These treatments are considerably prioritized over first line medications. However, these may also have different types of complications, such as, irritation, haemorrhage, fever, infection, seizures, and failure of surgery [14]. Although, research in hydrocephalus is rapidly progressing worldwide, very little regional data is available on the epidemiology, diagnostic practices, and treatment outcomes in Pakistan. Specifically, the issues that patients may be exposed to in Quetta, Baluchistan, regarding healthcare access, maternal health, and resource scarcity pertaining to diagnosis and management, are unknown. Therefore, the current study aimed to fill this gap by providing a comprehensive analysis of hydrocephalus in this underserved region. Moreover, it also contributed valuable insights to local healthcare improvement and policymaking.
2. Methodology
The current study employed a cross-sectional research design to investigate hydrocephalus patients at a tertiary care hospital in Quetta, Baluchistan from September 2021 to 2022. The research aimed to explore the clinical characteristics and distinctions between congenital and acquired hydrocephalus within a sample of 29 (18 congenital and 11 acquired) patients under the age of 3. A comprehensive questionnaire, encompassing inquiries about demographic data, medical history, clinical presentation, diagnostic techniques, treatment methods, and treatment outcomes was distributed among the patients’ family members with proper informed consent. Inclusion criteria for the current study encompassed patients of both genders, aged up to six years, who had been diagnosed with hydrocephalus and had undergone various treatment methods. Patients older than six years and those who declined to participate in the research were excluded from the study. Data collected from the questionnaire was subjected to statistical analysis using the Statistical Package for the Social Sciences (SPSS) software. Descriptive statistics, including frequencies, means, and standard deviations, were employed to summarize the demographic information, clinical characteristics, and treatment outcomes. Chi square test was employed as the statistical method, with statistical significance defined as p<0.05. Ethical guidelines, including informed consent, patient confidentiality, and data protection, were strictly adhered to throughout the study.
3. Results
The congenital group comprised 61.1% females and 38.9% males, whereas the acquired group consisted of 36.4% females and 63.6% males. Statistical significance was not found in the gender distribution (p=0.196, OR=2.75, 95% CI: 0.582–12.97). In all groups, the age distribution between 0 and 3 years and 3 and 6 years was comparable, with no discernible difference (p=0.867, OR=0.875, 95% CI: 0.181–4.21). This suggests that congenital or acquired status did not significantly correlate with either gender or age (Table 1).
Table 1. Distribution of Patients According to Gender and Age
|
|
Status |
p value |
OR 95%(CI) |
|
|---|---|---|---|---|
|
Congenital n (%) |
Acquired n (%) |
|||
|
Gender |
|
|
|
|
|
Female |
11(61.1) |
4 (36.4) |
0.196ns |
2.75 (0.582,12.97). |
|
Male |
7(38.9) |
7 (63.6) |
||
|
Age (Years) |
|
|||
|
0-3 years |
12(66.7) |
7(63.6) |
0.867ns |
0.875 (0.181,4.21). |
|
3-6 years |
6(33.3) |
4(36.4) |
||
|
Total |
18(100%) |
11(100%) |
||
The frequency (%) of extremely common symptoms in patients with congenital hydrocephalus is shown in Figure 1. All the patients showed irritability, drowsiness, and a growing head, indicating that these were common symptoms among the group. Seizures (77.7%), sun-setting eyes (83.3%), and antiseptic reflux/vomiting (72.2%) were among the other common symptoms. The least common symptom mentioned by 55.5% of the patients was trouble feeding.
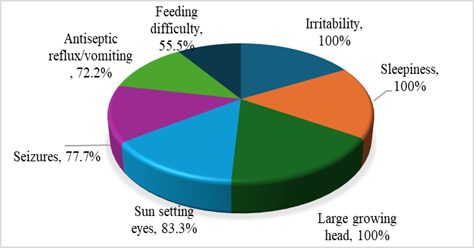
Figure 1. Frequency (%) Distribution of Symptoms of Congenital Patients. Hydrocephalus
According to the distribution of diagnostic approaches used for congenital hydrocephalus, postnatal diagnosis was universally applied, with raised intracranial pressure (ICP) used by 100% of patients. Imaging techniques, such as CT scans (55.5%) and MRI (44.4%) were also used frequently. Prenatal diagnostic methods, including prenatal diagnosis, ultrasound, and 3D scans, each contributed to 11.1% of diagnoses.
