
| Review | Open Access |
|---|
Exploring Sustainability through the Lens of Pakistani Artists |

|
|---|
![]() Fariha Rashid* and Suffah Naeem
Fariha Rashid* and Suffah Naeem
University of Home Economics, Lahore, Pakistan
Background. Hepatitis C virus (HCV) is a blood-borne infection that has spread all over the world. Around 10 million people in Pakistan are impacted by HCV, while over 58 million people worldwide have a chronic HCV infection. HCV is well known for its severe effects on the liver as well as its extra-hepatic manifestations.
Objective. This study assessed the renal profile (urea and creatinine), hematological factors (Hb, HCT, MCV), and diabetic profile (blood glucose fasting, blood glucose random, and HbA1c) of HCV-positive patients confirmed by real-time PCR (RT-PCR). The main aim was to determine the impact of hepatitis infection.
Methodology. This was a retrospective cohort study conducted on patients diagnosed as HCV-positive by using real-time PCR (RT-PCR). Their diabetic, renal, and hematological association with HCV was observed and analyzed by using SPSS 25.
Results. Out of 296 HCV-positive patients, 174 (58.8%) were male and 122 (41.2%) were female, indicating that HCV was found to be more prevalent in male patients. There was no statistical association found between HbA1c and gender. However, there was found a significant association of blood glucose fasting and blood glucose random with gender. Renal and hematological profiles were also disturbed in HCV-infected individuals.
Conclusion. Health professionals may benefit from this study by managing disrupted profiles more effectively and providing improved patient care. Additional research on the disrupted hematological, renal, and diabetic profiles may improve the treatment conditions for patients since these profiles revealed a variety of extra-hepatic symptoms in this study.
Highlights
- This study examines the impact of HCV infection in 296 HCV-positive patients confirmed by using RT-PCR.
- Assessment of renal profiles (urea and creatinine) and hematological factors (Hb, HCT, MCV) was made.
- To determine the impact of HCV on these profiles, diabetic profiles (blood glucose fasting, blood glucose random, and HbA1c) of the study participants were used.
1. INTRODUCTION
Both infectious viruses and non-infectious substances can induce hepatitis, an inflammation of the liver that can result in a number of health issues, some of which are fatal. The hepatitis virus comes in five primary strains known as A, B, C, D, and E. An estimated 354 million individuals worldwide have hepatitis B or C. For the majority, diagnosis and treatment remain out of reach. Also, many hepatitis patients remain unaware that they are infected since they do not exhibit any symptoms [1]. Acute infection symptoms can arise anywhere from two weeks to six months following exposure. Acute hepatitis may cause fever, exhaustion, appetite loss, nausea, vomiting, abdominal discomfort, light-colored feces, dark urine, joint pain, and jaundice [2].
The Hepatitis C virus has two phases: the acute phase and the chronic phase [3]. The acute phase of HCV resolves in six months. If it does not, there is a transition towards the chronic phase of the virus [4]. In western nations, HCV infection is the primary cause of hepatocellular carcinoma (HCC), one of the main causes of chronic liver diseases and a key predictor of liver transplantation. A WHO global hepatitis report from 2023 states that an estimated 58 million people worldwide are chronically infected with HCV, while 1.5 million new cases are reported annually. The estimates of the total prevalence of HCV infection worldwide range from 2.9% in Africa to 1.3% in the Americas, with a global viremia of 2.5% (177.5 million adults with HCV infection) [5]. As of January 1, 2021, an estimated 9,746,000 (7,573,000–10,006,000) Pakistanis had HCV viremia, representing a 4.3% viremia prevalence [5]. With an incidence rate of 205 per 100,000, 462,000 incident infections were predicted in 2021. Of the 9.7 million cases of viremia infections, 21% (2,010,000) had been identified by the end of the year [6]. With a prevalence of 10.10% and 51.0% respectively, blood transfusion and injectable medication usage were the two most frequent exposures linked to the spread of HCV [7].
