
| Review | Open Access |
|---|
Advances in Understanding Candida Species: Mechanisms of Antifungal Resistance and Emerging Therapies |

|
|---|
![]() Muhammad Taimur Khan1,2,
Muhammad Taimur Khan1,2,
![]() Zamarak Khan2,
Zamarak Khan2,
![]() Hajira Iqbal2,
Hajira Iqbal2,
![]() Syeda Mahnoor Bukhari2 ,
Syeda Mahnoor Bukhari2 ,
![]() Himmat Khan2,
Himmat Khan2,
![]() Sajjad Ahmad3,
Sajjad Ahmad3,
![]() Muhammad Salman4,
Muhammad Salman4,
![]() Abdullah4,5*
Abdullah4,5*
1Department of Pharmacy, Faculty of Chemical & Life Sciences, Abdul Wali Khan University Mardan, Pakistan
2School of International Education, Shandong Second Medical University, China
3Department of Clinical Medicine, Faculty of Veterinary Sciences, Lasbela University of Agriculture, Water and Marine Sciences, Uthal, Pakistan
4Department of Health and Biological Sciences, Abasyn University, Peshawar, Pakistan
5Bioscan Labs and Research Center, Dargai, Malakand, Pakistan
Background. The rising incidence of fungal infections and the growing threat of antifungal resistance have heightened the clinical importance of medical mycology. Candida species, particularly Candida albicans, are major contributors to fungal diseases, including vulvovaginal and oral candidiasis.
Methods. This mini review critically analyzed the current literature on Candida infection, primarily Candida albicans, growing antifungal resistance, and therapeutic limitations. Furthermore, this review also explored the emerging therapeutic strategies, including novel antifungal agents and nanotechnology-based strategies to overcome biofilm-related resistance.
Results. Recent studies highlight a rising prevalence of non-albicans Candida species (NAC), many of which exhibit increased antifungal resistance and a tendency for persistent infections. Nevertheless, Candida albicans remains a major pathogenic species, capable of evading the host immune response through robust biofilm formation and other virulence factors.
Conclusion. Infections caused by Candida species pose a significant healthcare challenge due to their rising incidence and increasing resistance to conventional antifungals. The complexity of the infection(s) is due to C.albicans accompanied by non-albicans species. This review emphasized on urgent need of emerging therapeutic strategies for biofilm-associated resistance.
Highlights
- The staggering rise of antifungal resistance due to Candida species () is an emerging problem in healthcare settings
- Due to limited therapeutic strategies, non-albicans are more contagious than Candida albicans spp.
- The albicans spp. promotes the formation of biofilm, contributes to antifungal resistance, and persistent infection
- To overcome the limitations of drug resistance, emerging molecular targeting therapies and nanotechnology are needed
- Host immune system plays a pivotal role in disease morbidity, severity, persistence, and response to therapy
GRAPHICAL ABSTRACT
1. INTRODUCTION
Invasive fungal infections (IFIs) are the cause of approximately 1.5 million deaths annually worldwide [1]. A significant proportion of these death tolls, including neonatal mortality are attributed to fungal sepsis, primarily acquired in hospitals, that is, opportunistic Candida infections [2]. Recent estimates suggest that IFIs affect over 6 million people worldwide, resulting in 3.8 million annual deaths [3]. In line with this, mucosal infections, particularly oral candidiasis, manifests in three primary forms: pseudomembranous, erythematous, and hyperplastic. Hyperplastic candidiasis is usually presented as a chronic lesion, while pseudomembranous and erythematous candidiasis are often acute in nature [4].
Additionally, a group of conditions known as "lesions associated with Candida spp.," such as Candida-associated denture stomatitis (CADS) as documented recently, are recognized in oral pathology [5]. Moreover, Vulvovaginal candidiasis (VVC), or Candida vaginitis, affects almost 70-75% of women during their lifetime, with about 10% experiencing recurrent VVC. Candida albicans is usually more recognized clinically compared to non-albicans species [6]. However, due to their nature, non albicans species (Candida parapsilosis, Candida. Tropicalis, Candida glabrata, Candida. krusei, and Candida. Dubliniensis) are increasingly implicated in nosocomial infections [7]. In addition, key risk factors of non-albicans candidiasis include age, prior antifungal use, diabetes and economic status. The pathogenic characteristics of non-albicans-related candidiasis are less explored but involve certain mechanisms including adhesion, epithelial invasion, enzyme secretion, and immune evasion [8]. Similarly, Candida albicans commonly colonizes the human gut and is generally considered normal. However, its presence has been associated with intestinal issues, such as Crohn's disease [9]. Patients often exhibit heightened antibodies against C. albicans, which is frequently found in their stools [10]. Certain genetic variations affect immune reactions to commensal fungi. C. albicans colonization delays recovery in ulcerative colitis but antifungal therapy and probiotics have demonstrated promising effects [11]
Despite its role in disseminated candidiasis, gut colonization via C. albicans may offer protective benefits, such as resistance against Clostridioides difficile infection and enhanced immune responses against various pathogens. Gastrointestinal colonization induces antifungal immune responses, protecting against C. albicans or Candida auris infections, and possibly against other pathogens, emphasizing the potential benefits of C. albicans gut colonization [12]. Particularly, the C. albicans antigens (Hyr1), potentially provides cross-kingdom protection against Ancinetobacter baumanii infection, facilitating gut colonization of albicans in immunocompromised patients [13].
Moreover, candidiasis includes mucosal and invasive candidiasis (IC). These kinds of candida infections include organ-related infections and candidemia, respectively. The IC is mainly caused by C. albicans and some other species, such as C. tropicalis, C. auris, and some other non-albicans species. The IC causes blood-associated candidiasis, such as deep vein thrombosis. On the other hand, the associated risk factors include critical illness, over-use of broad-spectrum antibiotics, immunosuppression, and skin disruption [14]. Therefore, this study examined the escalating challenge particularly Candida albicans, focusing on their growing antifungal resistance and clinical significance across various infections. In addition, emerging therapeutic strategies were also discussed to overcome resistance and improve treatment efficacy.
2. ETIOLOGY AND EPIDEMIOLOGY
Candidiasis is an opportunistic infection mainly caused by Candida spp., particularly C. albicans and non-albicans are involved including C. tropicalis, C. krusei, and others, typically in recurrent resistant cases. The infection is particularly associated with C. albicans which colonizes in oral, esophageal, and Gastrointestinal (GI) tracts of healthy individuals. However, in immunocompromised patients, such as those with leukemia or lymphoma who are receiving corticosteroid or cytotoxic drug therapies, Candida may cause proliferation, leading towards mucosal candidiasis [15].
In line with this, 90% of HIV patients are affected with oral candidiasis as opportunistic infection. Notably, esophageal candidiasis is more prevalent in individuals suffering from HIV/AIDS with low CD4+ counts [16, 17].