For acquired hydrocephalus, the most utilized diagnostic approach was brain MRI, identifying 63.6% of cases. Other methods included brain CT scans (27.2%) and brain CT scans with dye (9.2%) (Table 2).
Table 2. Distribution of Diagnostic Approaches in Patients with Congenital and Acquired Hydrocephalus
|
Diagnosis Type |
Diagnostic Approach |
Positive Diagnoses (n) |
Percentage (%) |
|
|---|---|---|---|---|
|
Congenital |
Prenatal Diagnosis |
2 |
11.1 |
|
|
Ultrasound |
2 |
11.1 |
||
|
3D Scan |
2 |
11.1 |
||
|
Postnatal Diagnosis |
18 |
100 |
||
|
Raised ICP |
18 |
100 |
||
|
CT scan |
10 |
55.5 |
||
|
MRI |
8 |
44.4 |
||
|
Valid N (list-wise) |
18 |
100 |
||
|
Acquired |
Brain MRI |
7 |
63.6 |
|
|
Brain CT scan |
3 |
27.2 |
||
|
Brain CT scan with Dye |
1 |
9.2 |
||
|
Valid N (list-wise) |
11 |
100 |
||
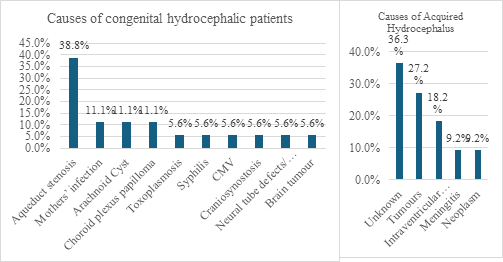
Figure 2. Frequency (%) Distribution of Causes of Congenital and Acquired Hydrocephalus
Among the causes of congenital hydrocephalus, aqueduct stenosis was the most prevalent cause, affecting 38.8% of patients. Maternal infections, arachnoid cysts, choroid plexus papilloma, and toxoplasmosis were each responsible for 11.1% of cases. While syphilis, CMV, craniosynostosis, neural tube defects, and brain tumours contributed to 5.6% of cases each. In contrast, for acquired hydrocephalus, the leading cause remained unknown, accounting for 36.3% of patients. Tumours were the second most common cause (27.2%), followed by intraventricular haemorrhage (18.2%), with meningitis and neoplasms contributing equally at 9.2%. These findings highlight the differences in etiological factors between congenital and acquired hydrocephalus, with aqueduct stenosis being prominent in congenital cases and an unknown aetiology dominating acquired cases (Figure 2).
Table 3 presents the distribution of treatment approaches among congenital and acquired hydrocephalus patients, along with the respective percentages and p-value (0.632), indicating no statistically significant difference between the two groups.
For congenital hydrocephalus, all patients (100%) underwent first-line medical treatment, while 61.1% required shunting, and 22.2% underwent Endoscopic Third Ventriculostomy (ETV). Post-surgical medical management was implemented in 16.6% of cases, and tumor removal was performed in 5.6% cases. In contrast, for acquired hydrocephalus, all patients (100%) also received first-line medical treatment, with 36.3% undergoing ventriculoperitoneal (VP) shunting and 18.2% undergoing ETV.
Table 3. Prevalence of Treatment Options among Hydrocephalus Patients
|
|
No. of patients |
Percentage (%) |
p-value |
|
|---|---|---|---|---|
|
Congenital |
First line medical treatment |
18.00 |
100.0 |
0.632534 |
|
Shunting |
11.00 |
61.1 |
||
|
ETV |
4.00 |
22.2 |
||
|
Post-surgery medical management |
3.00 |
16.6 |
||
|
Tumour removal |
1.00 |
5.6 |
||
|
Valid N (list wise) |
18.00 |
100.0 |
||
|
Acquired |
First line medical treatment |
11.00 |
100.0 |
|
|
VP shunt |
4.00 |
36.3 |
||
|
ETV |
2.00 |
18.2 |
||
|
Valid N (list wise) |
11.00 |
100.0 |
||
Table 4 presents the complications observed in congenital and acquired hydrocephalus patients undergoing different treatments, highlighting the most prevalent issues. For medicines, irritability was the most common complication, affecting 22 patients (11 congenital and 11 acquired), followed by increased urine output (14 patients) and slow or no response (6 congenital patients). In VP shunt treatments, irritability was again the most frequent complication, reported in 6 patients equally distributed between congenital and acquired cases. While fever (5 patients) and infection (4 patients) were also noted. For ETV, sore throat was the most prevalent complication observed in 9 congenital patients, with infection (5 patients) and clogged lines (1 patient) occurring exclusively in congenital cases. Overall, irritability was the leading complication for medicines and VP shunts, while sore throat was most common in ETV procedures.