In addition to liver problems, HCV infection can also affect other organs, leading to symptoms not related to the liver. Up to 38-76% of individuals with chronic HCV experience at least one extrahepatic symptom. Individuals with type 2 diabetes (T2DM) are more likely to have chronic hepatitis C [8]. Indeed, the risk of diabetes increases with chronic HCV infection. This is because the liver, which is involved in the storage of glucose, is impacted by the virus. If the liver cannot function adequately, it might lead to excessive blood glucose level and insulin resistance [9]. Also, HCV can directly affect the kidneys and renal functioning, which can result in various nephropathies. Although HCV may induce glomerular illness by immune complex deposition, the virus may also cause chronic inflammation, increased atherosclerosis, and insulin resistance in addition to its direct cytotoxic effect on renal tissue [10].
Variation in hematological parameters is another effect of HCV. Reduced levels of hematocrit (HCT) and hemoglobin (Hb), as well as a reduced red blood cell (RBC) count, are the outcomes of immune system changes brought on by specific stimuli [11]. One of the most well-known extra-hepatic symptoms of HCV is anemia [10]. Other than these symptoms, HCV also affects cardiovascular [12] and nervous systems, causing atherosclerosis and neuropsychiatric disorders [13]. Recognizing that viral hepatitis poses a public health threat on par with human immunodeficiency virus (HIV), malaria, and tuberculosis, the World Health Organization (WHO) published its first global health sector strategy in June 2016 and set forth the goal of the elimination of viral hepatitis as a major public health threat by 2030 [14].
Keeping in view the above, this study seeks to ascertain the impact of hepatitis infection on hematological factors (hemoglobin, hematocrit, mean corpuscular volume) and diabetic profiles (blood glucose fasting, blood glucose random, and HbA1c) in patients diagnosed with HCV infection by using Real-Time PCR (RT-PCR).
2. MATERIAL AND METHODS
The current study used a retrospective cohort design. Total of 296 HCV-positive (RT-PCR) samples were gathered from a community near Shalamar Hospital in Lahore, Pakistan. Purposive sampling, which is non-probability in nature, was used to gather samples. Data was collected from both male and female patients who were more than 18 years old and diagnosed with HCV by using RT-PCR. The patients' histories were used to evaluate the exclusion criterion. The study excluded the participants with autoimmune disorders, type 1 diabetes mellitus, cirrhosis, non-alcoholic fatty liver disease, and chronic kidney disease, as well as dialysis patients. The patients’ data was only accessible to the research team. The Shalamar School of Allied Health Sciences Ethics Committee gave its approval to this study (SSAHS-IRB/AL/17/2023).
2.1. Real-Time PCRThe HCV RNA in human plasma or serum from infected persons was quantified using the Abbott real-time hepatitis in vitro polymerase chain reaction (RT-PCR) test. The device is made to handle specimens in an ongoing workflow. The Abbott m24sp extraction unit, along with the Abbott m2000rt amplification and detection equipment, was used to perform the test [11].
2.2. Diabetic ProfileThe diabetic profile of patients which included random and fasting blood glucose was analyzed using Abbot’s Architect c4000 Chemistry Analyzer which works on the principle of electrophoresis. HbA1c (glycated hemoglobin) was analyzed by using D-10 Bio-Rad which works on the principle of HPLC.
2.3. Renal ProfileRenal profile includes urea and creatinine. These were analyzed using Abbott’s Architect c4000 Chemistry Analyzer which works on the principle of electrophoresis.
2.3.1. Hematological Profile. Hematological profile, comprising Hb (hemoglobin), HCT (hematocrit), and MCV (mean corpuscular volume), was examined using Sysmex XP 300™ Automated Hematology Analyzer.
2.4. AnalysisData was entered and analyzed using IBM SPSS Statistics for Windows (version 25.0). Qualitative data, such as gender, was presented in the form of frequency. After fulfilling parametric assumptions, a chi-square test was applied to determine the association between diabetic profile and hepatic infection. The correlation between diabetic profile, hematological factors, and renal function tests was determined using the Pearson correlation coefficient. A p-value of 0.05 or less was considered as significant.
