
| Review | Open Access |
|---|
Development of Microbial Biofilms and their Role in Device, Non-Device, and Organ System-Level Infections |
 |
|---|
![]() Farah Liaqat1 , Waiza Ansar2, Noor Muhammad2*, Maria Tariq3, Zahid Nazir2, Hafiz Muhammad Ghuffran Qamar4 and Iram Liaqat2
Farah Liaqat1 , Waiza Ansar2, Noor Muhammad2*, Maria Tariq3, Zahid Nazir2, Hafiz Muhammad Ghuffran Qamar4 and Iram Liaqat2
1Department of Zoology, University of Sialkot, Pakistan
2Microbiology Laboratory Department of Zoology, GC University, Lahore, Pakistan
3Department of Zoology, Education University, Lahore, Pakistan
4Department of Chemistry, GC University, Lahore, Pakistan
Background. Microorganisms, while providing many health benefits to human beings and other living organisms, are also responsible for significant infections. They cause infections in both planktonic and biofilm modes. Biofilms, defined as architectural communities of microorganisms encased in an extracellular polymeric substance (EPS), are strongly associated with infections. According to the National Institute of Health Sciences (NIH), biofilms account for 65% of microbial infections and 80% of chronic infections.
Methods. This review examines the current literature on microbial biofilms, focusing on their formation stages, pathogenicity, resistance mechanisms, and associated infections. Data from various studies is analyzed to summarize biofilm development and its role in chronic infections.
Results. Biofilm development involves four stages: attachment, microcolony formation, maturation, and dispersion. Quorum sensing (QS) mechanisms play a critical role in biofilm development and microbial communication. Biofilms enhance microbial pathogenicity and resistance to both the immune system and commercial antibiotics. They contribute to device-associated infections, such as those in catheters, and also to non-device infections in living tissues, as well as organ-level infections that impair systemic functions.
Conclusion. A comprehensive understanding of microbial biofilms is essential for developing strategies to manage and control biofilm-associated infections. This review highlights the need for further research on the mechanisms of biofilm formation and resistance to improve infection prevention and treatment.
Highlights
- Biofilms are associated with 65% of microbial infections and 80% of chronic infections, highlighting their significant role in disease development.
- Biofilm development occurs in four stages—attachment, microcolony formation, maturation, and dispersion—with quorum sensing playing a vital role in microbial communication.
- Microbial biofilms increase pathogenicity, enhance resistance to the immune system and antibiotics, and contribute to device-related and organ-level infections.
GRAPHICAL ABSTRACT

1. INTRODUCTION
Microorganisms are microscopic organisms that the naked eye cannot see. They are prokaryotic living organisms that live freely or in the form of colonies; this community is called biofilm. In a biofilm, microbes live in an arranged and ordered form inside an extracellular polymeric substance (EPS) produced by them. They are usually attached to a surface which can be either living or non-living and also to each other. In the biofilm mode, microorganisms show differentiation in gene expression and growth, as compared to the planktonic mode [1].
Biofilm is an advanced form of living because by adopting this mode, microbes can develop a better relationship with the host by creating a protective cover around themselves. This mode of living also increases their survival rate, as it protects them from external environmental changes and also from the danger posed by antibiotics and other harmful chemical compounds [2]. Unfortunately, the biofilm mode of living is associated with antibiotic resistance development. It also increases the infection rate in the host by forming persistent cells that are hard to manage. Recently, many studies reported that biofilms are the primary cause of emerging antibiotic resistance in microbes causing pathogenic infections [2]. Biofilm-forming microbes are found everywhere globally, whether in living or non-living structures. They are found in medical implants, hospital floors, water channels, food processing units, living tissues, catheters, and pipes, among others [3]. Microbial growth rate, metabolic activities, and antibiotic resistance are also associated with gene expression and phenotype changes in microbial cells influenced by biofilms. An increased virulence factor is also associated with the biofilm mode of living [4].
According to the National Health Institute (NIH), biofilms of microbes induce 65% of microbial and 80% of chronic infections. Further, microbes in biofilm mode infect both living tissues and medical implants. Some of the infected medical implants include joint prostheses, contact lenses, breast implants, tissue fillers, urinary catheters, vascular grafts, mechanical heart valves, ventricular shunts, ventricular-associated devices, pacemakers, defibrillators, and endotracheal tubes [5]. Dental plaques, lung infections, chronic tonsillitis, chronic wounds, chronic laryngitis, cystic fibrosis, urinary tract infections, and endocarditis are caused by microbial biofilms [6]. Similarly, the Center for Disease Control reported that biofilms are responsible for 500,000 deaths and 1700,000 hospital-acquired infections around the globe. The Center further noted that biofilms cause 11,000 million dollars in economic loss, annually [7]. Some food industries, such as dairy, aquaculture, and poultry, are highly affected by biofilm-forming microbes. These microbes are responsible for losses in these industries as they spoil food, which causes disease outbreaks and deaths [8].
This literature review aims to examine the role of microbial biofilms in chronic infections, focusing on the formation, structure, and impact of microbial biofilms. The aim is to highlight their contribution to antibiotic resistance, persistence, and increased virulence. Furthermore, this review explores their involvement in infections, both among living tissues and medical implants, emphasizing the need for effective strategies to manage and prevent biofilm-associated infections and losses.
2. STAGES OF BIOFILM DEVELOPMENT
In this study, different stages of biofilm formation are depicted sequentially: free-floating planktonic cells undergo reversible attachment to a surface, followed by irreversible attachment, leading to microcolony formation. Over time, the biofilm matures into a complex structure embedded in an extracellular polymeric matrix, culminating in the dispersion of cells to colonize new surfaces.
2.1 Surface ColonizationBiofilm development is a complex process which involves many stages. In this process, free-living planktonic microbes start living in a biofilm. However, the biofilm development process depends on many factors including pH, temperature, hydrodynamic forces, gravitational forces, nature of the surface (for attachment), quorum sensing, Brownian movements, secondary messengers, and many other signaling molecules [9, 10]. There are four main stages of biofilm development, as depicted in Figure 1.
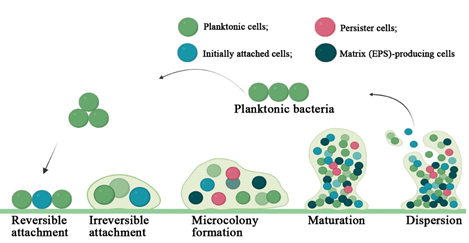
Figure 1. Stages of Biofilm Formation. Adapted according to Abera et al. [11]
2.2. AttachmentInitially, the planktonic microbes start to adhere to the surface of their choice. This is one of the crucial stages as microbial cells organize and colonize the selected surface in this stage [2]. At the start, microbes loosely attach to the surface, which can be reversible. Polarly attached microbes play a fundamental role in this stage. Afterwards, the microbes change their orientation and the attachment becomes irreversible [2]. The biofilm-forming microbes produce a compound known as (bis-(3’-5’)-cyclic dimeric guanosine monophosphate (c-di-GMP)), which acts as an intracellular signaling molecule. This molecule inhibits the free movement of microbial cells and enhances matrix production for the respective biofilm [12]. Pil-Chp surface sensing mechanisms present on the surface of microbial cells enhance c-di-GMP concentration with each event of attachment and detachment. Another mechanism involved in the attachment stage is the conversion of planktonic microbial cells which have low c-di-GMP concentration and haven't faced the surface initially (native planktonic cells). These cells are converted to microbial cells that exhibit a high c-di-GMP concentration (surface sentient cells). At the end of the attachment stage, the attachment becomes irreversible, forming biofilm; then, microbial cells may not leave [13].