Table 4. Prevalent Complications Associated with Treatment of Hydrocephalus
|
Treatment |
Complications |
Congenital (n) |
Acquired(n) |
Total |
|---|---|---|---|---|
|
Medicines |
Irritability |
11 |
11 |
22 |
|
Slow or No Response |
6 |
0 |
6 |
|
|
Increased Urine Output |
5 |
9 |
14 |
|
|
(Highest) |
Irritability (22patients) |
|||
|
VP Shunt |
Infection |
3 |
1 |
4 |
|
Fever |
3 |
2 |
5 |
|
|
Irritability |
3 |
3 |
6 |
|
|
(Highest) |
Irritability (6 patients) |
|||
|
ETV |
Sore Throat |
9 |
0 |
9 |
|
Infection |
5 |
0 |
5 |
|
|
Clogged Lines |
1 |
0 |
1 |
|
|
(Highest) |
Sore Throat (9 patients) |
4. Discussion
Infantile hydrocephalus is one of the most common clinical conditions. The total number of patients included in the current study was 29. Among them, 18 patients had congenital hydrocephalus, whereas 11 had acquired hydrocephalus and the retrospective age of these patient were from birth till six (0-6 years). According to different studies, maximum patients of hydrocephalus are infants [15, 16, 17]. The current study could not find significant association of the condition with gender and age, in contrast to the current study the condition was found to be more prevalent in males as compared to females, as reported by two previous studies [18, 19]. The most frequent presenting signs and symptoms in the current study included head enlargement, fontanelle bulging, and setting sun-sign eyes. Various studies have also observed such clinical symptoms [16, 20, 21] has reported by [22]. Sun-setting eyes were observed in about 30% cases of hydrocephalus. According to the current study, the most common cause of hydrocephalus was aqueduct stenosis (38%), followed by infection in mother (22%), and haemorrhages 16%. Similar aetiologies were observed in some other studies [19, 21, 23]. Among the patients, 11% were prenatally diagnosed using ultrasound, whereas the postnatal diagnosis was made through measuring ICP (intracranial pressure), CT scan, and ultrasound. The ultrasound was used as a diagnostic method in a study conducted in Japan in which out of 393 patients, 193 were diagnosed using the method [24]. In the current study, medical treatment was first line treatment option for most of the patients, followed by shunt and ETV as later options. Furthermore, a study was conducted in South Africa in 2001, according to which 217 children with hydrocephalus were initially treated medically and they had communicative hydrocephalus 25. By using this method, the authors were able to keep more than 70% of the patients out of surgery [25]. The medical treatment had some complications observed in the patients that included irritability, seizures, infections, excessive urination, and swelling. The adverse effects of medical treatment observed in some other studies were mild diarrhoea, mild paraesthesia, occasional vomiting, and appetite suppression [26]. These results deviate from the current study, the difference in the results may be due to geographic location or ethnicity.
Among all the patients, 61% of them underwent shunt treatment, whereas 22% chose ETV as a surgical treatment. The shunt-treated patients experienced complications that included sore site, infections, and clogged lines, whereas some of them needed longer shunt. The complications other than infections were different as reported in various studies by [17, 27]. Shunt infection rate as reported in the current study is comparable with the studies conducted by [28]. Approximately, 22% of the patients who underwent ETV had complications, for instance irritability, slow response, seizures, recurrent infection, excessive urine output, and swelling. The complications of ETV, according to some other studies [29], include CSF leakage hyponatremia and bleeding during surgery [30]. The contradiction of current study with other studies is due to small sample size that has limited the statistical power. This emphasizes the necessity of more extensive, multicenter research to corroborate results. Notwithstanding this drawback, this study offered vital baseline information to comprehend hydrocephalus in Quetta, Baluchistan's underserved community.