Subsequently, the use of broad-spectrum antibiotics is a risk factor of candidiasis in cancer patients receiving cytotoxic chemotherapy. They are at risk of mycosis due to fungal translocation through damaged mucosal barriers (as shown in Fig 1) [18]. In accordance with this, mutation in the endogenous population or host surrounding may lead to pathogenic symbiosis with GI tract [19]. Vaginal candidiasis is commonly an occurring infection in patients with diabetes mellitus, pregnant women, and in those using oral contraceptives [20] (shown in Fig. 2). Additional risk factors for candidiasis include tuberculosis, myxedema, hypoparathyroidism, Addison's disease, nutritional deficiencies (such as vitamin A, B6, and iron), smoking, poorly-maintained dentures, the use of intravenous tubes and catheters, heart valve issues, old age, infancy, pregnancy, and xerostomia. These tend to reduce the presence of protective antifungal proteins, such as histatin and calprotectin [21].

Figure 1. Etiology and Risk Factors for Candidiasis
This flowchart illustrates important factors contributing to the risk of developing candidiasis. Notable influences include antibiotic use, immunocompromised states (e.g., cancer, HIV), and underlying conditions, such as diabetes and age-related changes. These factors have the potential to significantly affect the frequency of Candida infections in susceptible populations.
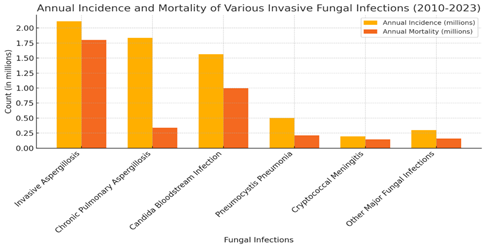
Figure 2. Global Impact of Invasive Fungal Infections (2010-2023).
This figure demonstrates annual incidence and significant mortality rate of various fungal infections [22].
3. CLINICAL MANIFESTATIONS
>3.1. Nosocomial Candidiasis and Antifungal ResistanceNosocomial candidiasis is a major cause of morbidity and high mortality (71%), particularly candidemia in hospital settings. Studies have reported C. albicans as the most predominantly isolated species in hospital-acquired infections. However, non-albicans species are also increasingly documented with unpredictable resistance patterns and antifungal agents [23, 24]. In addition, non-albicans species including C. parapsilosis, C. glabrata, and C.krusei have shown resistance to antifungal drugs (azole) as compared to C. albicans [25]. Similarly, factors affecting blood culture persistence in candidemia include host traits, antifungal resistance, treatment efficacy, and source control. Furthermore, risk factors for persistent candidemia include contiguous infections, central lines futile treatment, prolonged hospitalization, and septic shocks [26]. Global outbreaks of resistant Candida strains (as shown in figure 2 &3) highlight the need for infection control. Antifungal resistance is notably higher in non-albicans species, particularly C. parapsilosis. Additionally, C. albicans biofilm formation significantly boosts resistance against antifungal treatment [27]. However, significant research gaps still exist in understanding clinical outcomes between Candida species with and without resistance. In line with this, previous studies investigated critical and moderate COVID-19 patients with candidemia.
3.2. Oral CandidiasisThe current research evidently reported C. albicans as an opportunistic pathogen for the progression and development of Oral Squamous Cell Carcinoma (OSCC). This type of cancer promotes mutation in cell structure and cariogenic substances [28]. Similarly, malignant disorders (OPMDs), particularly oral leukoplakia, is significantly associated with the highest frequency of C. albicans [29]. However, the classification of Chronic Hyperplastic Candidiasis (CHC) as an OPMD remains controversial. Whereas, some classifications include CHC due to its high malignant transformation rate, while others exclude it. Recent meta-analyses indicate a notable malignant transformation rate for CHC patients. Furthermore, association between C. albicans and OSCC underscores its potential role in disease progression [30]. Epidemiological studies have revealed the association between C. albicans and OSCC development, with high detection rates observed in saliva of OSCC patients. Moreover, stability in C. albicans colonization after various OSCC treatments implies its persistence in disease progression [31]. Animal models have further verified the carcinogenic potential of C. albicans, demonstrating its ability to promote oral epithelial dysplasia transformation into OSCC. These experiments reveal C. albicans as a significant risk factor for oral mucosal carcinogenesis [32].
Similarly, DS, a commonly occurring candidiasis is more prevalent in denture users [32]. Despite its multifaceted origins, the primary cause of DS is the formation of Candida albicans biofilm on oral and denture surfaces. DS affects 17-75% of denture wearers, with a higher incidence in elderly females, commonly observed on mucosal denture surfaces and the posterior tongue. DS manifests as erythema, mucosal swelling, and edema. Management typically involves oral and denture hygiene measures, denture adjustments, smoking cessation, and antifungal medications as shown in Figure 1. Alternative therapies, such as microwave disinfection and photodynamic therapy are under investigation but require further validation for routine clinical use. General dental practitioners play a pivotal role in effectively managing DS by understanding its pathogenesis, recognizing clinical presentations, and employing contemporary treatment approaches [33].
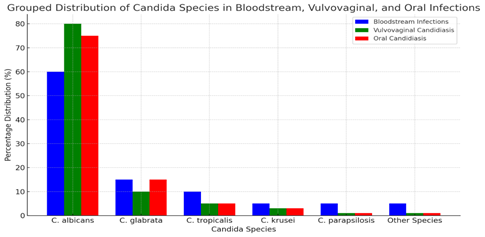
Figure 3. Distribution of Candida Species in Bloodstream, Vulvovaginal, and Oral Infections.
This chart illustrates the prevalence of various Candida species across different types of infections. C. albicans remains predominant in bloodstream infections, whereas non-albicans are more prevalent in vaginal and oral candidiasis [34].
3.3. Vulvovaginal Candidiasis (VVC)VVC is the fungal infection of vulva and vagina, primarily caused by fungal infections, such as Candida species, with Candida albicans being the most common species. VVC is affecting millions of women and is considered as the second-most common cause of vaginitis as compared to bacterial vaginosis [35]. Studies have revealed over one million of VVC cases among women of United states, and 53% of cases reported have often been treated with antifungal agents [36]. Likewise, non-albicans species including Candida glabrata, Candida tropicalis, Candida krusei, and Candida parapsilosis can also cause VVC. However, these species are often significantly associated with higher more recurrent rates and greater antifungal resistance compared to C. albicans [37]. Several risk factors contribute to VVC development including gene polymorphisms, allergies, antibiotics, diabetes, hypertension, estrogen levels, and multi-partners [38]. Clinically, VVC is divided into two main types, that is, uncomplicated cases, which are usually mild and sporadic and complicated cases, which can be severe or recurrent [39]. Fluconazole is the primary treatment for VVC, however, studies have claimed that about 63% of women may have ongoing infections after treatment [39].
