Clinical Significance of Molecular and Blood Biomarkers in Assessing the Severity of Dengue Infection in Peshawar, Pakistan
Aiman Waheed1,*, Muhammad Adnan2,Faisal Khan3, Asif Ali4,Nadia Kauser5, and Muhammad Moiz Malik1
1Center of Biotechnology and Microbiology, University of Peshawar, Pakistan
2Faculty of Allied Health and Biological Sciences, Ibadat International University of Islamabad, Pakistan
3Department of Nursing, Vertex Institute of Science and Technology, Abbottabad, Pakistan
4Department of Biotechnology, Faculty of Chemical & Life Sciences, Abdul Wali Khan University Mardan, Pakistan
5Department of Chemical and Life Sciences Qurtuba University of Science & Information Technology, Peshawar, Pakistan
ABSTRACT
Objective. . The current study was aimed to evaluate the impact of molecular and blood biomarkers on the severity of dengue fever.
Methods. . This study was conducted at the Center for Microbiology and Biotechnology, University of Peshawar, Khyber Pakhtunkhwa, Pakistan from June 2022 to November 2022. A total of 2,400 individuals exhibiting prominent signs and symptoms of dengue fever were enrolled. These subjects were screened for the presence of NS1, IgG, and IgM antibodies, as well as molecular biomarkers, using PCR.
Results. Out of the 2,400 suspected cases, 801 (33.37%) were confirmed for dengue fever based on NS1 antigen (33.37%), as well as IgG (3.37%) and IgM (11.25%) antibodies, with RT-PCR demonstrating 98.2% sensitivity. The DENV-3 serotype was identified as the most prevalent (61.18%). The highest infection rate was observed in men (56.05%), as compared to women (43.95%). The most affected age group was 16-30 years (46.19%). Common symptoms among the patients included fever (100%), muscle pain (100%), headache (69.78%), vomiting (49.2%), and skin rash (35.08%). The study found a significant association (p < 0.05) between hematological parameters and dengue infection, highlighting a significant decrease in total leucocyte count (TLC), eosinophils, neutrophils, and platelets, as well as a significant increase in monocytes and lymphocytes. Additionally, mild cases exhibited fewer clinical signs as compared to severely infected cases.
Conclusion. Based on the current report, it was concluded that climate change, rapid urbanization, and the emergence of different serotypes may escalate dengue outbreaks in District Peshawar, KPK, Pakistan. This highlights the critical necessity for extensive insect-control operations, public education campaigns, and climate-responsive strategies to successfully prevent future dengue epidemics.
- The current study was aimed to evaluate the severity of dengue infection based on molecular and blood biomarkers.
- In comparison with immunological tests, RT-PCR detection was determined as more specific and sensitive for identifying dengue virus infection.
- Molecular biomarkers, such as DENV-3, were determined as more predominant and a significant association between hematological parameters and dengue severity was established.
1. INTRODUCTION
A high ratio of dengue virus outbreaks have been reported all over the world, including in regions previously considered non-endemic. This mosquito-borne viral disease is particularly common in tropical and subtropical regions [1]. The World Health Organization (WHO) estimates that 100–400 million cases of dengue occur annually, with approximately 96 million being clinically diagnosed [2]. As of September 2024, Pakistan had recorded 2,795 new dengue cases, with Balochistan being the worst-hit area, reporting the highest number of cases in a single week. The dengue virus (DENV) is a single-stranded positive-sense RNA virus, which belongs to the Flaviviridae family and the Flavivirus genus [1]. There are four primary DENV serotypes found globally (DENV-1, DENV-2, DENV-3, DENV-4), along with the rare DENV-5 serotype. Previous studies confirmed the prevalence of various DENV serotypes in different regions of Pakistan, including Punjab (DENV-1, 2, 3, and 4) and Khyber Pakhtunkhwa (DENV-2 and 3) [2, 3], with DENV-5 documented through neutralization techniques [4, 5].
DENVs are transmitted by female Aedes mosquitoes classified into two groups, namely primary vectors (Aedes aegypti, or yellow fever mosquitoes) and secondary vectors (Aedes albopictus). The infection can be asymptomatic or may cause fever, mimicking other health issues, such as dengue fever (DF), dengue hemorrhagic fever (DHF), and dengue shock syndrome (DSS) [6]. About 5–10% of severe dengue cases result in mortality, while the remaining patients recover and develop immunity [2].