4.1. Conclusion
The current cross-sectional study conducted in Quetta, Baluchistan, shed light on the prevalence, gender distribution, causes, symptoms, risk factors, diagnostic methods, and treatment options of hydrocephalus in a sample of 29 individuals. The results correlate with the global pattern, however, it also throws up unique regional challenges, such as lack of prenatal diagnostic facilities. Absence of gender predominance might be due to small sample size, which suggests further large-scale studies. This study emphasized that maternal healthcare, early diagnosis, and tailored treatment would improve patient outcomes. Subsequent studies should focus on broader population-based data for validation and expansion of such findings. Further research should focus on population-based data and improvement of regional health infrastructure to better address hydrocephalus management in resource-poor settings.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Hetherington R, Dennis M, Barnes M, Drake J, Gentili F. Functional outcome in young adults with spina bifida and hydrocephalus. Childs Nerv Syst. 2006;22(2):117–124. https://doi.org/10.1007/s00381-005-1231-4
- Kahle KT, Kulkarni AV, Limbrick DD, Warf BC. Hydrocephalus in children. Lancet. 2016;387(10020):788–799. https://doi.org/10.1016/S0140-6736(15)60694-8
- Tully HM, Dobyns WB. Infantile hydrocephalus: a review of epidemiology, classification and causes. Eur J Med Genet. 2014;57(8):359–368. https://doi.org/10.1016/j.ejmg.2014.06.002
- Surti A, Usmani A, Javaid Q, Shafique S. Association of fetal hydrocephalus with other embryological anomalies: a prenatal ultrasound-based study. Pak J Med Sci. 2022;38(6):1617–1621. https://doi.org/10.12669/pjms.38.6.5223
- Alhassan A, Adam A, Nangkuu D. Prevalence of neural tube defect and hydrocephalus in Northern Ghana. J Med Biomed Sci. 2017;6(1):18–23. https://doi.org/10.4314/jmbs.v6i1.3
- Dewan MC, Rattani A, Mekary R, Glancz LJ, Yunusa I, Baticulon RE, Fieggen G, Wellons JC, Park KB, Warf BC. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg. 2018;130(4):1065–1079. https://doi.org/10.3171/2017.10.JNS17439
- Khan A, Zuhaid M, Fayaz M, Ali F, Khan A, Ullah A, Ahmad I. Frequency of congenital anomalies in newborns and its relation to maternal health in a Tertiary Care Hospital in Peshawar, Pakistan. Int J Med Stud. 2015;3(1):19–23. https://doi.org/10.5195/ijms.2015.108
- Kirkpatrick M, Engleman H, Minns R. Symptoms and signs of progressive hydrocephalus. Arch Dis Child. 1989;64(1):124–128. https://doi.org/10.1136/adc.64.1.124
- Quencer RM. Intracranial CSF flow in pediatric hydrocephalus: evaluation with cine-MR imaging. Am J Neuroradiol. 1992;13(2):601–608. https://doi.org/10.3174/ajnr.A0132
- Faggin R, Calderone M, Denaro L, Meneghini L, d’Avella D. Long-term operative failure of endoscopic third ventriculostomy in pediatric patients: the role of cine phase-contrast MR imaging. Neurosurg Focus. 2011;30(4):e1. https://doi.org/10.3171/2011.1.FOCUS10303
- Adeloye A. Management of infantile hydrocephalus in Central Africa. Trop Doct. 2001;31(2):67–70. https://doi.org/10.1177/004947550103100203
- Kiefer M, Unterberg A. The differential diagnosis and treatment of normal-pressure hydrocephalus. Dtsch Arztebl Int. 2012;109(1-2):15–25. https://doi.org/10.3238/arztebl.2012.0015
- Kanev PM, Park T. The treatment of hydrocephalus. Neurosurg Clin N Am. 1993;4(4):611–619. https://doi.org/10.1016/S1042-3680(18)30553-9
- Vinchon M, Rekate H, Kulkarni AV. Pediatric hydrocephalus outcomes: a review. Fluids Barriers CNS. 2012;9(1):18. https://doi.org/10.1186/2045-8118-9-18