Table 1. Major Clinical Forms of Candidiasis: Invasive, Nosocomial, Oral, Vulvovaginal, Gastrointestinal, and Chronic Hyperplastic Candidiasis (CHC)
|
Type of Candidiasis |
Clinical Features |
Associated Species |
Key Risk Factors |
References |
|---|---|---|---|---|
|
Invasive Candidiasis (IC) |
Bloodstream infection and deep-seated infection. Mortality: 50-71%. |
C. albicans, C. tropicalis, C. glabrata, C. parapsilosis, C. auris. |
Immunosuppression, broad-spectrum antibiotics, ICU stays, catheters, critical illness. |
|
|
Nosocomial Candidiasis |
Hospital-acquired candidemia; persistent infections due to biofilm formation on medical devices. |
Non-albicans species (e.g., C. parapsilosis complex), C. albicans. |
Central venous catheters, prolonged hospitalization, severe sepsis. |
|
|
Oral Candidiasis |
Subtypes: - Pseudomembranous (white plaques). - Erythematous (red patches). - Hyperplastic (chronic lesions). - Denture stomatitis (CADS) (erythema under dentures). |
Predominantly C. albicans; non-albicans in immunocompromised patients. |
HIV/AIDS, diabetes, denture use, smoking, xerostomia. |
|
|
Vulvovaginal Candidiasis (VVC) |
Vaginal itching, discharge, erythema; recurrent cases (≥4 episodes/year). |
C. albicans (85-95%); non-albicans (C. glabrata, C. africana, C. dubliniensis). |
Diabetes, estrogen therapy, antibiotic use, genetic polymorphisms. |
|
|
Gastrointestinal Candidiasis |
Asymptomatic colonization or dysbiosis linked to Crohn’s disease; potential protection against C. difficile |
C. albicans (commensal/pathogenic switch). |
Antibiotic use, immunosuppression, altered microbiota. |
|
|
Chronic Hyperplastic Candidiasis (CHC) |
Pre-malignant oral lesions; controversial association with oral squamous cell carcinoma (OSCC). |
C. albicans (hyphal form promotes epithelial dysplasia). |
Tobacco use, chronic mucosal irritation. |
The gut microbiome comprises various fungal species as normal flora which can be harmful to human health, sometimes acting as opportunistic pathogens. An imbalance of these fungal communities, known as dysbiosis, is directly linked with inflammation and some autoimmune disorders [62]. Despite the fact that C. albicans frequently engages in asymptomatic interactions with its host, it remains a standard constituent of the human gut microbiota. Colonization typically occurs in childhood and the fungal clones that establish infection are believed to persist in a quiescent state throughout the life of an individual [63]. To prevent these commensal fungi from turning pathogenic, the immune system plays a crucial role through complex interactions. Recent research has made considerable contributions in identifying the innate and adaptive immune pathways that regulate intestinal fungi [57]. These studies have advanced our understanding of fungal molecular pathways, revealing how these fungi can either remain benign or become pathogenic in the gut environment.
Additionally, C. albicans are commonly occurring species in GI tract, coexisting with diverse bacterial species and establishing commensal and pathogenic behavior [58]. Mouse models have shown that microbiota composition is key for successful colonization, with some bacterial consortia inhibiting C. albicans [64]. While C. albicans is not a representative colonizer in many mouse strains, certain strains, such as those treated with antibiotics, can be easily colonized. By altering metabolic pathways, fungal growth can be affected, resulting in colonization resistance and boosting the immune response to produce antimicrobial peptides, such as LL-37. Specific diets, however, may promote colonization [65].
Additionally, in human beings, the microbiome plays a crucial role in controlling C. albicans levels, with broad-spectrum antibiotics being a major risk factor for candidemia [66]. Patients undergoing hematopoietic stem-cell transplants or ICU treatments with antibiotics (targeting anaerobes) show increased Candida species in their intestinal mycobiome [67]. These findings underscore the role of microbiota in suppressing C. albicans overgrowth and pathogenicity in both experimental models and patients. Conversely, C. albicans colonization may affect the intestinal micro and mycobiome, promoting bacterial dysbiosis and invasive infection.
Furthermore, laboratory studies have revealed that bacteria may antagonize C. albicans growth and pathogenicity. Probiotic cocktails reduce polymicrobial biofilm formation and bacterial metabolites, such as fatty acids inhibit fungal hyphal formation [59]. Similarly, Lactobacillus rhamnosus can prevent the colonies of C. albicans from disrupting intestinal barriers [68]. Previously, study has also investigated the role of host epithelial cells to C. albicans resistance but due to various invading mechanisms, these pathogens easily translocate via epithelial cells barriers [69].
albicans is found to colonize the GI tract by utilizing available nutrients effectively, showing notable nutritional flexibility. It can use various carbon sources simultaneously and achieve adaptation to the low-glucose environment of the distal GI tract [59]. Nutritional adaptation includes tight regulation of nutrient acquisition pathways, with N-acetyl glucosamine (GlcNAc) playing a significant regulatory role. Different nutrient sources impact C. albicans' stress resistance and colonization ability, with specific mutants showing susceptibility to stresses and reduced colonization capability [70].
The C. albicans also possesses the ability to familiarize with diverse conditions, for instance the availability of carbon source and iron intake effects the colonization and pathogenicity. For instance, modification in cell wall structure can significantly influence immune activation or envision [71]. Consequently, the alteration of GI tract metabolites milieu by producing prostaglandin E2 (PGE2), derived from arachidonic acid which plays a crucial role in colonization of C. albicans [60].
For instance, bile acids also significantly affect C. albicans behavior, influencing colonization and infection. Secondary bile acids have antifungal properties, while primary bile acids can promote fungal growth and filamentation. However, antibiotic treatment disrupts bile acid conversion, increasing primary bile acids and enhancing C. albicans outgrowth [72].
Furthermore, C. albicans must adapt to gut-specific conditions, such as hypoxia and varied pH levels, requiring sophisticated regulatory networks. Phenotypic adaptation includes the ability to switch between yeast and hyphal forms, essential for invasive disease but detrimental for commensalism. The intestinal environment suppresses filamentation, supporting commensalism by limiting hyphal growth [73].
Additionally, C. albicans forms specialized gut cells during colonization. These cells have maximized ability of adherence to GI linings, increased susceptibility to bile associated acids, and alteration in metabolism, contributing in prolonged colonization [61].
4. DIAGNOSIS
4.1. Biomarkers of Candida SpeciesVarious diagnostic techniques and non-culture-based methods, such as serological biomarkers (CAGTA test, BDG, Mannan-Ag, and Mannan-Ab), are available for sensitive and rapid diagnosis of invasive candidiasis. Techniques include the detection of Candida DNA and circulating fungal antigens in serum. Commercial tests exist for BDG, Mannan-Ag, and Cand-TecTM Candida-antigen (CA), though nucleic acid amplification techniques still require standardization [74]. Reported sensitivity/specificity for these techniques vary, with BDG at 77%/85%, Mannan-Ag at 58%/93%, and CA at 64%/58% [75]. Despite this, BDG and Mannan-Ag have proved to be effective serum biomarkers depending on the diagnostic approach. However, ELISA can increase the sensitivity of Mannan-Ag and Mannan-Ab measurements to 83% and 86%, respectively [76]. Additionally, high BDG levels in bacteremia challenge its validity to diagnose invasive fungal disease [77]. Furthermore, antibodies against glucans (ALCA) and chitin (ACCA) have also been explored as potential biomarkers [78].