2.4. Microcolony FormationAs soon as the microbes successfully attach to the surface, their multiplication begins and the colony size grows in the presence of high c-di-GMP concentration. The colony grows within the self-produced EPS and is known as a microcolony. Interactions among microorganisms and surfaces and cell-to-cell aggregations to form the microcolony highly depend on the motilities of flagella and type IV pili [14].
2.5. MaturationEPS plays an essential role in the maturation of biofilms. It helps the microbial cells to attach to the surface and stabilize the 3D structure of the respective biofilm. Furthermore, it groups microbial cells and protects them from harsh conditions including antimicrobials, host immune response, metallic carbon, and oxidative damage. It also plays a role in cell signaling, a fundamental requirement for enzymes, quorum sensing, and metabolic products [15]. A tower or mushroom shape indicates a mature biofilm, an arrangement of microbial cells per metabolic rate and aero tolerance [16]. Samrot et al. reported that modulins and surfactants may alter the biofilm maturation and quorum sensing mechanism. A mature biofilm comprises three main layers: the outer layer (which consists of microbes ready to leave the biofilm), the middle microbial basement layer, and the inner regulating layer [17].
2.6. DispersionDispersion is the last stage in biofilm development, incorporating both active or passive dispersion. EPS and motility degradation lead to active biofilm dispersion, while physical factors are responsible for passive dispersion. After dispersion, the microbial cells may choose to restart biofilm formation or decide to live a planktonic life. The lack of nutrients, outgrown population, and intense competition are the main natural factors responsible for biofilm dispersion. The degradation of the EPS layer is caused by enzyme action and environmental factors including metabolite accumulation, pH, temperature, and oxygen deficiency, which also influence biofilm dispersion. Some factors decrease EPS synthesis while enhancing motility in microbial cells, which can be another reason for biofilm dispersion [18].
3. QUORUM SENSING (QS) MECHANISM IN BIOFILM FORMATION
As the population of cells in a biofilm increases, a cell-to-cell interaction method known as quorum sensing (QS) synchronizes the gene expression. Biofilm formation and QS mechanisms are two independent processes. As soon as the QS gene is activated, it regulates biofilm development, maturation, and dispersal. The limitation of QS mechanism is that it only works when certain bacteria are found in a minimum quantity. The quantity of autoinducer signaling molecules released by the bacteria in a microcolony can serve as an indicator of the bacterial population within a given volume [19]. However, Laganenka et al. suggested that the autoinducer signaling molecules are only the byproducts of bacterial cells and are not signaling molecules. Therefore, they must not be considered as signaling molecules [20].
To date, various modeling and mathematical approaches have been used to understand the QS mechanism in biofilm formation. Scientists are working to inhibit the QS process in biofilm formation, as it is the essential process required to form a biofilm. By inhibiting the QS mechanism, the biofilm-based infections can be controlled. This has given rise to a new research field called “quorum quenching”, which incorporates the searching and development of quorum quench products. Research on two strong biofilm-former bacterial strains, that is, B. cepacian and P. aeruginosa, also showed reduction in bacterial antibiotic resistance. Thus, the inhibition of QS process would not only control biofilm associated infections but also microbial antibiotic resistance [21].
4. BIOFILM BASED INFECTIONS
About 65% of bacterial infections are caused by bacterial biofilms. Biofilms may cause infections, classified as device/implants and non-device/non-implant associated diseases. Infections for various implants have been reported. About 40% of infections in ventricular-associated implants, 10% of ventricular shunts, 4% of pacemakers and defibrillators, 2% of joint prostheses, and 2% of breast implant infections are caused by bacterial biofilms [22]. Chambers and Bayer reported that bacterial interactions of staphylococci, streptococci, and some other Gram-negative bacteria, with pulmonic valves and vascular endothelium of the heart, cause native valve endocarditis infections [23]. These microbes usually come through the oropharynx, urinary tract, and gastrointestinal tract and access blood and the heart to cause such conditions. When microorganisms adhere to the valve and endothelium and cause damage, the immune system may clear the bacteria, but the injury site often develops a non-bacterial thrombotic endocarditis (NBTE). This condition leads to thrombus formation, characterized by the aggregation of platelets, red blood cells, and fibrin in the affected area [6].
4.1. Device-related Biofilm InfectionsSome unique medical implants such as pacemakers, mechanical heart valves, catheters, urinary tract catheters, contact lenses, peritoneal dialysis catheters, central nervous venous catheters, and prosthetic joints are the main targets of bacterial biofilms inside the body [24]. Mirghani et al. [25] reported that different bacterial species or even a a single species may arrange themselves to form a biofilm. Physiological conditions, duration of implants, and types of devices are some factors that may influence the formation of mature biofilms (Table 1).
Microorganisms may adhere to and target both hard and soft contact lenses. The contact lenses are categorized based on their frequency of disposal, design, construction material, and wear schedule. Staphylococcus epidermidis, Escherichia coli, Staphylococcus aureus, and Pseudomonas aeruginosa are some bacterial species, while Proteus, Serratia, and Candida are some fungal genera, that are mostly reported to target contact lenses and form microbial biofilms [26, 27]. However, the attachment and biofilm formation of these microbes depend on the substrate's nature, water content, electrolyte concentration, microbial composition, and polymer composition. Biofilm formed by P. aeruginosa was observed with the help of an electron microscope on the contact lens of a patient with keratitis. Biofilm formation has been reported also on contact lenses stored in storage boxes, which is why these boxes are considered a source of lens contamination [28].
Gominet et al. [29] reported that central venous catheters are another common target of microbial biofilms. Again, it depends on the duration of catheterization. For instance, the external surface may have more biofilms for short-term (10 days) catheterization, while the catheter lumen has more significant biofilms for long-term (about 30 days) catheterization. The liquid that is injected through a central venous catheter may affect the growth and formation of biofilms. For instance, Gram-negative strains such as Klebsiella spp. Enterobacter spp. and P. aeruginosa grow well and form biofilms in intravenous fluid, while Gram-positive bacterial strains such as S. aureus and S. epidermidis may not [30].
Prosthetic valve endocarditis is a condition caused by microbial biofilms. Microbes lead to this condition when they attach and form biofilms on the mechanical heart valves—some Gram-positive bacteria such as S. epidermidis, Bacillus spp., S. aureus, and Streptococcus spp., Gram-negative bacteria such as Enterococcus, and fungal species such as Candida spp. are known to cause prosthetic valve endocarditis. These microbes may arise from the skin or other medical implants including dental implants or central venous catheters [31]. Sometimes, fibrin and platelets may accumulate on the surface of medical implants because of tissue damage, for instance, during surgical implantation of the prosthetic heart valve. These are favorite places for microbes to grow and form biofilms [32].
After surgical procedures, urine excretion and generation are measured by using urinary catheters applied to the urinary bladder. This can be a closed or an open system. The open system is most commonly used to collect urine directly from the body and place it in an open collection center. This system has a higher chance of causing urinary tract infections (UTIs). On the other hand, in a closed system, urine is collected in plastic bags, which pose a lower chance of causing UTIs [33]. E. faecalis, P. aeruginosa, K. pneumoniae, E. coli, P. mirabilis and S. epidermidis are the common bacterial species found to cause UTIs [34].