Since the first reported case in Punjab in 1982, dengue virus infection has become endemic in Pakistan [7]. The country has experienced several deadly outbreaks. A significant outbreak occurred in Punjab in 2011, with 21,685 cases and 350 deaths [8–10]. The first major and lethal outbreak in Khyber Pakhtunkhwa (KPK) was documented in Swat in 2013, with 8,546 cases and 33 deaths [11]. Another severe outbreak occurred in KPK in 2017, resulting in 24,938 cases and 70 fatalities [1]. According to the National Institute of Health (NIH), a total of 25,932 cases with 62 deaths were reported between January and September 2022. Sindh accounted for the highest proportion of cases (32%, n=6,888), followed by Punjab (29%, n=6,255), Khyber Pakhtunkhwa (25%, n=5,506), and Balochistan (14%, n=3,128) [12]. As of 2024, more than 20,072 confirmed cases have been reported in Pakistan by the end of the month of September, with a significant number of cases documented in Sindh, Punjab, and KPK [13]. In this backdrop, the current study aimed to evaluate the incidence of dengue infection in District Peshawar, KPK. Additionally, it assessed the clinical manifestations and laboratory markers of dengue-positive patients.
2. MATERIAL AND METHOD
2.1. Study Area
The current study was conducted in District Peshawar, KPK, Pakistan. Peshawar, the largest city and capital of the KPK province, is situated in the northwestern region of the country. According to the most recent census, the district has a population of approximately 4,331,959, spread across an area of 1,257 square kilometers. About 45% of the population resides in urban areas, with an average annual growth rate of 3.93%.
2.2. Sample Size and Processing
The study included 2,400 suspected patients presenting with various symptoms, including persistent fever, nausea, vomiting, skin rashes, and muscle or body pain. Blood samples were collected from these individuals at the Khyber Teaching Hospital (KTH), Peshawar. Diagnostic tests, including the detection of NS1, IgM, and IgG antibodies, were performed at the Microbiology Laboratory of the University of Peshawar. Positive samples were further analyzed using RT-PCR to identify different dengue serotypes within 24 hours.
2.3. Immunological Tests
Venous blood samples (4 ml) were collected from suspected patients in aseptic EDTA tubes. The samples were centrifuged at 3,000 rpm for 6 minutes to obtain plasma for the detection of anti-dengue antibodies using the Tuber Dengue NS1 Ag ELISA (Merux Pty Ltd., Australia). To convert the anticoagulated plasma into serum, the anticoagulant was neutralized using different methods, such as dialysis or ion exchange resins. After the removal of the anticoagulant, the samples were allowed to clot, facilitating the separation of the serum. However, for improved efficiency and simplicity, non-anticoagulated blood was utilized primarily for direct serum extraction, allowing natural clotting to occur without additional processing. The presence of dengue virus-specific IgM antibodies was analyzed using an IgM capture ELISA (TUBER ELISA Dengue IgM, Merux Pty Ltd., Australia). The presence of anti-IgG antibodies was confirmed using TUBER ELISA Dengue IgG (Merux Pty Ltd., Australia).
2.4. Molecular Identification of Dengue Virus/Serotypes
In this study, dengue-positive samples were identified using RT-PCR for viral RNA detection and different serotypes were evaluated following the standard protocol [3]. Dengue RNA was extracted from 140µl serum using viral kit (QIA mini kit, Qiagen, Germany). A real-time Taqman PCR (one-step) was performed for dengue serotyping and detecting viral RNA. The viral RNA was used for different serotypes including DENV1–DENV-4. We used Dengue serotype-specific primers, namely Dengue-Forward (DF1): CAAAAGGAAGTCGTGCAATA and Dengue-Reverse (DR1): CTGAGTGAATTCTCTCTACTGAACC, including the Type Specific 1 (TS1) primer for DENV1: CGTCTCAGTGATCCGGGGG, TS2 (DENV2): CGCCACAAGGGCCATGAACAG, TS3 (DENV3): TAACATCATCATGAGACAGAGC, TS4 (DENV4): CTCTGTTGTCTTAAACAAGAGA.