Table 2. Summary of Diagnostic Techniques and Biomarkers for Invasive Candida Infections
|
Diagnostics |
Details |
|---|---|
|
Urgent Medical Need |
Improved diagnostic tools for early detection of invasive Candida infections and monitoring antifungal therapy. |
|
Diagnostic Techniques |
Non-culture-based methods: CAGTA test, BDG, Mannan-Ag, Mannan-Ab. <br>- Detection of Candida DNA and circulating fungal antigens in serum. |
|
Commercial Tests |
BDG, Mannan-Ag, Cand-TecTM Candida-antigen (CA). |
|
Sensitivity/Specificity |
BDG: 77%/85% <br>- Mannan-Ag: 58%/93% <br>- CA: 64%/58%. |
|
Effectiveness of Biomarkers |
BDG and Mannan-Ag show promise based on diagnostic approach. <br>- ELISA increases sensitivity: Mannan-Ag (83%), Mannan-Ab (86%). <br>- High BDG in bacteremia challenges its diagnostic validity. |
|
Other Biomarkers |
Antibodies against glucans (ALCA) and chitin (ACCA) explored as potential biomarkers. |
|
CAGTA Test and BDG |
High sensitivity and NPV in ICU patients with severe abdominal conditions; reduces unnecessary antifungal therapy in 31% of patients. |
|
Combination of Biomarkers |
CAGTA + BDG or Mannan-Ag: Very high NPV. <br>- Useful in antifungal control programs to limit unnecessary empirical therapy in suspected candidemia cases. |
|
Challenges |
Limited data on biomarkers for deep-seated candidiasis with negative blood cultures. <br>- Interpretation difficulties, potential false positives/negatives. |
|
Promising Detection Tool |
Bispecific monoclonal antibody combining mAbs against BDG and MP65 for detecting significant Candida biomarkers in patient sera. |
The CAGTA test and BDG, used serially during empirical antifungal treatment, show high sensitivity and negative predictive value (NPV) in ICU patients with severe abdominal conditions. This method could reduce unnecessary antifungal therapy in at least 31% of patients, supporting antifungal control programs. Combining CAGTA with BDG or Mannan-Ag yields a very high NPV and may help limit unnecessary empirical therapy in suspected candidemia cases. Furthermore, data on biomarkers in patients with deep tissue candidiasis and negative blood cultures is rare, leading to challenges in interpretation and potential false positives or negatives. A bispecific monoclonal antibody, combining mAbs against BDG and MP65, shows promising results as a tool for the detection of clinically-significant Candida biomarkers in patient sera [79].
5. THERAPEUTIC ADVANCEMENTS
5.1. Pathogenesis Associated with Biofilm Formation: Future Recommendations and Therapeutic AdvancementsThe challenge of the high mortality and morbidity rate caused by C. albicans biofilm formation is a critical issue. As the problem of biofilm and biomaterial infections continues to escalate, it becomes imperative to develop new antifungal agents and identify new targets [80]. According to studies, the formation of biofilm and pathogenesis of C. abicans could be an exploring point for therapeutic strategies and drug resistance [81].
Recent advancements have highlighted different transcription factors including quorum sensing molecules, host response to adhesion, changes in efflux pumps, enzymes, bud to hyphal transition, and aberration in lipid profiles that lead to biofilm resistance [82]. Additionally, researchers are actively exploring the development of anti-adhesive biomaterials, anti-infective lock therapies, and high throughput screening methods to discover small-molecule inhibitors derived from natural compounds [83]. In terms of medical instruments' prevention measures against bacterial accumulation and biofilm formation, coating them with nanomaterial has shown promising results [84]. Conversely, metal nanoparticles are also considered as potential agents to inhibit biofilm formation in C. albicans [85].
Extensive studies should be conducted to understand different phenotypic character changes involved in biofilm formation. To enhance our knowledge further, electron microscopic techniques, such as TEM (Transmission Electron Microscopy) and SEM (Scanning Electron Micro) can be utilized at higher resolutions, providing detailed insights into the structure of these complex structures [86]. Another approach is using engineered enzymes that inhibit colony formation thus, preventing subsequent biofilm growth effectively [87].
In its host environment, C. albicans utilizes various secreted effectors, including candidalysin and nutrient acquisition machinery, for survival. Recent findings have revealed that macrophages possess the ability to detect these fungal effectors. A specific cysteine-rich protein, resembling effectors of plant pathogens, has been observed to activate macrophages through Toll-like receptor (TLR)-2 and 4 signaling [88]. Additionally, candidalysin, a hypha-associated toxin, has been implicated in macrophage activation. The release of IL-1β plays a crucial role in host defense against C. albicans, facilitating neutrophil recruitment to vital sites, such as the brain [88]. Candidalysin is identified as a mediator of NLRP3-inflammasome activation, essential for processing pro-IL-1β in macrophages [89]. These discoveries underscore the dual role of fungal effectors, serving as virulence factors for the fungus while also being recognized by macrophages, leading to neutralization of its virulence. In healthy individuals, macrophages exhibit optimal functionality. However, in patients with systemic candidiasis, macrophage function can be severely compromised due to underlying conditions, intense inflammation, and immunosuppressive therapy. Immunotherapy presents a promising avenue to bolster host defense and combat fungal infections, as discussed by Armstrong-James et al. Interferon-γ (IFN-γ) stimulation has emerged as a particularly intriguing approach, as it enhances phagocytosis and killing by macrophages [90]. Murine models have shown that depletion of NK cells and the consequent reduction in IFN-γ levels impairs macrophage-mediated clearance of C. albicans [91]. Additionally, intravenous immunoglobulin therapy has shown promising results in providing protection against Candida auris and Candida albicans in mouse models, especially in combination with antifungal drugs, such as amphotericin B [92]. Consequently, IFN-γ presents an attractive strategy to enhance macrophage function in order to eliminate C. albicans. However, the precise molecular mechanisms underlying the enhanced clearance of C. albicans by macrophages following IFN-γ treatment remain to be fully elucidated. Conversely, an excess of IL-1β-mediated inflammation can exacerbate immunopathology. Immunotherapy aimed at modulating this proinflammatory signal holds promising results to enhance infection outcomes. To mitigate immunopathological effects resulting from candidalysin-induced NLRP3-inflammasome activation, sulfonylureases have been proposed as a potential suppressive agent [93]. Despite their perceived efficacy, macrophages often fail to overcome candidiasis in severely-compromised patients. Recent studies emphasize the significant adaptability of C. albicans within macrophages, highlighting its ability to evade immune responses. In the early stages of infection, the fungus detect environmental and primes itself for interactions with phagocytes, a trait that highlights its evolutionary adaptation as commensal-turned pathogen [94].