4.2. Non-device-related Biofilm InfectionsBiofilms cause many types of infections in human beings (Table 1). Microbial biofilms damage the soft tissues of the teeth and the bone that supports the teeth, resulting in gum infection, a condition known as periodontitis. This condition may also result in tooth loss. Poor hygienic oral cavity is the main reason for this infection [35]. Periodontitis is mainly caused by Fusobacterium and P. aerobicus. In addition to tooth infection, these microbes may form biofilm-associated infections on mucosal surfaces [36]. They produce toxins, alter the flow of calcium in the epithelial layer, and damage mucosal cells upon tooth colonization. Dental plaque may result within three weeks due to microbial colonization and the mineralization of phosphate ions and calcium ions [37].
Similarly, Calhoun et al. [38] reported that bacterial and fungal species cause a bone disease known as osteomyelitis. In this disease, microbial cells use the bloodstream to enter into the bones. These microbes infect the metaphysis of bone after entering the bone via the bloodstream. This condition alerts the white blood cells (WBCs) which accumulate at the disease site. They start a process called phagocytose to lyse the pathogen. As a result of this process, WBCs release some enzymes. These enzymes also digest the bone cells, resulting in pus formation and spreading to other sites via blood vessels. The infection damages the bone cells and stops the normal flow of blood [39].
Table 1. Device-Related and Non-Device-Related Biofilms: Diseases, Pathogens, and Prevention
|
Category |
Diseases |
Common Species of Biofilm |
Factors/Prerequisites/Conditions of Biofilm Formation |
Prevention Options |
|---|---|---|---|---|
|
Device-Related |
Catheter-Associated Urinary Tract Infections (CAUTIs) |
Escherichia coli, Candida albicans, Pseudomonas spp. |
Surface material promoting adhesion, prolonged catheter usage, poor catheter maintenance, inadequate sterilization |
Use of antimicrobial or silver-coated catheters, regular catheter replacement, strict hand hygiene, and proper sterilization techniques |
|
|
Prosthetic Joint Infections |
Staphylococcus aureus, Staphylococcus epidermidis |
Introduction of bacteria during implantation surgery, contamination of prosthetic material, immune suppression |
Preoperative skin disinfection, use of antibiotic-impregnated prostheses, antibiotic prophylaxis, and sterile surgical protocols |
|
Ventilator-Associated Pneumonia (VAP) |
Acinetobacter baumannii, Klebsiella pneumoniae |
Prolonged mechanical ventilation, contaminated humidification systems, biofilm formation on tubing and connectors |
Regular cleaning and disinfection of ventilators, use of biofilm-resistant tubing, and limiting ventilation duration where possible |
|
|
Central Line-Associated Bloodstream Infections (CLABSIs) |
Candida spp., Enterococcus faecalis, Staphylococcus aureus |
Contamination during insertion, prolonged use of central lines, lack of sterile technique |
Use of chlorhexidine skin antiseptics, strict sterile insertion protocols, and regular line replacements |
|
|
Contact Lens-Associated Keratitis |
Pseudomonas aeruginosa, Staphylococcus aureus |
Poor lens hygiene, prolonged lens wear, inadequate cleaning solutions |
Regular lens cleaning, use of sterile solutions, and avoiding overnight lens use |
|
|
Non-Device-Related |
Periodontitis |
Porphyromonas gingivalis, Fusobacterium nucleatum |
Accumulation of dental plaque, poor oral hygiene, high consumption of dietary sugars, immune system evasion by biofilms |
Regular dental check-ups, proper brushing and flossing, use of antimicrobial mouthwash, and scaling and root planing treatments |
|
Osteomyelitis |
Staphylococcus aureus, Pseudomonas aeruginosa |
Trauma leading to bone exposure, contamination during surgery, hematogenous spread of bacteria |
Prompt surgical debridement, appropriate use of antibiotics, and management of any underlying medical conditions |
|
|
Chronic Sinusitis |
Staphylococcus aureus, Pseudomonas aeruginosa |
Blocked sinus drainage, recurrent infections, immune suppression |
Nasal irrigation, targeted antibiotics, and endoscopic sinus surgery if necessary |
|
|
Chronic Wound Infections |
Staphylococcus aureus, Pseudomonas aeruginosa |
Open wounds, poor hygiene, contamination, reduced local immunity |
Regular wound cleaning, use of wound dressings with antimicrobial properties, and early surgical debridement |
|
|
Otitis Externa (Swimmer’s Ear) |
Pseudomonas aeruginosa, Staphylococcus epidermidis |
Prolonged water exposure, damage to the ear canal lining |
Avoid prolonged water exposure, use of ear plugs, and topical antimicrobial drops |
5. POLYMICROBIAL BIOFILM INFECTIONS
Within an organism’s body, one microorganism may influence the colonization of other microorganisms. These microbes cause polymicrobial infections through their mutual interaction. For example, viruses destroy epithelial cells, suppress the immune system, and upregulate the secretion of compounds that are essential for bacterial adhesion to the surface. In this way, they promote bacterial infections in the respiratory tract. Similarly, microbial infections are also promoted by viruses in the middle ear which results in otitis media [40]. Scientist are showing more interest in studying microorganisms as a mixed community, rather than in isolation. Polymicrobial biofilms cause various infections including otitis media, oral infections, lung infections, urinary tract infections, diabetic foot infections, and infections in surgical wounds (Table 2) [41]. The most common dental infection is dental caries which affects upto 80% of adults and children. The microbes form a biofilm on tooth surface which works as a conditioning film and supports microbial attachment [42].
Table 2. Common Polymicrobial Infections and Microbes
|
Sr. No. |
Common Species |
Polymicrobial Infections |
References |
|---|---|---|---|
|
1 |
S. aureus, H. influenzae, Candida albicans, P. aeruginosa, Burkholderia cepacia complex, Viruss |
Lung infection (Cystic fibrosis) |
|
|
2 |
Prevotella sp., Mycoplasma spp., E. faecalis, Gardnerella vaginalis, Peptostreptococci, Ureaplasma urealyticum, Prevotella spp., Fusobacterium nucleatum |
Vaginosis |
|
|
3 |
H. influenzae, Streptococcus pneumoniae, Moraxella catarrhalis |
Otitis media |
[47] |
|
4 |
P. aeruginosa, S. aureus, K. pneumoniae, E. faecalis, C. albicans |
Medical device-associated infections |
[48] |
|
5 |
Proteus mirabilis, P. aeruginosa, E. faecalis, E. coli, K. pneumoniae |
Urinary tract infections |
[49] |
|
6 |
C. albicans, S. mutans |
Dental caries |
[50] |
|
7 |
Trichomonas vaginalis, U. urealyticum, E. coli, Chlamydia trachomatis, Mycoplasma hominis, Enterococci |
Prostatitis |
[51] |
|
8 |
Treponema denticola, Porphyromonas gingivalis, Tannerella forsythia |
Periodontitis |
[52] |
|
9 |
E. coli, Enterococcus spp., P. aeruginosa, Enterobacter spp., Klebsiella spp., S. aureus, Candida spp. |
Wound infections |
[53] |
Peters et al. [42] reported that otitis media affects the Eustachian tube of the middle ear. This disease rarely results in the death of the patient. More commonly, it results in hearing loss. Many bacterial species including M. catarrhalis, S. pneumoniae, and H. influenza in polymicrobial biofilm mode cause this infection with the help of a variety of viruses, such as Rhinovirus, influenza A virus, respiratory syncytial virus, and adenovirus.