3, RESULTS AND DISCUSSION
To determine the impact of HCV on the three profiles renal (urea, creatinine), hematological (Hb, HCT, and MCV), and diabetic (blood glucose fasting, blood glucose random, and HbA1c) were examined. Among the 296 patients, 174 were male and 122 were female patients.
Numerous studies have revealed that HCV directly affects the liver. Moreover, when it enters the chronic phase, it also results in extra-hepatic manifestations that lead to a variety of illnesses, including diabetes mellitus, chronic kidney disease (which ultimately results in kidney failure), and anemia. Research has also revealed that men are more likely than women to contract HCV [15]. The results from patients with chronic hepatitis C (without cirrhosis) were shown in a previous study alongside normal values. The analysis of 1303 non-hepatopathic controls and 1046 CHC (chronic hepatitis C) patients revealed a substantial increase in the risk of T2DM in CHC patients [16].
Several studies have demonstrated a higher incidence of T2DM in the context of chronic HCV, partly because of the virus's predictable direct impact on insulin resistance and glucose metabolism [17]. Another study revealed that participants (n = 251) had an average follow-up period of 28 ± 13 months. At baseline, 42 (17%) individuals satisfied the criteria for T2DM, while 33 (79%) of these subjects were taking medication for the condition [18]. In this study, of the 296 patients who were administered HbA1c test, 174 were men and 122 were women. There were 83, 174, and 174 male diabetic patients who were administered HbA1c, blood glucose fasting, and blood glucose random tests, respectively (Table 1).
Table 1. Descriptive Statistics of Blood Glucose Fasting, Blood Glucose Random, HbA1C, Urea, Creatinine, Hb, HCT, and MCV
|
Blood Glucose Fasting |
Blood Glucose Random |
HBA1C |
Urea |
Creatinine |
Hb hemoglobin |
HCT hematocrit |
MCV mean corpuscular volume |
|---|---|---|---|---|---|---|---|
|
142.11±66.480 |
202.74± 125.632 |
7.254± 2.5742 |
48.53±45.948 |
1.44± 1.879 |
12.00± 8.191 |
36.89± 7.262 |
84.99±9.396 |
Of the total female patients, 58 had high HbA1c values, 86 had high blood glucose fasting values, and 80 had high blood glucose random values. Given that the p value was 0.9, the statistical analysis revealed no significant correlation between gender and HbA1c. On the other hand, the p value of 0.2 indicated a significant relationship between gender and blood glucose (fasting and random) among patients. The patients with pre diabetes were observed in both sexes (Figure 1). This indicated that although some individuals with chronic hepatitis were already diabetic, others developed diabetes as their condition deteriorated. Numerous investigations have established a strong link between HCV infection and mixed cryoglobulinemia. A study on HCV-related cryoglobulinemic glomerulonephritis in which 87% of the 146 patients had HCV infection. The most common histological characteristic was diffused membrane proliferative glomerulonephritis, which accounted for 83% of infections. More than 1.5 mg/dl (>133 μmol/l) basal creatinine resulted in the worse Kaplan-Meier survival curve [19].
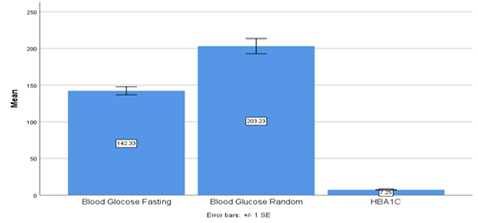
Figure 1. Diabetic Profiles Include HbA1c, Blood Glucose Fasting, and Blood Glucose Random
Out of the 174 male patients included in the current study, 28 were found to have high creatinine levels, 62 had low levels, and the remaining patients had normal levels. Out of the 122 female patients who were administered the test, 98 had elevated levels, while the remaining 115 had normal levels (Table 1). The p-value of 0 indicates a positive and significant relationship between creatinine and gender (Figure 2). According to the results, persons with elevated creatinine readings were found to be susceptible to chronic kidney diseases. According to the findings of the 2017 study by Mohammad Asaduzzaman, 38 patients (79.2% of whom were men and 92.9% of whom were women and positive for the HIV antibody) were classified as anemic because of decreased hemoglobin [10].