Table 3. Advance Therapeutic Strategies to Overcome C. albicans Biofilm Resistance
|
Therapeutic Strategy |
Description |
References |
|---|---|---|
|
Targeting Transcription Factors and Quorum Sensing |
Investigating roles of transcription factors (e.g., biofilm regulators) and quorum sensing molecules (e.g., farnesol) to disrupt biofilm resistance. |
[82] |
|
Host Response to Adhesion |
Developing anti-adhesive biomaterials (e.g., nanomaterial coatings) to prevent fungal adhesion to medical devices. |
[83] |
|
Efflux Pumps and Enzymes |
Exploring inhibitors of efflux pumps (e.g., ABC transporters) and enzymes (e.g., hydrolases) to reduce antifungal resistance. |
[87] |
|
Bud-to-Hyphal Transition |
Targeting hyphal formation (critical for biofilm virulence) using small-molecule inhibitors or genetic modulation. |
[82] |
|
Lipid Profile Alterations |
Disrupting lipid-mediated biofilm robustness through lipidomic studies and antifungal agents. |
[82] |
|
Anti-Infective Lock Therapies |
Using lock therapies (e.g., antifungal-infused solutions) to prevent biofilm formation on catheters. |
[83] |
|
High-Throughput Screening |
Identifying novel antifungal compounds (natural/synthetic) via high-throughput methods. |
[84] |
|
Nanotechnology-Based Approaches |
Applying nanoparticles (e.g., metal NPs, carbon nanotubes) to disrupt biofilms or enhance drug delivery. |
[85] |
|
IFN-γ Immunotherapy |
Enhancing macrophage phagocytosis and fungal clearance via IFN-γ stimulation. |
[93] |
|
NLRP3-Inflammasome Modulation |
Suppressing excessive IL-1β-mediated immunopathology using sulfonylureases. |
[93] |
|
Probiotics and Engineered Enzymes |
Lactobacillus rhamnosus GG releases Chitinase (Msp1) enzyme Degrades chitin in Candida albicans hyphal cell walls, inhibiting morphogenesis and biofilm formation. Saccharomyces boulardii CNCM I-745 produces Capric acid (Decanoic acid) which Inhibits C. albicans hyphal morphogenesis and biofilm formation. |
6. CONCLUSION
In conclusion, the rising global incidence of candidiasis, driven by increasing antifungal resistance, and emergence of resilient non-albicans species, highlights an urgent need for state of the art diagnostic and treatment strategies. Candida species particularly C. albicans remain a challenging pathogen owing to its dual nature as commensal and opportunistic invasive species, capable of evading host immune system by biofilm formation, phenotypic plasticity, and immunoregulation. The therapeutic landscape is further challenged by emerging resistance of non-albicans (C. glabrata, C. parapsilosis, and C. auris) to traditional antifungals, demanding a transformative shift in management approaches. Additionally, emerging therapies such as immunotherapy targeting macrophage function, quorum sensing inhibitors and nanotechnology based drug delivery significantly overcoming biofilm associated resistance. Moreover, engineered enzymes and probiotics underscore the potential of microbiome-based intervention to disturb C. albicans virulence. Therefore, further studies are required to address challenges particularly in immunocompromised patients where host-pathogen interaction are deregulated. .
AUTHOR CONTRIBUTION
Muhammad Taimur Khan: conceptualization. Zamarak Khan: writing – review & editing. Hajira Iqbal: conceptualization. Syeda Mahnoor Bukhari: writing – review & editing. Himmat Khan: conceptualization. Sajjad Ahmad: conceptualization. Muhammad Salman: writing – review & editing. Abdullah: writing – review & editing.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
Data supporting the findings of this study will be made available by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
GENERATIVE AI DISCLOSURE STATEMENT
The authors did not used any type of generative artificial intelligence software for this research.
REFERENCES
- Bajpai VK, Khan I, Shukla S, et al. Invasive fungal infections and their epidemiology: measures in the clinical scenario. Biotechnol Biopro Eng. 2019;24:436–444. https://doi.org/ 10.1007/s12257-018-0477-0
- Chavez-Bueno S, McCulloh RJ. Current trends in epidemiology and antimicrobial resistance in neonatal sepsis. In: Vincent J-L, ed. Annual Update in Intensive Care and Emergency Medicine 2018. Springer Nature; 2018:39–51.
- Pinho S, Miranda IM, Costa-de-Oliveira S. Global epidemiology of invasive infections by uncommon candida species: a systematic review. J Fungi. 2024;10(8):e558. https://doi.org/10.3390/jof10080558
- Vila T, Sultan AS, Montelongo-Jauregui D, Jabra-Rizk MA. Oral candidiasis: a disease of opportunity. J Fungi. 2020;6(1):e15. https://doi.org /10.3390/jof6010015
- Firoozi P, Farshidfar N, Fekrazad R. Efficacy of antimicrobial photodynamic therapy compared to nystatin therapy in reducing Candida colony count in patients with Candida-associated denture stomatitis: a systematic review and meta-analysis. Evid Based Dent. 2021:1–8. https://doi.org/10.1038/s41432-021-0208-9
- Nsenga L, Bongomin F. Recurrent candida vulvovaginitis. Venereology. 2022;1(1):114–123. https://doi.org/ 10.3390/venereology1010008
- Xiao M, Fan X, Chen SCA, et al. Antifungal susceptibilities of Candida glabrata species complex, Candida krusei, Candida parapsilosis species complex and Candida tropicalis causing invasive candidiasis in China: 3 year national surveillance. J Antimicrobl Chem. 2015;70(3):802–810. https://doi.org/10.1093/jac/ dku460
- Mba IE, Nweze EI. Mechanism of Candida pathogenesis: revisiting the vital drivers. Eur J Clinic Microbiol Infect Dis. 2020;39(10):1797–1819. https://doi.org/10.1007/s10096-020-03912-w
- Gerard R, Sendid B, Colombel J-F, Poulain D, Jouault T. An immunological link between Candida albicans colonization and Crohn’s disease. Eur J Clin Microbiol Infect Dis. 2015;41(2):135–139. https://doi.org/10.3109/1040841X.2013.810587
- Wang H, Wu H, Li K-D, et al. Intestinal fungi and systemic autoimmune diseases. Autoimmun Rev. 2023;22(2):e103234. https://doi.org /10.1016/j.autrev.2022.103234
- Jangi S, Hsia K, Zhao N, et al. Dynamics of the gut mycobiome in patients with ulcerative colitis. Clinic Gastroenterol Hepatol. 2024;22(4):821–830. https://doi.org /10.1016/j.cgh.2023.09.023
- Gutierrez MW, van Tilburg Bernardes E, Changirwa D, McDonald B, Arrieta M-C. “Molding” immunity—modulation of mucosal and systemic immunity by the intestinal mycobiome in health and disease. Mucosal Immunol. 2022;15(4):573–583. https://doi.org/10.1038/s41385-022-00515-w
- Alonso-Monge R, Gresnigt MS, Román E, Hube B, Pla J. Candida albicans colonization of the gastrointestinal tract: a double-edged sword. Plos Pathog. 2021;17(7):e1009710. https://doi.org/ 10.1371/journal.ppat.1009710
- Lass-Flörl C, Kanj SS, Govender NP, Thompson III GR, Ostrosky-Zeichner L, Govrins MA. Invasive candidiasis. Nat Rev Dis Primers. 2024;10(1):e20. https://doi.org/10.1038/s41572-024-00503-3
- Chahine A, Farooqi S, Marzvanyan A, Michael M, Chavez-Frazier A, Guzman N. Mucocutaneous Candida infections in immunocompromised patients. Curr Derm Rep. 2022;11(2):73–88. https://doi.org/ 10.1007/s13671-022-00356-7
- Olum R, Baluku JB, Okidi R, Andia-Biraro I, Bongomin F. Prevalence of HIV-associated esophageal candidiasis in sub-Saharan Africa: a systematic review and meta-analysis. Tropical Medicine and Health. 2020;48:e82. https://doi.org/10.1186/ s41182-020-00268-x
- Carpintieri S, Uyar E, Buryk Y. Opportunistic infections and malignancies in a patient with HIV/AIDS and a critically Low CD4 Count of 1 Cell/μL. Cureus. 2024;16(5):e60129. https://doi.org/ 10.7759/cureus.60129
- Ucar S, Naik AQ, Zafar T. Cancer and fungal infections. In: Masood N, Yasmin A, eds. The Microbiome And Cancer: Understanding the Role of Microorganisms in Tumor Development And Treatment. Springer Nature; 2024:209–226.