Table 1.Gender-wise and Age-wise Distribution of Dengue-positive Cases| Variable | Number of Positive Cases | Percentage | p-value |
|---|---|---|---|
| Gender | |||
| Male | 449 | 56.05 | 0.001 |
| Female | 352 | 43.95 | |
| Total | 801 | 100 | |
| Age | % | ||
| 1–15 | 89 | 11.11 | |
| 16–30 | 370 | 46.19 | |
| 31–45 | 274 | 34.2 | |
| 46–60 | 56 | 6.99 | |
| >60 | 12 | 1.49 | |
| Total | 801 | 100 | |
| SD ± 27.71 ± 15.15 |
3.2. Immunological Information
All patients in the study were tested using ICT and ELISA techniques for the presence of NS1, IgM, and IgG antibodies, confirming 801 positive dengue cases. All samples tested positive for NS1, while 270 (33.75%) tested positive for IgM, and 81 (10.1%) tested positive for IgG antibodies using the ICT technique. Similarly, the samples (2,160) were examined for dengue antibodies and antigens using ELISA. Of these, 279 (28.79%) were tested positive for NS1, followed by 196 (33.91%) for IgM, and 107 (17.45%) for IgG, as shown in tables 2 and 4.
Table 2.Frequency of Anti-dengue Antibodies in Positive Cases| Anti-dengue Antibodies | Number of Cases (%) | Positive (%) | p-value |
|---|---|---|---|
| NS1 | 1599 (66.62) | 801 (33.37) | – |
| IgG | 2319 (96.62) | 81 (3.375) | 0.78 |
| IgM | 2130 (88.75) | 270 (11.25) | 0.70 |
3.3. Clinical Manifestations
Several associated clinical features were compared between dengue-positive and dengue-negative patients. Among the 801 dengue-positive patients, all (100%) experienced muscular pain, as compared to 1,201 (75%) dengue-negative patients. Headaches were reported by 559 (69.78%) dengue-positive patients and 945 (59.1%) dengue-negative patients. Additionally, vomiting, abdominal pain, rashes, and cough were noted in 529 (33%), 161 (10.1%), 129 (8%), and 401 (25%) dengue-negative patients, respectively. In contrast, 394 (49.2%), 299 (37.32%), 281 (35.08%), and 201 (25.09%) dengue-positive patients reported vomiting, abdominal pain, rashes, and cough, respectively. Other symptoms in dengue-positive patients included nosebleed (86, 10.73%), hematuria (102, 12.73%), and shock (103, 12.85%) (Table 3).
On the basis of symptoms, dengue-positive patients were categorized into mild, moderate, and severe infection groups. Of the 801 dengue-positive patients, 436 (54.43%) exhibited mild symptoms, 284 (35.45%) were moderately affected, and 81 (10.11%) developed severe conditions. Among the severe cases, headaches (72, 89%), vomiting (64, 79.1%), abdominal pain (29, 72.5%), rashes (56, 69.2%), cough (37, 45.8%), shock (69, 85.2%), hematuria (25, 30.9%), and nosebleed (25, 30.9%) were prevalent. These findings indicate that severe dengue infections are associated with more pronounced and serious symptoms, as compared to moderate and mild infections.
Table 3.Clinical Manifestations of Suspected and Dengue-positive Patients| Clinical Symptoms | DENV-Negative 1599 (66.625%) |
DENV-Positive 801 (33.375%) |
DENV-Mild 436 (18.16%) |
DENV-Moderate 284 (11.833%) |
DENV-Severe 81 (3.375%) |
|---|---|---|---|---|---|
| Fever | 1599 (100) | 801 (100) | 436 (100) | 284 (100) | 81 (100) |
| Headache | 945 (59.1) | 559 (69.78) | 274 (62.84) | 213 (75) | 72 (89) |
| Vomiting | 529 (33.0) | 394 (49.2) | 150 (34.4) | 180 (63.4) | 64 (79.1) |
| Skin rash | 129 (8) | 281 (35.08) | 110 (25.22) | 115 (40.5) | 56 (69.2) |
| Muscles pain | 1201 (75) | 801 (100) | 436 (100) | 284 (100) | 81 (100) |
| Fatigue | 1009 (63.1) | 753 (94.0) | 388 (88.99) | 284 (100) | 81 (100) |