Tay et al. [54] reported cystic fibrosis (CF) as another polymicrobial infection. This microbial infection is also an autosomal recessive disorder and may lead to respiratory failure. Patients suffering with CF lack muccilairy clearance which makes it dificult to remove the microbes trapped in the airways which results in polymicrobial infection. B. cepacia, S. aureus, H. influenzae, S. maltophilia, P. aeruginosa, C. albicans, and S. milleri are the microbial pathogens that cause CF.
5.1 Polymicrobial InteractionsThe three most common polymicrobial biofilms are bacterial-bacterial biofilms, fungal-fungal biofilms, and bacterial-fungal biofilms. The interaction among microorganisms plays a critical role in microbiome structure maintenance. Some of the interactions including pathogenic interactions are known as negative interactions, while beneficial interactions such as commensal or mutualistic interactions are called positive interactions. Advanced understanding of these microbial interactions has improved their application in pharmaceutical development, agriculture, environment management, and medical treatments [55]. Almost all the microbial cells were found to be attached with living or inert surfaces in polymicrobial biofilms. Various microbial groups including viruses, fungi, and bacteria coordinate to form polymicrobial biofilms. Exopolysaccharides (EPS), formed during biofilm development, cover the entire bacterial population [40]. Proteins, extracellular DNA, lipids, and exopolysaccharides comprise the exopolysaccharide matrix which plays an important role in determining the functional, structural, and virulence properties of biofilms [56].
6. ORGAN SYSTEM-RELATED BIOFILM INFECTIONS
Microbial biofilms have been reported to cause many organ system-level infections. These biofilm-associated infections are a serious challenge to medical procedures, since they are persistent and hard to eradicate with traditional antimicrobial therapies. The infection causing biofilms can develop on living tissues, as well as on medical implants and devices. Organ system-level infections include infections in respiratory, cardiovascular, urinary, and gastrointestinal organ systems. Biofilm prevention techniques with integrated medicine can help to cure biofilm-related infections.
6.1 Auditory SystemMicrobial biofilms cause inflammation in the middle-year cavity, resulting in otitis media (OM) (Figure 2 and Table 3). Preschool children are the main target of this infection. In developed countries, this is the primary reason for surgical procedures and antibiotic prescriptions for children [57]. OM can be categorized as acute otitis media (AOM), effusion otitis media (EOM), or chronic supportive otitis media (CSOM). These OM conditions may lead to temporary or permanent hearing loss [58].
Eustachian tube in children (under one year) and infants is the main target of these microbes. This tube is wider, horizontal, and shorter at this life stage, prone to pathogenic bacterial transmission from the nasopharynx to the middle ear cavity [58]. H. influenzae and S. pneumoniae are the two major microbial species that colonize the nasopharynx and increase the risk of AOM and OME [59]. Polymerase chain reaction (PCR) and reverse transcriptase polymerase chain reaction (RT-PCR) studies showed that the biofilms of pathogenic bacteria cause CSOM and OME [6]. Furthermore, confocal laser microscopical and scanning electron microscopical results also confirmed the presence of microbial biofilm in the ear cavity infected with OM [60]. AOM commonly targets children under the age of five years—nearly 40% of infected children have multiple episodes of AOM [61]. CSOM also targets children under the age of five years. Studies have reported the presence of biofilms (up to 42%) in the mastoid mucosa and in the middle ear (up to 92%) of the children affected with CSM [62].
Figure 2. Biofilm-associated Infections in Human Beings
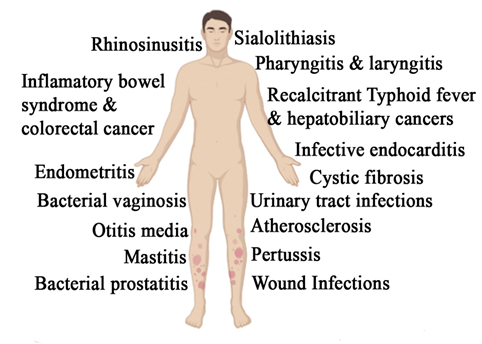
Microbial biofilms cause two types of cardiovascular infections, namely infective endocarditis (IE) and atherosclerosis (Figure 2 and Table 3). Infective endocarditis is the primary infection caused by a bacterial biofilm composed of host components of cardiac valve and bacterial cells. This biofilm contributes to disease development through several mechanisms: (1) it interferes with valve function by physically impairing closure, leading to leakage, and by disrupting smooth blood flow when the valve is open, causing turbulence and reduced efficiency; (2) it serves as a persistent source of bloodstream infection, challenging to eliminate with antibiotics; and (3) fragments of the biofilm may detach, travelling through the circulatory system and posing a significant risk of emboli, particularly in the brain, kidneys, and extremities. This kind of disease is challenging to treat with antibiotics; even though the microbes are sensitive to antibiotics, they still remain unaffected by them. Prolonged intravenous antibiotic treatment is required for this bacterial infection. Streptococci, staphylococci, and enterococci are the most prominent bacterial strains that cause about 80% of infective endocarditis [6, 63].
On the other hand, atherosclerosis is associated with plaque formation in the arterial wall. The plaque is composed of calcium and fat droplets. This narrows the artery's luman, thus reducing blood flow and can be life-threatening [64]. Meta-analysis of the plaque showed the presence of oral bacteria. However, whether bacteria initiate plaque formation or colonize the plaque after its formation remains unknown. Fluorescence in situ hybridization (FISH) and fluorescence microscopy studies revealed microbial biofilm in artery plaques [65].
6.3 Digestive SystemIn the digestive system, microbial biofilms have been reported to cause three primary infections: sialolithiasis, cancer, and typhoid fever, as well as colorectal cancer and inflammatory bowel disease (Figure 2 and Table 3).
Calcified masses form in the salivary gland, which results in sialolithiasis. The infected individual may feel pain and swelling. Studies have reported the presence of microbial biofilms at this site [66]. Morphological analysis using confocal laser scanning microscopy also showed the presence of bacterial biofilms in acute sialolithiasis [67]. Salmonella enterica causes a foodborne disease known as typhoid fever. In patients with typhoid fever, S. typhi's biofilm has been reported in the gall bladder [68]. The colon epithelium is covered by a protective mucosal layer, which separates it from the luminal bacterial community. Sometimes, pathogenic microbes breach this layer, access the epithelium, and start biofilm development. This condition results in inflammatory bowel disease (IBD) [69, 70].
6.4 Integumentary SystemBacterial biofilms cause various wound infections (Figure 2 and Table 3). Specifically, acute and chronic wounds are infected by pathogenic microbes. S. aureus, P. aeruginosa, and S. epidermidis are the most common bacterial strains that form biofilms and cause wound infections. Previously, it was a known fact that planktonic bacteria cause wound infections. However, recent findings have revealed that biofilms cause infections in chronic wounds [71]. Some studies have reported chronic wound infections as biofilm infections and attested the presence of microbial biofilms in acute wound infections [71, 72].