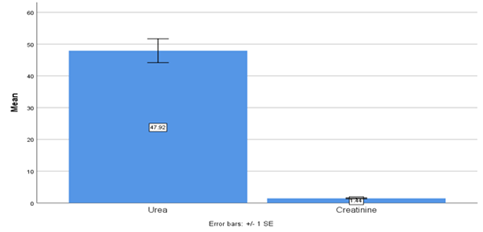
Figure 2. Renal Profiles Including Urea and Creatinine
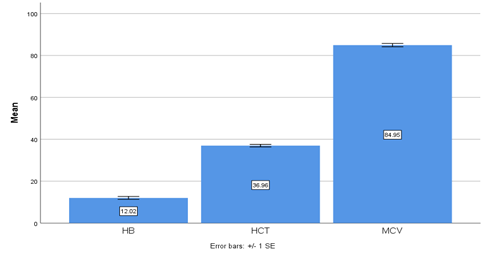
Figure 3. Hematological Profiles Including Hemoglobin (Hb), Hematocrit (HCT), and Mean Corpuscular Volume (MCV)
In a study, the vales of MCV and HCT were calculated as [p = 0.9449] and HCT [p = 0.0328], respectively. The study demonstrated that MCV did not differ between HCV-affected and normal individuals. Moreover, HCT was significantly lower in hepatitis C patients as compared to normal individuals [20]. In the current study, 148 HCV-positive patients were included; of these, 1.4% had a high HCT value, 73.10% had a low HCT value, and 25.0% had a normal HCT value (among male patients). Furthermore, 5.4% had a high HCT value, 38.5% had a low HCT value, and 55.4% had a normal HCT value (among female patients). This demonstrates that HCT is lower in HCV patients as compared to normal persons of both sexes. Similarly, 148 HCV-positive individuals who participated in this study had their MCV analyzed; of these, 4.7% had a high MCV value, 29.1% had a low MCV value, and 65.5% had a normal MCV value (Figure 3). Given that 65.5% of patients had an MCV value within normal range, this indicates that HCV does not impact MCV (Table 1).
3.1. ConclusionThe diabetic profiles (blood glucose fasting and blood glucose random), renal profiles (urea and creatinine), and hematological profiles (Hb, HCT, and MCV) of HCV-positive patients showed significant variation with gender. On the other hand, HbA1c showed no significant variation. However, the viral load of disrupted profiles, which could aid in a better understanding of the association and evaluation of patient treatments, were not included in this study.
AUTHOR CONTRIBUTION
Tahira Idrees: data curation. Tahira Batool: supervision; writing – original draft. Rukhsar Akbar: investigation, formal analysis. Rabbia Mutaqeen: formal analysis. Asma Irshad: data curation, formal analysis.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
Data supporting the findings of this study will be made available by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
GENERATIVE AI DISCLOSURE STATEMENT
The authors did not used any type of generative artificial intelligence software for this research.
REFERENCES
- Kaplan DE. Hepatitis C virus. Ann Int Med. 2020;173(5):ITC33–ITC48. https://doi.org/10.7326/AITC202009010
- Roger S, Ducancelle A, Le Guillou-Guillemette H, Gaudy C, Lunel F. HCV virology and diagnosis. Clinics Res Hepatol Gastroenterol. 2021;45(3):e101626. https://doi.org/ 10.1016/j.clinre.2021.101626
- Masia R, Misdraji J. Liver and bile duct infections. Diagnost Pathol Infect Dis. 2018:272–322. https://doi.org/10.1016/B978-0-323-44585-6.00011-4
- Guntipalli P, Pakala R, Gara SK, et al. Worldwide prevalence, genotype distribution and management of hepatitis C. Acta Gastro Belg. 2021;84(4):637–656.