- Caruso R, Lo BC, Chen GY, Núñez G. Host–pathobiont interactions in Crohn’s disease. Nat Rev Gastroenterol Hepatol. 2025;(6):395–414. https://doi.org/10.1038/s41575-024-00997-y
- Gedefie A, Shimeles G, Motbainor H, Kassanew B, Genet C. Vaginal colonization and vertical transmission of Candida species: prevalence and associated factors among pregnant women and their neonates at public health facilities of Northeast Ethiopia. BMC Pregnan Child. 2025;25(1):e22. https://doi.org/10.1186/s12884-024-07103-9
- Nagendra L, Mondal S, Bhattacharya S. Thyroid Disorders in the Tropics. Endotext; 2024.
- Ikuta KS, Meštrović T, Naghavi M. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(5):e268. https://doi.org/ 10.1016/s1473-3099(24)00102-6
- El-Ganiny AM, Yossef NE, Kamel HA. Prevalence and antifungal drug resistance of nosocomial Candida species isolated from two university hospitals in Egypt. Current Med Mycol. 2021;7(1):e31. https://doi.org/ 10.1016/s1473-3099(24)00102-6
- Aydin S, Derin O, Sahin M, et al. Epidemiology of nosocomial candidemia, mortality, and antifungal resistance: 7-year experience in Turkey. Jpn J Infect Dis. 2022;75(6):597–603.
- Prajapati J. Antifungal susceptibility and speciation of Candida isolated from blood at a tertiary care centre. Int J Med Med Res. 2024;10(1):32–39.
- Dutta A. Candidiasis: the laboratory report states that there are yeast in the blood culture! In: Domachowske J, ed. Introduction to Clinical Infectious Diseases: A Problem-Based Approach. Springer; 2025:487–493.
- Katsipoulaki M, Stappers MH, Malavia-Jones D, et al. Candida albicans and Candida glabrata: global priority pathogens. Microbiol Molecul Biol Rev. 2024;88(2):e00021-23. https://doi.org/10.1128/mmbr.00021-23.
- Malavika G, Ravi SSS, Maheswary D, Leela K, Lathakumari RH, Priya KSL. Role of Candida albicans in chronic inflammation and the development of oral squamous cell carcinoma. Cancer Pathog Ther. 2025. https://doi.org/ 10.1016/j.cpt.2025.03.002
- Casu C, Pinna M, Denotti G, Murgia M, Orru G. Association between C. albicans and leukoplakia and its treatment with photodynamic therapy: a review of the literature and a case report. World Cancer Res J. 2023;10:e2712. https://dx.doi.org/ 10.32113/wcrj_202312_2712
- Tasso CO, Ferrisse TM, de Oliveira AB, Ribas BR, Jorge JH. Candida species as potential risk factors for oral squamous cell carcinoma: systematic review and meta-analysis. Cancer Epidemiol. 2023;86:e102451. https://doi.org/10.1016/j.canep.2023.102451
- Ayuningtyas NF, Mahdani FY, Pasaribu TAS, et al. Role of Candida albicans in oral carcinogenesis. Pathophysiology. 2022;29(4):650–662. https://doi.org/10.3390/ pathophysiology29040051
- Yang Z, Zhang S, Ji N, Li J, Chen Q. The evil companion of OSCC: Candida albicans. 2024;30(4):1873–1886.https://doi.org/10.1111/odi.14700
- Abuhajar E, Ali K, Zulfiqar G, et al. Management of chronic atrophic candidiasis (denture stomatitis)—a narrative review. Int J Environ Res Public Health. 2023;20(4):e3029. https://doi.org/10.3390/ijerph20043029
- Katsipoulaki M, Stappers MH, Malavia-Jones D, Brunke S, Hube B, Gow NA. Candida albicans and Candida glabrata: global priority pathogens. Microbiol Molecul Biol Rev. 2024;88(2):e00021-23. https:// doi.org/10.1128/mmbr.00021-23
- Satora M, Grunwald A, Zaremba B, et al. Treatment of vulvovaginal candidiasis—an overview of guidelines and the latest treatment methods. J Clinic Med. 2023;12(16):e5376. https://doi.org/10.3390/jcm12165376
- Benedict K, Singleton AL, Jackson BR, Molinari NAM. Survey of incidence, lifetime prevalence, and treatment of self-reported vulvovaginal candidiasis, United States, 2020. BMC Women's Health. 2022;22(1):e147. https://doi.org/10. 1186/s12905-022-01741-x
- Hösükoğlu FG, Ekşi F, Erinmez M, Uğur MG. An epidemiologic analysis of vulvovaginal candidiasis and antifungal susceptibilities. Infect Microbe Dis. 2022;4(3):131–136. https://doi.org/10.1097/IM9.0000000000000095
- Shahabudin S, Azmi NS, Lani MN, Mukhtar M, Hossain MS. Candida albicans skin infection in diabetic patients: an updated review of pathogenesis and management. Mycoses. 2024;67(6):e13753. https://doi.org/10.1111/myc.13753
- Satora M, Grunwald A, Zaremba B, et al. Treatment of vulvovaginal candidiasis—an overview of guidelines and the latest treatment methods. J Clin Med. 2023;12(16):e5376. https://doi.org/10.3390/jcm12165376
- Pinho S, Miranda IM, Costa-de-Oliveira S. Global epidemiology of invasive infections by uncommon Candida species: a systematic review. J Fungi. 2024;10(8):e558. https://doi.org/10.3390/jof10080558
- Alves J, Alonso-Tarrés C, Rello J. How to identify invasive candidemia in ICU—a narrative review. Antibiotics. 2022;11(12):e1804. https://doi.org/10.3390/antibiotics11121804
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers. 2108;4:e18026. https://doi.org/10.1038/nrdp.2018.26
- Dutta A. Candidiasis: the laboratory report states that there are yeast in the blood culture! In: Domachowske J, ed. Introduction to Clinical Infectious Diseases: A Problem-Based Approach. Springer Nature; 2019:335–340.