6.5 Reproductive SystemMicrobial biofilms cause many infections in the reproductive system, including bacterial vaginosis, chronic endometritis, and mastitis (Figure 2 and Table 3). One of the most common vaginal infections during reproductive years is bacterial vaginosis. This infection is usually associated with anaerobic bacterial strains such as Atopobium vagnae and Gardnerella vaginalis [73]. Chronic endometritis, as the name suggests, is a microbial infection related to the uterus. Various pathogenic bacterial strains, including some probiotic strains, have been found in the uterus. The most abundant are Lactobacillus, Prevptella, Sneathia, Gardnerella, and Atopobium [74]. In chronic endometritis, bacterial strains such as Proteus spp., E. coli, K. pneumonia, E. faecalis, Staphylococcus spp., P. aeruginosa, Streptococcus spp., and G. vaginalis reportedly colonize the endometrial mucosa. Various studies have reported the biofilms of these strains in endometrium, suggesting that these biofilms might be causing infections. The inflammation of mammary glands during lactation is called mastitis. Various bacterial strains have been reported to cause inflammation during lactation, such as E. coli, S. agalactiae, S. aureus, Klebsiella spp., S. uberis, Pseudomonas spp., and Enterobacter spp. These microbes colonize and form biofilms on the epithelial cells of mammary glands [75].
6.6 Respiratory SystemMicrobial biofilms also cause various infections in the respiratory system. Some diseases caused by these biofilms are chronic rhinosinusitis, pharyngitis, laryngitis, cystic fibrosis, and bordertella infections (Table 3). The inflammation of the paranasal sinuses and nose is called rhinosinusitis. The symptoms of this condition are nasal discharge, obstruction, and nasal blockage. It can be categorized both as acute, lasting up to 12 weeks, and chronic, persisting for more than 12 weeks. Bacterial biofilms such as S. aureus reportedly cause this condition [76]. Pharyngitis is a throat infection caused by many bacterial strains, such as Streptococcus spp., Haemophilus spp., and S. aureus. Transmission electron microscopy, scanning electron microscopy, and confocal microscopical studies have reported bacterial biofilm formation in the throat during pharyngitis [77, 78].
A highly contagious disease called pertussis/whooping cough is caused by Bordetella pertussis and Bordetella parapertussis. The biofilm of Bordertella has been reportedly causes whooping cough [79]. Cystic fibrosis is another infection caused by bacterial biofilms that affects the digestive and respiratory systems. The biofilms of S. aureus and H. influenzae reportedly cause this infection in the lungs, which may lead to death if matured to a chronic stage [80].
6.7 Urinary SystemSome urinary system infections, including chronic bacterial prostatitis and urinary tract infections or UTIs, are caused by microbial biofilms (Table 3). Bacterial prostatitis usually occurs with UTIs. The patient feels pain in the genital and pelvic region. During this infection, a person may face urosepsis, bladder infection, reduced fertility, prostatic abscesses, and even death [81]. If bacterial prostatitis lasts longer than 3 months, it is considered a chronic infection—many bacterial species including Klebsiella spp., E. coli, P. aeruginosa, E. faecalis, and P. mirabilis and their biofilms reportedly cause chronic bacterial prostatitis [82]. In this disease, microbe colonizes the bladder, kidneys, urethra, and ureters. The symptoms of this infection may vary depending on its anatomical location. In most cases, the patient feels urinary urgency, high frequency, dysuria, and pain. This infection is quicker to treat using antibiotics [83].
Table 4. Organ System-Related Biofilms: Diseases, Pathogens, and Prevention Strategies
|
System of Organs |
Diseases |
Common Species of Biofilm |
Factors/Prerequisites/Conditions of Biofilm Formation |
Prevention Options |
|---|---|---|---|---|
|
Respiratory |
Cystic Fibrosis |
Pseudomonas aeruginosa, Staphylococcus aureus |
Persistent thick mucus secretions, impaired mucociliary clearance, chronic airway inflammation |
Regular airway clearance techniques (e.g., chest physiotherapy), inhaled antibiotics, and use of mucolytics |
|
Tuberculosis |
Mycobacterium tuberculosis |
Prolonged exposure to infected individuals, immune suppression |
Vaccination (BCG), early diagnosis, and prolonged combination antibiotic therapy |
|
|
Cardiovascular |
Infective Endocarditis |
Streptococcus viridans, Staphylococcus aureus |
Damaged heart valves, presence of prosthetic valves, transient or persistent bacteremia |
Antibiotic prophylaxis prior to invasive dental or surgical procedures, early diagnosis and treatment of bacteremia |
|
Atherosclerosis |
Porphyromonas gingivalis, Helicobacter pylori |
Chronic inflammation, presence of circulating bacteria, immune system activation |
Controlling risk factors (e.g., cholesterol, blood pressure), and addressing chronic infections (e.g., periodontal disease) |
|
|
Urinary |
Recurrent Urinary Tract Infections |
Escherichia coli, Proteus mirabilis |
Urinary stasis due to obstruction or anatomical abnormalities, long-term catheter use |
Regular catheter changes, use of antimicrobial-coated catheters, hydration, and cranberry product supplementation |
|
Gastrointestinal |
Helicobacter pylori Gastritis |
Helicobacter pylori |
Colonization of gastric mucosa, acidic environment adaptation, immune evasion mechanisms |
Use of proton pump inhibitors, combination antibiotic therapy for eradication, and avoidance of NSAIDs |
|
Colitis |
Clostridium difficile |
Prolonged antibiotic use, gut microbiome disruption |
Judicious use of antibiotics, probiotics, and early diagnosis with fecal microbial transplant if necessary |
|
|
Auditory |
Chronic Otitis Media |
Haemophilus influenzae, Moraxella catarrhalis |
Eustachian tube dysfunction leading to fluid retention, recurrent infections, immune response suppression |
Tympanostomy tube placement, use of antibiotic ear drops, and regular ear examinations |