- Pan P. Outcome analysis of ventriculoperitoneal shunt surgery in pediatric hydrocephalus. J Pediatr Neurosci. 2018;13(2):176–181. https://doi.org/10.4103/jpn.JPN_29_18
- Kyalo MC, Nganga NH, Kamau MN. Management and functional outcome of childhood hydrocephalus at the Kenyatta National Hospital, Nairobi. UoN Digit Repository. 2015. https://doi.org/10.4314/eah.v29i4.9
- Tambo FM, Djientcheu V, Chiabi A, Mbonda E, Tchatat E, Ngowe MN. Our experience in the management of infantile hydrocephalus: a study on thirty-five regrouped cases in Yaounde, Cameroon. Afr J Paediatr Surg. 2011;8(2):199–202. https://doi.org/10.4103/0189-6725.86062
- Abebe MS, Seyoum G, Emamu B, Teshome D. Congenital hydrocephalus and associated risk factors: an institution-based case-control study, Dessie Town, North East Ethiopia. Pediatr Health Med Ther. 2022;13:175–182. https://doi.org/10.2147/PHMT.S364447
- Kutscher A, Nestler U, Bernhard MK, Merkenschlager A, Thome U, Kiess W, Schob S. Adult long-term health-related quality of life of congenital hydrocephalus patients. J Neurosurg Pediatr. 2015;16(6):621–625. https://doi.org/10.3171/2015.4.PEDS15106
- Yusuf AS, Omokanye HK, Adeleke NA, Akanbi RO, Ajiboye SO, Ibrahim HG. Management and outcome of infantile hydrocephalus in a tertiary health institution in Nigeria. J Neurosci Rural Pract. 2017;8(2):249–253. https://doi.org/10.4103/jnrp.jnrp_321_16
- Ahmed A, Sandlas G, Kothari P, Sarda D, Gupta A, Karkera P, Joshi P. Outcome analysis of shunt surgery in hydrocephalus. J Indian Assoc Pediatr Surg. 2009;14(3):98–101. https://doi.org/10.4103/0971-9261.57700
- Shallat RF, Pawl RP, Jerva MJ. Significance of upward gaze palsy (Parinaud’s syndrome) in hydrocephalus due to shunt malfunction. J Neurosurg. 1973;38(6):717–721. https://doi.org/10.3171/jns.1973.38.6.0717
- Saidu SA, Maaji SM, Nzeh DA, Shehu B, Ismail N. Sonographic pattern of hydrocephalus among the under five children in Sokoto North Western Nigeria. Sahel Med J. 2015;18(4):172. https://doi.org/10.4103/1118-8561.176584
- Moritake K, Nagai H, Nagasako N, Yamasaki M, Oi S, Hata T. Diagnosis of congenital hydrocephalus and delivery of its patients in Japan. Brain Dev. 2008;30(6):381–386. https://doi.org/10.1016/j.braindev.2007.11.002
- Luscombe NM, Greenbaum D, Gerstein M. What is bioinformatics? a proposed definition and overview of the field. Methods Inf Med. 2001;40(4):346–358. https://doi.org/10.1055/s-0038-1634431
- Hetherington R, Dennis M, Barnes M, Drake J, Gentili F. Functional outcome in young adults with spina bifida and hydrocephalus. Childs Nerv Syst. 2005;22(2):117–124. https://doi.org/10.1007/s00381-005-1231-4
- Deshmukh SN, Yadav AT. Clinical study and management of hydrocephalus in children. Int Surg J. 2020;7(4):1258–1262. https://doi.org/10.18203/2349-2902.isj20201191
- Mancao M, Miller C, Cochrane B, Hoff C, Sauter K, Weber E. Cerebrospinal fluid shunt infections in infants and children in Mobile, Alabama. Acta Paediatr. 2007;87(6):667–670. https://doi.org/10.1111/j.1651-2227.1998.tb01527.x
- Rajshekhar V, Moorthy R. Endoscopic third ventriculostomy for hydrocephalus: a review of indications, outcomes, and complications. Neurol India. 2011;59(6):848–854. https://doi.org/10.4103/0028-3886.91364
- Javadpour M, Mallucci C, Brodbelt A, Golash A, May P. The impact of endoscopic third ventriculostomy on the management of newly diagnosed hydrocephalus in infants. Pediatr Neurosurg. 2001;35(3):131–135. https://doi.org/10.1159/000050406