- Mooneyhan E, Qureshi H, Mahmood H, et al. Hepatitis C prevalence and elimination planning in Pakistan, a bottom‐up approach accounting for provincial variation. J Viral Hepatitis. 2023;30(4):345–354. https://doi.org/ 10.1111/jvh.13802
- Arshad A, Ashfaq UA. Epidemiology of hepatitis C infection in Pakistan: current estimate and major risk factors. Critic Rev in Eukaryotic Gene Expr. 2017;27(1):63–77. https://doi.org/ 10.1615/CritRevEukaryotGeneExpr.2017018953
- Negro F. Natural history of hepatic and extrahepatic hepatitis C virus diseases and impact of interferon-free HCV therapy. Cold Spring Harbor Perspect Med. 2020;10(4):ea036921. https:// doi.org/10.1101/cshperspect.a036921
- Chakraborty AK, Swapnil MAM, Al Mamun A, Karim F, Dey U. Association of Biochemical Markers between Hepatitis C Virus and Diabetes Mellitus among Bangladeshi Male. Insight. 2022;5(01):190–197.
- Henson JB, Sise ME. The association of hepatitis C infection with the onset of CKD and progression into ESRD. Seminars Dialysis. 2019;32(2):108–118. https://doi.org/10.1111/sdi.12759
- Asaduzzaman M, Bappy SR, Fatema B, et al. Effect of hepatitis C virus (HCV) on hemoglobin, blood cells and random blood glucose levels among serologically positive HCV patients. IOSR J Nurs Health Sci. 2017;6(5):41–45.
- Takei F, Tani H, Matsuura Y, Nakatani K. Detection of hepatitis C virus by single-step hairpin primer RT-PCR. Bioorg Med Chem Letters. 2014;24(1):394–396. https://doi.org /10.1016/j.bmcl.2013.10.021
- Abdel-Gawad M, Nour M, El-Raey F, Nagdy H, Almansoury Y, El-Kassas M. Gender differences in prevalence of hepatitis C virus infection in Egypt: a systematic review and meta-analysis. Sci Rep. 2023;13(1):e2499. https:// doi.org/10.1038/s41598-023-29262-z
- Fabiani S, Fallahi P, Ferrari SM, Miccoli M, Antonelli A. Hepatitis C virus infection and development of type 2 diabetes mellitus: systematic review and meta-analysis of the literature. Rev Endocr Metabol Disord. 2018;19:405–420. https://doi.org/ 10.1007/s11154-017-9440-1
- Chaudhury CS, Sheehan J, Chairez C, et al. No improvement in hemoglobin A1c following hepatitis C viral clearance in patients with and without HIV. J Infect Dis. 2018;217(1):47–50. https://doi.org/10.1093/infdis/jix517
- Roccatello D, Fornasieri A, Giachino O, et al. Multicenter study on hepatitis C virus–related cryoglobulinemic glomerulonephritis. Am J Kidney Dis. 2007;49(1):69–82. https://doi.org/ 10.1053/j.ajkd.2006.09.015
- Rasheed H, Khawar MB, Sohail AM, et al. Altered hematological parameters in HCV infection: a diagnostic approach. Asian J Health Sci. 2022;8(2):eID46.
- Guo F, Moellering DR, Garvey WT. Use of HbA1c for diagnoses of diabetes and prediabetes: comparison with diagnoses based on fasting and 2-hr glucose values and effects of gender, race, and age. Metabol Synd Relat Disord. 2014;12(5):258–268. https://doi.org/10.1089/met.2013.0128
- Negro F, Alaei M. Hepatitis C virus and type 2 diabetes. World J Gastroenterol. 2009;15(13):1537–1547. https://doi.org/10.3748/wjg. 15.1537
- Bhattacharya D, Aronsohn A, Price J, Lo Re V. Clinical practice guidance for testing, managing, and treating Hepatitis C virus infection: 2023 Update by AASLD-IDSA. Clinic Infect Dis. 2023:eciad319. https://doi.org/10.1093/cid/ciad319
- Lam L, Fontaine H, Lapidus N, et al. Impact of direct‐acting antiviral treatment for hepatitis C on cardiovascular diseases and extrahepatic cancers. Pharmacoepidemiol Drug Safety. 2023;32(4):486–495. https://doi.org/10.1002/pds.5576