There are three main categories of microbial biofilm infections, namely device-related, non-device-related, and organ system-level infections. In device-level infections, microbial biofilms target medical implants including catheters, heart valves, and contact lenses. However, the development of biofilm on devices is determined by the type of device and the duration of implant. The non-device related infections include periodontitis and osteomyelitis, among others. In these infections, the biofilms often target the soft tissues. While, in organ system-level infections, the biofilms target the various parts of the system which leads to organ system-level disorders. The treatment of these biofilm-based infections often proves to be very complicated because of their resistance against traditional antimicrobial compounds. Control strategies should be adopted to encounter biofilm-related infections. The main aim of biofilm control strategies should be quorum sensing (QS) inhibition. In the absence of QS, biofilms do not form. For device-related infections, strategies to modify the surface and antimicrobial coating on the surface can be promising. While to control organ system-level infections, integrated approaches should be utilized, including combined use of antibiotics as biofilm disruptors and immunoregulators. Advanced techniques must be adopted to understand the stages of biofilm formation and their resistance mechanism to effectively reduce the burden of biofilm-associated infections.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Penesyan A, Paulsen IT, Kjelleberg S, Gillings MR. Three faces of biofilms: a microbial lifestyle, a nascent multicellular organism, and an incubator for diversity. NPJ Biofilms Microbiomes. 2021;7(1):80. https://doi.org/10.1038/s41522-021-00251-2
- Sharma S, Mohler J, Mahajan SD, Schwartz SA, Bruggemann L, Aalinkeel R. Microbial biofilm: a review on formation, infection, antibiotic resistance, control measures, and innovative treatment. Microorganisms. 2023;11(6):1614. https://doi.org/10.3390/microorganisms11061614
- Shineh G, Mobaraki M, Bappy MJP, Mills DK. Biofilm formation, and related impacts on healthcare, food processing and packaging, industrial manufacturing, marine industries, and sanitation–a review. Appl Microbiol. 2023;3(3):629–665. https://doi.org/10.3390/applmicrobiol3030044
- Shree P, Singh CK, Sodhi KK, Surya JN, Singh DK. Biofilms: understanding the structure and contribution towards bacterial resistance in antibiotics. Med Microecol. 2023;16:100084. https://doi.org/10.1016/j.medmic.2023.100084
- Mirzaei R, Mohammadzadeh R, Alikhani MY, Sholeh M, Moghadam MS, Karampoor S. The biofilm-associated bacterial infections unrelated to indwelling devices. IUBMB Life. 2020;72(7):1271–1285. https://doi.org/10.1002/iub.2266
- Vestby LK, Grønseth T, Simm R, Nesse LL. Bacterial biofilm and its role in the pathogenesis of disease. Antibiotics. 2020;9(2):59. https://doi.org/10.3390/antibiotics9020059
- Brinkman CL, Schmidt-Malan SM, Karau MJ, Greenwood-Quaintance KE, Hassaballa H, Mandrekar J, Patel R. Exposure of bacterial biofilms to electrical current leads to cell death mediated in part by reactive oxygen species. PLoS One. 2016;11(12):e0168595. https://doi.org/10.1371/journal.pone.0168595
- Liu X, Yao H, Zhao X, Ge C. Biofilm formation and control of foodborne pathogenic bacteria. Molecules. 2023;28(6):2432. https://doi.org/10.3390/molecules28062432
- Sauer K, Stoodley P, Goeres DM, Hall-Stoodley L, Burmølle M, Stewart PS, Bjarnsholt T. The biofilm life cycle: expanding the conceptual model of biofilm formation. Nat Rev Microbiol. 2022;20(10):608–620. https://doi.org/10.1038/s41579-022-00767-0
- Liaqat I, Muhammad N, Ara C, Hanif F, Zehra M, Shahid M. Bioremediation of heavy metals polluted environment and decolourization of black liquor using microbial biofilms. Mol Biol Rep. 2023;50(5):3985–3997. https://doi.org/10.1007/s11033-023-08334-3
- Abera GB, Trømborg E, Solli L, Haugen T, Berstad D. Biofilm application for anaerobic digestion: a systematic review and an industrial scale case. Biotechnol Biofuels Bioprod. 2024;17(1):145. https://doi.org/10.1186/s13068-024-02592-4
- Rasamiravaka T, Labtani Q, Duez P, El Jaziri M. The formation of biofilms by Pseudomonas aeruginosa: a review of the natural and synthetic compounds interfering with control mechanisms. Biomed Res Int. 2015;2015:759348. https://doi.org/10.1155/2015/759348
- Armbruster CR, Parsek MR. New insight into the early stages of biofilm formation. Proc Natl Acad Sci U S A. 2018;115(17):4317–4319. https://doi.org/10.1073/pnas.1804084115
- Rabin N, Zheng Y, Opoku-Temeng C, Du Y, Bonsu E, Sintim HO. Biofilm formation mechanisms and targets for developing antibiofilm agents. Future Med Chem. 2015;7(4):493–512. https://doi.org/10.4155/fmc.15.6
- Lu L, Zhao Y, Li M, Wang Y, Zhang J, Huang S. Contemporary strategies and approaches for characterizing composition and enhancing biofilm penetration targeting bacterial extracellular polymeric substances. J Pharm Anal. 2024;14(4):100906. https://doi.org/10.1016/j.jpha.2023.11.013
- Costerton W, Veeh R, Shirtliff M, Pasmore M, Post C, Ehrlich G. The application of biofilm science to the study and control of chronic bacterial infections. J Clin Invest. 2003;112(10):1466–1477. https://doi.org/10.1172/JCI20365
- Samrot AV, Mohamed AA, Faradjeva E, Si Jie L, Sze Chin H, Noel Vinay T. Mechanisms and impact of biofilms and targeting of biofilms using bioactive compounds–a review. Medicina. 2021;57(8):839. https://doi.org/10.3390/medicina57080839
- Zhao A, Sun J, Liu Y. Understanding bacterial biofilms: from definition to treatment strategies. Front Cell Infect Microbiol. 2023;13:1137947. https://doi.org/10.3389/fcimb.2023.1137947
- He Z, Liang J, Tang Z, Ma R, Peng H, Huang Z. Role of the luxS gene in initial biofilm formation by Streptococcus mutans. J Mol Microbiol Biotechnol. 2015;25(1):60–68. https://doi.org/10.1159/000371816
- Laganenka L, Sourjik V. Bacterial quorum sensing signals at the interdomain interface. Isr J Chem. 2023;63(5-6):e202200080. https://doi.org/10.1002/ijch.202200080
- Brackman G, Cos P, Maes L, Nelis HJ, Coenye T. Quorum sensing inhibitors increase the susceptibility of bacterial biofilms to antibiotics in vitro and in vivo. Antimicrob Agents Chemother. 2011;55(6):2655–2661. https://doi.org/10.1128/AAC.00045-11
- Ali A, Zahra A, Kamthan M, Husain FM, Albalawi T, Zubair MS. Microbial biofilms: applications, clinical consequences, and alternative therapies. Microorganisms. 2023;11(8):1934. https://doi.org/10.3390/microorganisms11081934
- Chambers HF, Bayer AS. Native-valve infective endocarditis. N Engl J Med. 2020;383(6):567–576. https://doi.org/10.1056/NEJMcp2000400
- Kaushik A, Kest H, Sood M, Steussy BW, Thieman C, Gupta S. Biofilm producing methicillin-resistant Staphylococcus aureus (MRSA) infections in humans: clinical implications and management. Pathogens. 2024;13(1):76. https://doi.org/10.3390/pathogens13010076