| Nose bleed | 0 | 86 (10.73) | 11 (2.52) | 50 (17.772) | 25 (30.9) |
| Cough | 401 (25) | 201 (25.09) | 61 (14.0) | 103 (36.3) | 37 (45.8) |
| Abdominal pain | 161 (10.1) | 299 (37.32) | 127 (29.12) | 108 (38.1) | 64 (79.1) |
| Hematuria | 0 | 102 (12.73) | 13 (2.98) | 64 (22.6) | 25 (30.9) |
| Shocks | 0 | 103 (12.85) | 0 | 34 (12.0) | 69 (85.2) |
|
Technique Name |
Tested Cases |
Positive Cases (%) |
Sensitivity (%) |
|
|---|---|---|---|---|
|
ICT |
||||
|
NS1 |
2400 |
801 |
88.9 |
|
|
IgM |
2400 |
270 |
69.2 |
|
|
IgG |
2400 |
81 |
24.8 |
|
|
Overall |
- |
|
71.2 |
|
|
ELISA |
||||
|
NS1 |
969 |
279 (28.79) |
93.3 |
|
|
IgM |
578 |
196(33.91) |
86.3 |
|
|
IgG |
613 |
107 (17.45) |
74.8 |
|
|
Overall |
- |
- |
85.0 |
|
|
PCR |
||||
|
RT-PCR |
240 |
219 |
98.2 |
|
3.4. Incidence of Molecular Biomarkers for RT-PCR
Of the 240 samples selected for molecular analysis, 219 were confirmed positive using RT-PCR. Among these, the most prevalent serotype was DENV-3, accounting for 61.18% of all cases. This was followed by DENV-2 at 25.74% and DENV-1 at 13.69%, while the least documented serotype was DENV-4 at 1.36%, as detailed in Table 5.
Table 5.Distribution of Dengue Serotypes| Serotype | Positive | Percentage (%) |
|---|---|---|
| DENV-1 | 30 | 13.70 |
| DENV-2 | 52 | 23.74 |
| DENV-3 | 134 | 61.19 |
| DENV-4 | 3 | 1.37 |
| Total | 219 | 100.0 |
3.5. Blood Biomarkers and Disease Level of Dengue Patients
Various blood biomarkers were evaluated to determine disease severity among mild, moderate, and severe groups. A significant decrease in platelet count (thrombocytopenia) was observed in both the moderate (149.96±31.83 μl) and severe (64.24±108.74 μl) group (p-value < 0.05). The hematocrit level was notably elevated in the severe group (38.04±8.90, 95 % CI), which indicates RBC concentration as a result of plasma leakage. Conversely, WBC count was statistically insignificant across all groups (p-value > 0.05). Bivariate analysis showed a strong positive correlation between platelet count (μl) and WBC count (10^9/l) (r= 0.467, p= 0.000), as detailed in Table 6.
Table 6. Blood Biomarkers at Different Disease Levels| Biomarkers | Total n = 801 |
Mild n = 436 (95% CI) |
Moderate n = 284 (95% CI) |
Severe n = 81 (95% CI) |
p-value |
|---|---|---|---|---|---|
| Neutrophils (%) | 68.39±14.84 (67.36–69.42) |
69.93±14.55 (68.56–71.30) |
67.57±14.91 (65.83–69.32) |
62.96±14.83 (59.68–66.24) |
0.001 |
| Platelets count (μl) | 205.35±96.76 (198.64–212.07) |
267.80±69.02 (261.3–274.3) |
149.96±31.83 (146.2–153.68) |
64.24±108.74 (40.20–88.29) |
0.001 |
| Lymphocytes count (%) | 21.91±13.32 (20.98–22.83) |
20.31±12.80 (19.11–21.52) |
22.80±13.75 (21.19–24.41) |
27.32±12.98 (24.45–30.20) |
0.05 |
| WBCs (109/l) | 6.23±3.16 (6.01–6.45) |
7.18±3.31 (6.87–7.49) |
5.02±2.14 (4.77–5.27) |
5.36±3.62 (4.56–6.16) |
0.05 |
| Hematocrit (%) | 37.39±5.68 (37.00–37.70) |
36.72±5.08 (36.24–37.20) |
38.24±5.26 (37.63–38.86) |
38.04±8.90 (36.07–40.01) |
0.005 |
| Hemoglobin (g/dl) | 13.33±2.04 (13.19–13.48) |
13.03±1.81 (12.85–13.20) |
13.74±1.89 (13.52–13.96) |
11.56±3.17 (11.87–13.26) |
0.001 |
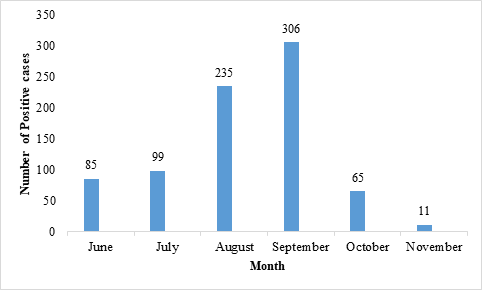
3.6. Month-wise Incidence of Dengue Fever
The current study reported dengue incidence from June 2022 to November 2022. The month of September was marked with the highest number of cases (n=306, 38.25%), followed by August (n=235, 29.38%), July (99, 12.35%), June (85, 10.63%), October (65, 8.13%), and November (11, 1.37%), as shown in Figure 1.