- Makled AF, Ali SA, Labeeb AZ, et al. Characterization of Candida species isolated from clinical specimens: insights into virulence traits, antifungal resistance and molecular profiles. BMC Microbiol. 2024;24(1):e388. https://doi.org/10.1186/s12866-024-03515-x
- Won EJ, Sung H, Kim M-N. Changing epidemiology of clinical isolates of Candida species during the coronavirus disease 2019 pandemic: data analysis from a Korean Tertiary Care Hospital for 6 Years (2017–2022). J Fungi. 2024;10(3):e193. https://doi.org/10.3390/jof10030193
- Liu T, Sun S, Zhu X, Wu H, Sun Z, Peng S. Epidemiology, clinical characteristics, and outcome in candidemia: a retrospective five-year analysis from two tertiary general hospitals. BMC Infect Dis. 2025;25(1):e512. https://doi.org/10. 1186/s12879-025-10908-4
- Alenazy H, Alghamdi A, Pinto R, Daneman N. Candida colonization as a predictor of invasive candidiasis in non-neutropenic ICU patients with sepsis: a systematic review and meta-analysis. Int J Infect Dis. 2021;102:357–362. https://doi.org/10. 1016/j.ijid.2020.10.092
- Soulountsi V, Schizodimos T, Kotoulas SC. Deciphering the epidemiology of invasive candidiasis in the intensive care unit: is it possible? Infection. 2021;49(6):1107–1131. https://doi.org/10.1007/s15010-021-01640-7
- Lu S-Y. Oral candidosis: pathophysiology and best practice for diagnosis, classification, and successful management. J Fungi. 2021;7(7):e555. https://doi.org/10. 3390/jof7070555
- Candidiasis P, Candidiasis E, Glossitis MR, et al. Fungal and protozoal infections. In: Color Atlas of Oral and Maxillofacial Diseases. Elsevier Health Sciences; 2018:125–140.
- Romaneschi N. Effect of a Multispecies Probiotic with Fluconazole on Oral Candidiasis in Subjects with HIV. [master’s thesis]. Connecticut, United States; Yale University; 2024.
- Zeise KD, Woods RJ, Huffnagle GB. Interplay between Candida albicans and lactic acid bacteria in the gastrointestinal tract: impact on colonization resistance, microbial carriage, opportunistic infection, and host immunity. Clinic Microbiol. 2021;34(4):e00323-20. https://doi.org /10.1128/CMR.00323-20
- Sobel JD. Recurrent vulvovaginal candidiasis. Am J Obstet Gynecol. 2016;214(1):15–21. https://doi.org /10.1016/j.ajog.2015.06.067
- Nsenga L, Bongomin F. Recurrent candida vulvovaginitis. Venereology. 2022;1(1):114–123. https://doi.org/10.3390/venereology1010008
- Gonçalves B, Ferreira C, Alves CT, Henriques M, Azeredo J, Silva S. Vulvovaginal candidiasis: epidemiology, microbiology and risk factors. Critic Rev Microbiol. 2016;42(6):905–927. https://doi.org/ 10.3109/1040841X.2015.1091805
- Benedict K, Singleton AL, Jackson BR, Molinari NAM. Survey of incidence, lifetime prevalence, and treatment of self-reported vulvovaginal candidiasis, United States, 2020. BMC Women's Health. 2022;22(1):e147. https://doi.org/10. 1186/s12905-022-01741-x
- Bojang E, Ghuman H, Kumwenda P, Hall RA. Immune sensing of Candida albicans. J Fungi. 2021;7(2):e119. https://doi.org/10.3390/jof7020119
- Eckstein M-T, Moreno-Velásquez SD, Pérez JC. Gut bacteria shape intestinal microhabitats occupied by the fungus Candida albicans. Curr Biol. 2020;30(23):4799–4807. https://doi. org/10.1016/j.cub.2020.09.027
- Kumamoto CA, Gresnigt MS, Hube B. The gut, the bad and the harmless: Candida albicans as a commensal and opportunistic pathogen in the intestine. Curr Opinion Microbiol. 2020;56:7–15. https://doi.org/10.1016/j.mib. 2020.05.006
- Mochochoko BM, Pohl CH, O’Neill HG. Candida albicans-enteric viral interactions—the prostaglandin E2 connection and host immune responses. iScience. 2023;26(1):e105870. https://doi.org/ 10.1016/j.isci.2022.105870
- Sprague JL, Kasper L, Hube B. From intestinal colonization to systemic infections: Candida albicans translocation and dissemination. Gut Micro. 2022;14(1):e2154548. https://doi.org/10.1080/19490976.2022.2154548
- Jawhara SJM. How gut bacterial dysbiosis can promote Candida albicans overgrowth during colonic inflammation. Microorganisms. 2022;10(5):e1014. https://doi.org/10. 3390/microorganisms10051014
- Zeise KD, Woods RJ, Huffnagle GB. Interplay between Candida albicans and Lactic Acid Bacteria in the Gastrointestinal Tract: impact on Colonization Resistance, Microbial Carriage, Opportunistic Infection, and Host Immunity. Clinic Microbiol Rev. 2021;34(4):e00323-20. https://doi.org/ 10.1128/CMR.00323-20
- Bratburd JR, Keller C, Vivas E, et al. Gut microbial and metabolic responses to Salmonella enterica serovar typhimurium and Candida albicans. mBio. 2018;9(6):e02032-18. https:// doi.org/10.1128/mbio.02032-18
- Nagaoka I, Tamura H, Reich J. Therapeutic potential of cathelicidin peptide LL-37, an antimicrobial agent, in a murine sepsis model. Int J Mol Sci. 2020;21(17):e5973. https://doi.org/10.3390/ijms21175973
- Poissy J, Damonti L, Bignon A, et al. Risk factors for candidemia: a prospective matched case-control study. Crit Care. 2020;24:e109. https://doi.org/10.1186/s13054-020-2766-1
- Galloway-Peña JR, Kontoyiannis DP. The gut mycobiome: the overlooked constituent of clinical outcomes and treatment complications in patients with cancer and other immunosuppressive conditions. Plos Pathog. 2020;16(4):e1008353. https://doi.org/10.1371/journal.ppat.1008353
- Graf K, Last A, Gratz R, et al. Keeping Candida commensal: how lactobacilli antagonize pathogenicity of Candida albicans in an in vitro gut model. Dis Model Mech. 2019;12(9):edmm039719. https://doi.org/10.1242/dmm.039719
- Tong Y, Tang JJ. Candida albicans infection and intestinal immunity. Microbiol Res. 2017;198:27–35. https://doi.org/10.1016/j.micres.2017.02.002
- Alves R, Barata-Antunes C, Casal M, Brown AJ, Van Dijck P, Paiva S. Adapting to survive: how Candida overcomes host-imposed constraints during human colonization. Plos Pathog. 2020;16(5):e1008478. https://doi.org/10.1371/journal.ppat.1008478
- Rana A, Gupta N, Asif S, Thakur A. Surviving the storm: how Candida species master adaptation for pathogenesis. In: Hameed S, Vijayaraghavan P, eds. Recent Advances in Human Fungal Diseases: Progress and Prospects. Springer; 2024:109–155.