- Mirghani R, Saba T, Khaliq H, Mitchell J, Dunne C, Khan S. Biofilms: formation, drug resistance and alternatives to conventional approaches. AIMS Microbiol. 2022;8(3):239–277. https://doi.org/10.3934/microbiol.2022019
- Szczotka-Flynn LB, Pearlman E, Ghannoum M. Microbial contamination of contact lenses, lens care solutions, and their accessories: a literature review. Eye Contact Lens. 2010;36(2):116–129. https://doi.org/10.1097/ICL.0b013e3181d20cae
- Wu YT, Zhu H, Harmis NY, Iskandar SY, Willcox M, Stapleton F. Profile and frequency of microbial contamination of contact lens cases. Optom Vis Sci. 2010;87(3):E152–E158. https://doi.org/10.1097/OPX.0b013e3181cf86ee
- Ayush PT, Ko J-H, Oh H-S. Characteristics of initial attachment and biofilm formation of Pseudomonas aeruginosa on microplastic surfaces. Appl Sci. 2022;12(10):5245. https://doi.org/10.3390/app12105245
- Gominet M, Compain F, Beloin C, Lebeaux D. Central venous catheters and biofilms: where do we stand in 2017? APMIS. 2017;125(4):365–375. https://doi.org/10.1111/apm.12665
- de Sousa T, Hébraud M, Alves O, Costa P, Maltez L, Pereira JE, Machado I. Study of antimicrobial resistance, biofilm formation, and motility of Pseudomonas aeruginosa derived from urine samples. Microorganisms. 2023;11(5):1345. https://doi.org/10.3390/microorganisms11051345
- Galar A, Weil AA, Dudzinski DM, Muñoz P, Siedner MJ. Methicillin-resistant Staphylococcus aureus prosthetic valve endocarditis: pathophysiology, epidemiology, clinical presentation, diagnosis, and management. Clin Microbiol Rev. 2019;32(2):e00041-18. https://doi.org/10.1128/CMR.00041-18
- Su Y, Yrastorza JT, Matis M, Cusick A, Thompson S, Klapper I, Stewart PS. Biofilms: formation, research models, potential targets, and methods for prevention and treatment. Adv Sci. 2022;9(29):e2203291. https://doi.org/10.1002/advs.202203291
- Abdel-Aleem H, Aboelnasr MF, Jayousi TM, Habib FA. Indwelling bladder catheterisation as part of intraoperative and postoperative care for caesarean section. Cochrane Database Syst Rev. 2014;2014(4):CD010322. https://doi.org/10.1002/14651858.CD010322.pub2
- Yi-Te C, Shigemura K, Nishimoto K, Yamamichi F, Fujisawa M, Kitagawa K. Urinary tract infection pathogens and antimicrobial susceptibilities in Kobe, Japan and Taipei, Taiwan: an international analysis. J Int Med Res. 2020;48(2):0300060519867826. https://doi.org/10.1177/0300060519867826
- Lasserre JF, Brecx MC, Toma S. Oral microbes, biofilms and their role in periodontal and peri-implant diseases. Materials. 2018;11(10):1802. https://doi.org/10.3390/ma11101802
- Jamal M, Ahmad W, Andleeb S, Jalil F, Imran M, Nawaz MA, Hussain T. Bacterial biofilm and associated infections. J Chin Med Assoc. 2018;81(1):7–11. https://doi.org/10.1016/j.jcma.2017.07.012
- Rajasekaran JJ, Krishnamurthy HK, Bosco J, Jayaraman V, Krishna K, Wang Z, Arunachalam K. Oral microbiome: a review of its impact on oral and systemic health. Microorganisms. 2024;12(9):1797. https://doi.org/10.3390/microorganisms12091797
- Calhoun JH, Manring MM, Shirtliff M. Osteomyelitis of the long bones. Semin Plast Surg. 2009;23(2):59–72. https://doi.org/10.1055/s-0029-1214158
- Kumar V, Abbas AK, Aster JC. Robbins basic pathology. Philadelphia, PA: Elsevier Health Sciences; 2012. https://doi.org/10.1016/B978-1-4377-1781-5.00020-5
- Brogden KA, Guthmiller JM, Taylor CE. Human polymicrobial infections. Lancet. 2005;365(9455):253–255. https://doi.org/10.1016/S0140-6736(05)17745-9
- Maisetta G, Batoni G. Editorial: interspecies interactions: effects on virulence and antimicrobial susceptibility of bacterial and fungal pathogens. Front Microbiol. 2020;11:1922. https://doi.org/10.3389/fmicb.2020.01922
- Peters BM, Jabra-Rizk MA, O’May GA, Costerton JW, Shirtliff ME. Polymicrobial interactions: impact on pathogenesis and human disease. Clin Microbiol Rev. 2012;25(1):193–213. https://doi.org/10.1128/CMR.00013-11
- Limoli DH, Hoffman LR. Help, hinder, hide and harm: what can we learn from the interactions between Pseudomonas aeruginosa and Staphylococcus aureus during respiratory infections? Thorax. 2019;74(7):684–692. https://doi.org/10.1136/thoraxjnl-2018-212616
- Khanolkar RA, Clark ST, Wang PW, Wright GD, Guttman DS, Beiko RG. Ecological succession of polymicrobial communities in the cystic fibrosis airways. mSystems. 2020;5(6):e00809-20. https://doi.org/10.1128/mSystems.00809-20
- Javed A, Manzoor S. Comparative analysis of bacterial vaginosis microbiota among pregnant and non-pregnant females and isolation of phages against Enterococcus faecalis, Enterococcus faecium, and Shigella flexneri strains. Microb Pathog. 2020;149:104588. https://doi.org/10.1016/j.micpath.2020.104588
- Tomas M, Palmeira-de-Oliveira A, Simoes S, Martinez-de-Oliveira J, Palmeira-de-Oliveira R. Bacterial vaginosis: standard treatments and alternative strategies. Int J Pharm. 2020;587:119659. https://doi.org/10.1016/j.ijpharm.2020.119659
- Bair KL, Campagnari AA. Moraxella catarrhalis promotes stable polymicrobial biofilms with the major otopathogens. Front Microbiol. 2019;10:3006. https://doi.org/10.3389/fmicb.2019.03006
- Kaya E, Tollapi L, Pastore A, Bosetto A, Mozzo M, Merlini S, Berto S. Comparison of methods for the microbiological diagnosis of totally implantable venous access port-related infections. J Med Microbiol. 2020;69(11):1273–1284. https://doi.org/10.1099/jmm.0.001263
- Azevedo AS, Almeida C, Melo LF, Azevedo NF. Impact of polymicrobial biofilms in catheter-associated urinary tract infections. Crit Rev Microbiol. 2017;43(4):423–439. https://doi.org/10.1080/1040841X.2016.1240656
- Sridhar S, Suprabha BS, Shenoy R, Suman E, Rao A. Association of Streptococcus mutans, Candida albicans and oral health practices with activity status of caries lesions among 5-year-old children with early childhood caries. Oral Health Prev Dent. 2020;18:911–919. https://doi.org/10.3290/j.ohpd.a45411
- Škerk V, Schönwald S, Krhen I, Car V, Mareković I, Roglić S, Baršić B. Aetiology of chronic prostatitis. Int J Antimicrob Agents. 2002;19(6):471–474. https://doi.org/10.1016/S0924-8579(02)00087-0
- Dahlen G, Basic A, Bylund J. Importance of virulence factors for the persistence of oral bacteria in the inflamed gingival crevice and in the pathogenesis of periodontal disease. J Clin Med. 2019;8(9):1339. https://doi.org/10.3390/jcm8091339