4. DISCUSSION
There has been an exponential rise in dengue cases in Pakistan for the last two decades due to climate change, particularly floods [14][15]. The incidence of this mosquito-borne viral disease has increased significantly in tropical and subtropical regions. In Pakistan, dengue infection has become more prevalent over the years, with all four serotypes reported in various regions, often with severe consequences [1][3][9][16][17]. This study aimed to evaluate the molecular and blood biomarkers associated with the severity of dengue fever in Peshawar, Pakistan. A total of 2400 suspected serum samples were analyzed for dengue virus infection using various immunoassay techniques.
Among these samples, 801 (33.37%) were confirmed as dengue-positive using immunological tests detecting anti-dengue antibodies. Previous studies determined these tests as the most efficient and convenient method to detect the acute phase of dengue infection [16][18][19]. The current study evaluated the diagnostic accuracy of various immunoassay techniques, such as ICT and ELISA, at the early stage of DENV infection. The overall sensitivity of ICT was observed as 71.1%, with NS1 value of 88.9% and IgM and IgG values of 69.2% and 24.8%, respectively. Similarly, ELISA showed greater sensitivity (85.0%) in identifying NS1 (93.3%), IgM (86.3), and IgG (74.8%). Comparatively, ELISA was found to have greater sensitivity than ICT due to its comprehensive diagnostic accuracy and minimum false reading. In this regard, the findings are consistent with previous studies [19][20].
The current study also evaluated 240 dengue samples using RT-PCR. Of these, 219 (91.2%) were confirmed positive for dengue virus, along with DENV serotypes. The most commonly reported serotype was DENV-3 (61.19%), followed by DENV-2 (23.74%), and DENV-1 (13.70%), while the least frequent was DENV-4 (1.37%). These findings align with the findings of other studies in Pakistan [1][3] but contrast with studies conducted in other regions where DENV-2 was found to be more prevalent [21].
The study recorded a higher infection rate in men (56.05%) as compared to women (43.95%), which is consistent with previous research [17][22]. This gender disparity may be due to cultural factors, as men are more active outdoors and thus more exposed to mosquito bites, while women are generally more restricted in their outdoor activities. However, some studies have reported different gender-related findings [23][24]. The current study also revealed the highest number of cases in 16–30 years old (45%), which aligns with other reports [15][25][26][27], but differs from studies showing higher infection rates among children [16, 24]. This variation may be due to differences in immune status, past exposure to different serotypes, and delays in seeking medical care.
This study also revealed the highest dengue incidence in the month of September (38.25%), followed by August (29.375%). This trend is consistent with previous studies indicating that the post-monsoon season, which favors mosquito propagation, is more susceptible to dengue outbreaks [1][14][28]. Another study argued that the transmission of dengue virus is strongly associated with humid conditions which supports the propagation of the Aedes aegypti mosquito [20].
According to WHO, clinical manifestations are crucial to detect and monitor dengue virus infection [25, 26, 30]. In this study, the most common symptoms among dengue-positive patients were high fever (100%), muscle pain (100%), headache (69.78%), vomiting (49.2%), rashes (25.08%), and abdominal pain (37.32%). These symptoms are consistent with other reports on dengue infection [29][31][32], although some studies reported different clinical outcomes, possibly due to variations in the virus strain or virulence factors [21].
Furthermore, thrombocytopenia was observed in 365 dengue-positive patients (moderate and severe cases). This decrease in platelet level is consistent with other studies and may be due to abnormalities in megakaryocytes and bone marrow suppression [15][16][33]. Additionally, a significant increase in hematocrit level was noted in severe cases, likely due to blood vessel permeability and plasma leakage. A decrease in HB level was also observed in severe cases, possibly due to hemolysis [16][18].