- Guinan J, Villa P, Thangamani S. Secondary bile acids inhibit Candida albicans growth and morphogenesis. Pathog Dis. 2018;76(3):efty038. https://doi.org/10.1093/femspd/fty038
- Chen H, Zhou X, Ren B, Cheng L. The regulation of hyphae growth in Candida albicans. Virulence. 2020;11(1):337–348. https://doi.org /10.1080/21505594.2020.1748930
- Dadar M, Tiwari R, Karthik K, Chakraborty S, Shahali Y, Dhama K. Candida albicans-Biology, molecular characterization, pathogenicity, and advances in diagnosis and control–An update. Microb Pathog. 2018;117:128–138. https://doi.org /10.1016/j.micpath.2018.02.028
- Ahmad S, Khan ZJ. Invasive candidiasis: a review of nonculture-based laboratory diagnostic methods.Indian J Med Microbiol. 2012;30(3):264–269. https://doi.org /10.4103/0255-0857.99482
- Mikulska M, Calandra T, Sanguinetti M, Poulain D, Viscoli C. The use of mannan antigen and anti-mannan antibodies in the diagnosis of invasive candidiasis: recommendations from the Third European Conference on Infections in Leukemia. Critical Care. 2010;14:1–14. https://doi.org/10.1186/cc9365
- Hoenigl M, Enoch DA, Wichmann D, Wyncoll D, Cortegiani A. Exploring European consensus about the remaining treatment challenges and subsequent opportunities to improve the management of invasive fungal infection (IFI) in the Intensive Care Unit. Mycopathologia. 2024;189(3):e41. https://doi.org/ 10.1007/s11046-024-00852-3
- Lorenzo-Villegas DL, Gohil NV, Lamo P, et al. Innovative biosensing approaches for swift identification of candida species, intrusive pathogenic organisms. Life. 2023;13(10):e2099. https://doi.org/10.3390/life13102099
- Bouza E, Almirante B, García Rodríguez J, et al. Biomarkers of fungal infection: expert opinion on the current situation. Rev Esp Quimioter. 2020;33(1):1–10. https://doi.org /10.37201/req/2260.2019
- Allkja J, Roudbary M, Alves AMV, Černáková L, Rodrigues CF. Biomaterials with antifungal strategies to fight oral infections. Critical Rev Biotechnol. 2024;44(6):1151–1163. https://doi.org/10.1080/07388551.2023.2236784
- Pereira R, Dos Santos Fontenelle R, De Brito E, de Morais SM. Biofilm of Candida albicans: formation, regulation and resistance. J Appl Microbiol. 2021;131(1):11–22. https://doi.org/10.1111/jam.14949
- Kumar A, Francis A, Hans S, Thakur A. Unravelling drug resistance in Candida species: genetic, biofilm, transcriptional, and epigenetic perspectives. In: Hameed S, Vijayaraghavan P, eds. Recent Advances in Human Fungal Diseases: Progress and Prospects. Springer; 2024:203–237.
- Atriwal T, Azeem K, Husain FM, et al. Mechanistic understanding of Candida albicans biofilm formation and approaches for its inhibition. Front Microbiol. 2021;12:e638609. https://doi.org/10.3389/fmicb.2021.638609
- Li B, Mao J, Wu J, et al. Nano-Bio interactions: biofilm-targeted antibacterial nanomaterials. Small. 2024;20(7):e2306135. https://doi.org/ 10.1002/smll.202306135
- do Carmo PHF, Garcia MT, Figueiredo-Godoi LMA, Lage ACP, Silva NSd, Junqueira JC. Metal nanoparticles to combat Candida albicans infections: an update. Microorganisms. 2023;11(1):e138. https://doi.org/10.3390/microorganisms11010138
- Kumar D, Kumar A. High throughput bioanalytical techniques for elucidation of Candida albicans biofilm architecture and metabolome. Rend Lincei Sci Fisiche Natu. 2023;34(1):117–129. https://doi.org /10.1007/s12210-022-01115-3
- Tscherner M, Giessen TW, Markey L, Kumamoto CA, Silver PA. A synthetic system that senses Candida albicans and inhibits virulence factors. ACS Synth Biol. 2019;8(2):434–444. https://doi.org/10.1021/acssynbio.8b00457
- Austermeier S, Kasper L, Westman J, Gresnigt MS. I want to break free–macrophage strategies to recognize and kill Candida albicans, and fungal counter-strategies to escape. Curr Opinion Microbiol. 2020;58:15–23. https://doi.org/10.1016/j.mib.2020.05.007
- König A, Hube B, Kasper L. The dual function of the fungal toxin candidalysin during Candida albicans—macrophage interaction and virulence. Toxins. 2020;12(8):e469. https://doi.org/10.3390/toxins12080469
- Williams TJ, Harvey S, Armstrong-James D. Immunotherapeutic approaches for fungal infections. Curr Opinion Microbiol. 2020;58:130–137. https://doi.org/10.1016/j.mib.2020.09.007
- Esher SK, Fidel PL, Noverr MC. Candida/staphylococcal polymicrobial intra-abdominal infection: pathogenesis and perspectives for a novel form of trained innate immunity. J Fungi. 2019;5(2):e37. https://doi.org/10.3390/jof5020037
- Van De Veerdonk FL, Netea MG, Joosten LA, Van Der Meer JW, Kullberg BJ. Novel strategies for the prevention and treatment of Candida infections: he potential of immunotherapy. FEMS Microbiol Rev. 2010;34(6):1063–1075. https://doi.org /10.1111/j.1574-6976.2010.00232.x
- d'Enfert C, Kaune A-K, Alaban L-R, et al. The impact of the Fungus-Host-Microbiota interplay upon Candida albicans infections: current knowledge and new perspectives. FEMS Microbiol Rev. 2021;45(3):efuaa060. https://doi.org/10.1093/femsre/fuaa060
- Zhao S, Shang A, Guo M, Shen L, Han Y, Huang X. The advances in the regulation of immune microenvironment by Candida albicans and macrophage cross-talk. Front Microbiol. 2022;13:e1029966. https://doi.org/10.3389/fmicb.2022.1029966
- Kunyeit L, Anu-Appaiah KA, Rao RP. Application of probiotic yeasts on Candida species associated infection. J Fungi. 2020;6(4):e189. https://doi.org/10.3390/jof6040189
- Allonsius CN, Vandenheuvel D, Oerlemans EFM, et al. Inhibition of Candida albicans morphogenesis by chitinase from Lactobacillus rhamnosus GG. Sci Rep. 2019;9:e2900. https://doi.org/10.1038/s41598-019-39625-0