- Serra R, Grande R, Butrico L, Montemurro R, de Franciscis S. Chronic wound infections: the role of Pseudomonas aeruginosa and Staphylococcus aureus. Expert Rev Anti Infect Ther. 2015;13(5):605–613. https://doi.org/10.1586/14787210.2015.1023291
- Tay WH, Chong KK, Kline KA. Polymicrobial–host interactions during infection. J Mol Biol. 2016;428(17):3355–3371. https://doi.org/10.1016/j.jmb.2016.05.006
- Pierce EC, Dutton RJ. Putting microbial interactions back into community contexts. Curr Opin Microbiol. 2022;65:56–63. https://doi.org/10.1016/j.mib.2021.10.008
- Karygianni L, Ren Z, Koo H, Thurnheer T. Biofilm matrixome: extracellular components in structured microbial communities. Trends Microbiol. 2020;28(8):668–681. https://doi.org/10.1016/j.tim.2020.03.016
- DeAntonio R, Yarzabal JP, Cruz JP, Schmidt JE, Kleijnen J. Epidemiology of otitis media in children from developing countries: a systematic review. Int J Pediatr Otorhinolaryngol. 2016;85:65–74. https://doi.org/10.1016/j.ijporl.2016.03.032
- Schilder AG, Chonmaitree T, Cripps AW, Rosenfeld RM, Casselbrant ML, Haggard MP, Venekamp RP. Otitis media. Nat Rev Dis Primers. 2016;2:16063. https://doi.org/10.1038/nrdp.2016.63
- Chonmaitree T, Trujillo R, Jennings K, Alvarez-Fernandez P, Patel JA, Loeffelholz MJ, Nokso-Koivisto J. Acute otitis media and other complications of viral respiratory infection. Pediatrics. 2016;137(4):e20153555. https://doi.org/10.1542/peds.2015-3555
- Donlan RM, Costerton JW. Biofilms: survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev. 2002;15(2):167–193. https://doi.org/10.1128/CMR.15.2.167-193.2002
- Jamal A, Alsabea A, Tarakmeh M, Safar A. Etiology, diagnosis, complications, and management of acute otitis media in children. Cureus. 2022;14(8):e28019. https://doi.org/10.7759/cureus.28019
- Khairkar M, Deshmukh P, Maity H, Deotale V. Chronic suppurative otitis media: a comprehensive review of epidemiology, pathogenesis, microbiology, and complications. Cureus. 2023;15(8):e43729. https://doi.org/10.7759/cureus.43729
- Elgharably H, Hussain ST, Shrestha NK, Blackstone EH, Pettersson GB. Current hypotheses in cardiac surgery: biofilm in infective endocarditis. Semin Thorac Cardiovasc Surg. 2016;28(1):56–59. https://doi.org/10.1053/j.semtcvs.2015.12.005
- Linton MF, Yancey PG, Davies SS, Jerome WG, Linton EF, Vickers KC. The role of lipids and lipoproteins in atherosclerosis. South Dartmouth, MA: Endotext; 2019. https://www.ncbi.nlm.nih.gov/books/NBK343489
- Snow DE, Everett J, Mayer G, Cox SB, Dinwiddie D, Beer J. The presence of biofilm structures in atherosclerotic plaques of arteries from legs amputated as a complication of diabetic foot ulcers. J Wound Care. 2016;25(Sup2):S16–S22. https://doi.org/10.12968/jowc.2016.25.Sup2.S16
- Schrøder SA, Eickhardt S, Bjarnsholt T, Nørgaard T, Homøe P. Morphological evidence of biofilm in chronic obstructive sialadenitis. J Laryngol Otol. 2018;132(7):611–614. https://doi.org/10.1017/S0022215118000646
- Kao WK, Chole RA, Ogden MA. Evidence of a microbial etiology for sialoliths. Laryngoscope. 2020;130(1):69–74. https://doi.org/10.1002/lary.27860
- Crawford RW, Rosales-Reyes R, Ramírez-Aguilar MD, Chapa-Azuela O, Alpuche-Aranda C, Gunn JS. Gallstones play a significant role in Salmonella spp. gallbladder colonization and carriage. Proc Natl Acad Sci U S A. 2010;107(9):4353–4358. https://doi.org/10.1073/pnas.1000862107
- Dejea CM, Sears CL. Do biofilms confer a pro-carcinogenic state? Gut Microbes. 2016;7(1):54–57. https://doi.org/10.1080/19490976.2015.1121363
- Li S, Konstantinov SR, Smits R, Peppelenbosch MP. Bacterial biofilms in colorectal cancer initiation and progression. Trends Mol Med. 2017;23(1):18–30. https://doi.org/10.1016/j.molmed.2016.11.004
- Diban F, Di Lodovico S, Di Fermo P, D’Ercole S, Dotta T, Cellini L, Petrini M. Biofilms in chronic wound infections: innovative antimicrobial approaches using the in vitro Lubbock chronic wound biofilm model. Int J Mol Sci. 2023;24(2):1004. https://doi.org/10.3390/ijms24021004
- James GA, Swogger E, Wolcott R, Pulcini ED, Secor P, Sestrich J, Costerton JW, Stewart PS. Biofilms in chronic wounds. Wound Repair Regen. 2008;16(1):37–44. https://doi.org/10.1111/j.1524-475X.2007.00321.x
- Jung H-S, Ehlers MM, Lombaard H, Redelinghuys MJ, Kock MM. Etiology of bacterial vaginosis and polymicrobial biofilm formation. Crit Rev Microbiol. 2017;43(6):651–667. https://doi.org/10.1080/1040841X.2017.1291579
- Moreno I, Codoñer FM, Vilella F, Valbuena D, Martinez-Blanch JF, Jimenez-Almazán J, Simon C. Evidence that the endometrial microbiota has an effect on implantation success or failure. Am J Obstet Gynecol. 2016;215(6):684–703. https://doi.org/10.1016/j.ajog.2016.09.075
- Douglas P. Re-thinking benign inflammation of the lactating breast: a mechanobiological model. Womens Health. 2022;18:17455065221075907. https://doi.org/10.1177/17455065221075907
- Tan NC, Foreman A, Jardeleza C, Douglas R, Vreugde S, Wormald PJ. Intracellular Staphylococcus aureus: the Trojan horse of recalcitrant chronic rhinosinusitis? Int Forum Allergy Rhinol. 2013;3(4):261–266. https://doi.org/10.1002/alr.21154
- Woo JH, Kim ST, Kang IG, Lee JH, Cha HE, Kim DY. Comparison of tonsillar biofilms between patients with recurrent tonsillitis and a control group. Acta Otolaryngol. 2012;132(10):1115–1120. https://doi.org/10.3109/00016489.2012.689859
- Roberts AL, Connolly KL, Kirse DJ, Evans AK, Poehling KA, Peters TR, Reid SD. Detection of group A Streptococcus in tonsils from pediatric patients reveals high rate of asymptomatic streptococcal carriage. BMC Pediatr. 2012;12:3. https://doi.org/10.1186/1471-2431-12-3
- Cattelan N, Dubey P, Arnal L, Yantorno OM, Deora R. Bordetella biofilms: a lifestyle leading to persistent infections. Pathog Dis. 2015;74(1):ftv108. https://doi.org/10.1093/femspd/ftv108
- Hector A, Frey N, Hartl D. Update on host–pathogen interactions in cystic fibrosis lung disease. Mol Cell Pediatr. 2016;3:12. https://doi.org/10.1186/s40348-016-0039-5
- Yoon BI, Han D-S, Ha US, Lee SJ, Kim HW, Kim SW, Cho YH. Clinical courses following acute bacterial prostatitis. Prostate Int. 2013;1(2):89–93. https://doi.org/10.12954/PI.12013
- Pendegast H, Leslie S, Rosario D. Chronic prostatitis and chronic pelvic pain syndrome in men. Treasure Island, FL: StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK557614
- Klein RD, Hultgren SJ. Urinary tract infections: microbial pathogenesis, host–pathogen interactions and new treatment strategies. Nat Rev Microbiol. 2020;18(4):211–226. https://doi.org/10.1038/s41579-020-0324-0