4.1. Conclusion
This study highlighted the increasing risk of the prevalence of dengue virus infection in Peshawar district, KPK, Pakistan. Evidence suggests that certain factors such as climate change, urbanization, and the presence of different dengue serotypes are responsible for the dengue burden. It was concluded that effective vector control programs, improved community education campaigns, and weather monitoring strategies are critical to manage the transmission period as well as future outbreaks.
CONFLICT OF INTEREST
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Ali S, Salman M, Din M, Khan K, Ahmad M, Khan FH, Arif M. Dengue outbreaks in Khyber Pakhtunkhwa (KPK), Pakistan in 2017: an integrated disease surveillance and response system (IDSRS)-based report. Polish J Microbiol. 2019;68(1):115–119. https://doi.org/10.21307/pjm-2019-013
- World Health Organization. Dengue and Severe Dengue (2024). WHO Web site. https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue. Accessed January 21, 2025.
- Anwar F, Tayyab M, Salman M, et al. Dengue outbreak 2018 in district Shangla KPK; clinical features and laboratory markers of dengue virus infection. Future Virol. 2020;15(10):693–699. https://doi.org/10.2217/fvl-2019-0130
- Boulaaras S, Jan R, Khan A, Ahsan M. Dynamical analysis of the transmission of dengue fever via Caputo-Fabrizio fractional derivative. Chaos Solitons Fractals: X. 2022;8:e100072. https://doi.org/10.1016/j.csfx.2022.100072
- Morra ME, Altibi AM, Iqtadar S, et al. Definitions for warning signs and signs of severe dengue according to the WHO 2009 classification: systematic review of literature. Rev Med Virol. 2018;28(4):e1979. https://doi.org/10.1002/rmv.1979
- Abdul-Ghani R, Mahdy MA, Al-Eryani SM, et al. Impact of population displacement and forced movements on the transmission and outbreaks of Aedes-borne viral diseases: Dengue as a model. Acta Tropica. 2019;197:e105066. https://doi.org/10.1016/j.actatropica.2019.105066
- Haider Z, Ahmad FZ, Mahmood A, et al. Dengue fever in Pakistan: a paradigm shift; changing epidemiology and clinical patterns. Perspect Public Health. 2015;135(6):294–298. https://doi.org/10.1177/1757913915599019
- Rai MA. Control of dengue fever in Pakistan. Nature. 2011;479:e41. https://doi.org/10.1038/479041d
- Rasheed SB, Butlin RK, Boots M. A review of dengue as an emerging disease in Pakistan. Pub Health. 2013;127(1):11–17. https://doi.org/10.1016/j.puhe.2012.09.006
- Khan J, Khan I, Amin I. A comprehensive entomological, serological and molecular study of 2013 dengue outbreak of Swat, Khyber Pakhtunkhwa, Pakistan. PloS One. 2016;11(2):e0147416. https://doi.org/10.1371/journal.pone.0147416
- Khan J, Khan A. Incidence of dengue in 2013: dengue outbreak in District Swat, Khyber Pakhtunkhwa, Pakistan. Inter J of Fauna and Biolo Stud. 2015;2(1):1–7.
- World Health Organization. Dengue-Pakistan (2022). WHO Web site. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON414. Accessed November 1, 2023.
- World Health Organization. Dengue fever – Pakistan. WHO Web site. https://www.who.int/emergencies/disease-outbreak-news/item/dengue-fever-pakistan. Updated October 11, 2024.
- Paranavitane SA, Gomes L, Kamaladasa A, et al. Dengue NS1 antigen as a marker of severe clinical disease. BMC Infect Dis. 2014;14(1):1–7. https://doi.org/10.1186/s12879-014-0570-8
- Urooj H, Altaf S, Saadat E, Qadir MS, Moiz B. Characterization of thrombocytopenia in pediatric patients in noncritical hospital setting: an institutional review from Pakistan. J Pediat Hematol/Oncol. 2025;47(1):1–6. https://doi.org/10.1097/MPH.0000000000002972
- Kashif M, Afzal M, Zeshan B, Javed H, Batool S, Mazhar M. Molecular and haematological analysis of dengue virus-3 among children in Lahore, Pakistan. Jundishapur J Microbiol. 2021;14(1):e109512. https://doi.org/10.5812/jjm.109512
- Rehman AU, Anwar F, Tayyab M, et al. Incidence of Dengue fever, serotypes, clinical features, and laboratory markers: a case study of 2019 outbreak at district Shangla, KP, Pakistan. Afr Health Sci. 2022;22(1):521–531. https://doi.org/10.4314/ahs.v22i1.61
- Kulkarni RD, Patil SS, Ajantha GS, et al. Association of platelet count and serological markers of dengue infection-importance of NS1 antigen. Indian J Med Microbiol. 2011;29(4):359–362. https://doi.org/10.4103/0255-0857.90159
- Pal S, Dauner AL, Mitra I, et al. Evaluation of dengue NS1 antigen rapid tests and ELISA kits using clinical samples. PLOS ONE. 2014;9(11):e113411. https://doi.org/10.1371/journal.pone.0113411
- Khan J. Pakistan reports 2,795 dengue cases in last seven days. ARY Web site. https://arynews.tv/pakistan-reports-2795-dengue-cases-in-last-seven-days/. Accessed January 21, 2025.
- Hakim R, Bibi S, Ali Q, et al. Molecular epidemiology of dengue virus circulating during 2021 outbreak in Pakistan. Future Virol. 2023;18(9):545–555. https://doi.org/10.2217/fvl-2022-0196
- Wahala WM, Kraus AA, Haymore LB, Accavitti-Loper MA, de Silva AM. Dengue virus neutralization by human immune sera: role of envelope protein domain III-reactive antibody. Virology. 2009;392(1):103–113. https://doi.org/10.1016/j.virol.2009.06.037
- Saud B, Adhikari S, Maharjan L, Paudel G, Amatya N, Amatya S. An epidemiological prospective of focal outbreak of dengue infection in Kathmandu, Nepal. J Clinic Virol Plus. 2022;2(1):e100063. https://doi.org/10.1016/j.jcvp.2022.100063
- Farrukh AM, Ganipineni VD, Jindal U, et al. Prevalence and outcomes of Myocarditis in dengue viral fever: A systematic review and Meta-analysis. Curr Prob Cardiol. 2023:e102029. https://doi.org/10.1016/j.cpcardiol.2023.102029
- Haider Z, Ahmad FZ, Mahmood A, et al. Dengue fever in Pakistan: a paradigm shift; changing epidemiology and clinical patterns. Perspect Public Health. 2015;135(6):294–298. https://doi.org/10.1177/1757913915599019
- Shams N, Amjad S, Yousaf N, Ahmed W, Seetani NK, Farhat S. Dengue knowledge in indoor dengue patients from low socioeconomic class; etiology, symptoms, mode of transmission and prevention. J Ayub Med College Abbott. 2018;30(1):40–44.
- Shahid M, Amin I, Afzal S, et al. Prevalence and molecular detection of dengue virus in 2013 outbreak in KPK and Punjab, Pakistan. Pak J Zool. 2017;49(3):1119–1122. https://doi.org/10.17582/journal.pjz/2017.49.3.sc4
- Abdullah, Ali S, Salman M, Khan M. A looming twindemic of COVID-19 and dengue on post-flood scenario in the developing countries. Asian Pacific J Trop Med. 2022;15(9):383–384. https://doi.org/10.4103/1995-7645.356990
- Khan J, Ghaffar A, Khan SA. The changing epidemiological pattern of Dengue in Swat, Khyber Pakhtunkhwa. PLOS ONE. 2018;13(4):e0195706. https://doi.org/10.1371/journal.pone.0195706
- Ahmed S, Arif F, Yahya Y, et al. Dengue fever outbreak in Karachi 2006--a study of profile and outcome of children under 15 years of age. J Pak Med Assoc. 2008;58(1):4–8.
- Suleman M, Faryal R, Alam MM, et al. Dengue virus serotypes circulating in Khyber Pakhtunkhwa province, Pakistan, 2013–2015. Ann Labor Med. 2017;37(2):e151. https://doi.org/10.3343/alm.2017.37.2.151
- Srikiatkhachorn A, Gibbons RV, Green S, et al. Dengue hemorrhagic fever: the sensitivity and specificity of the World Health Organization definition for identification of severe cases of dengue in Thailand, 1994–2005. Clinic Infect Dis. 2010;50(8):1135–1143. https://doi.org/10.1086/651268
- Anwar F, Ullah S, Aziz AU, et al. Epidemiological and hematological investigation of dengue virus infection. Microbiol Immunol. 2022;66(9):426–432. https://doi.org/10.1111/1348-0421.13018