| Review | Open Access |
|---|
Experiences of Young Clinical Psychologists Dealing with Clients having Different Sexual Orientations |
 |
|---|
![]() Hafsa Faryad, Zain Haider*, and Sadia Akbar
Hafsa Faryad, Zain Haider*, and Sadia Akbar
Lahore School of Behavioral Sciences, The University of Lahore, Pakistan
An exciting and challenging avenue for young clinical psychologists is to work with clients having different sexual orientations. The existing literature lacks the experience-based reporting of such challenges. Hence, by exploring these challenges, the training programs can be better planned. Hence, the current qualitative study used the phenomenology approach to explore the challenges experienced by young clinical psychologists dealing with clients having different sexual orientations. A purposive sample of eight young clinical psychologists was selected for a semi-structured interview. The descriptive phenomenology analysis identified four themes: (1) “training barrier”; (2) “construct diversity issues”; (3) “cultural challenges”; and (4) “therapists’ biases”. The common challenge experienced by the participants was the training barrier regarding assessment and intervention for mental health concerns of the clients having different sexual orientations. The results highlight the importance of incorporating the perspective of young clinical psychologists to plan better training programs in order to make them competent mental health service providers.
1. INTRODUCTION
Psychology is a diverse profession, and developing its workforce is particularly challenging due to the range of the sectors in which psychologists work (such as healthcare, academia, industry) and their diverse roles including those of clinical, teaching, research, consultation, and administrative nature (Robiner et al., 2014).
A clinical psychologist focuses on diagnosing and treating mental, emotional, and behavioral disorders. Some of the common disorders that might be treated include learning disabilities, substance abuse, sexual disorders, and eating disorders. There has been a growing movement to integrate the various therapeutic approaches, especially those with an increased understanding of issues regarding ethnicity, gender, spirituality, and sexual orientation, into clinical counseling services. Clinical psychologists may also work as part of a team with other professionals, such as social workers and nutritionists (Cleveland Clinic, 2025).
According to Kaczmarek (2006), there are some central unifying themes among clinical psychologists. These include a focus on an individual’s strengths, relationships, their educational and career development, as well as a focus on normal personalities. Clinical psychologists help people to improve their well-being, reduce and manage stress, and also improve their overall functioning in life.
The difficulties faced by young clinical psychologists in the early stages of their career may intensify when they encounter individuals with mental health concerns, along with having different sexual orientations. The LGBTQI acronym is used to refer to the community comprising individuals whose sexual orientation differs from being heterosexual. It is crucial to examine the specific challenges that young clinical psychologists encounter when working with LGBTQI clients (Moagi et al., 2021).
The term "sexual orientation" refers to a personality attribute that makes certain individuals more likely to be attracted to other individuals of the same sex (homosexual, gay, or lesbian), rather than to individuals of the opposite sex (heterosexual or straight), or to individuals of both sexes (bisexual) (Cook, 2021). A person's emotional attachment, romantic involvement, or sexual attraction to members of a certain gender (or genders) is referred to as their sexual orientation. These individuals may find themselves drawn to people arguing against gender (Bailey et al., 2016).
According to Arambula (2015) heterosexism is an ideological structure that is critical of and marginalizes any non-heterosexual identity, behavior, interaction, or organization. This ideology is pervasive in the discipline of psychology and is upheld by many practitioners, whether they are aware of it or not. Heterosexism can have an adverse effect on the psychological wellness and overall well-being of those who self-identify as LGBTQ+ by passing on prejudice and discrimination against them. Psychologists who take a sexual orientation-blind perspective may not realize that their own heterosexist beliefs can impact their therapy sessions (Ronzon-Tirad et al., 2023).
It's critical for therapists to be aware of their own biases and take action to make sure that their therapeutic methods are accepting of people of all sexual orientations (Morrow, 2000). A homosexual is a person attracted to other people of the same gender. The word "homosexual" comes from the Greek word "homos," which means "the same." This term is frequently used to describe people who are attracted romantically or sexually to other people of the same gender. However, it should be remembered that a person's sexual orientation is additionally determined by their natural attraction towards people and not just by their sexual behavior. Accordingly, the term "homosexual" refers to a person's general sexual orientation, rather than the sexual activities and relationships between people of the same sex (Isaiah, 2012).
Research has repeatedly demonstrated that sexual orientation is not something that can be deliberately chosen or changed. Rather, it is likely determined by a complex interaction of genetic, hormonal, and environmental variables. Therefore, it is not accurate to view homosexuality as a choice or behavior that can be controlled (Ahmed, 2006).
Sexual orientation is one of the major sex differences in human beings. The vast majority of the human population is heterosexual, that is, they are attracted to members of the opposite sex. However, a small but significant proportion of people are bisexual or homosexual and experience attraction to members of the same sex. The origins of the phenomenon have long been the subject of scientific study (Ngun & Vilain, 2014).
As individual’s age, they may experience a range of emotional responses, including anxiety, depression, grief, guilt, helplessness, and loneliness. These emotions are not exclusive to any particular sexual orientation and both LGBTQI+ and heterosexual older adults experience them. However, it is essential to recognize that older LGBTQI+ people may suffer particular difficulties and experiences linked to their sexuality or gender identity, which may have an effect on their psychological well-being (Fowler et al., 2023).
Different types of orientations fall under the category of sexual orientation, including same sex (homosexual), opposite sex (heterosexual), and both sexes (bisexual). Recognizing that sexual orientation includes a person's overall attractiveness is crucial since sexual orientation is not defined solely by sexual behavior. A more inclusive vocabulary that recognizes the full range of sexual orientations and identities has replaced outdated terminology and classification schemes. The presence of LGBTQI identities in Pakistan is an undeniable element of South Asian history. Indeed, the evidence of their existence in the subcontinent can be found in queer narratives and autobiographical records, particularly from the Mughal era (Mitchell et al., 2015).
In an experiment, Bowers and Bieschke (2005) discovered that psychologists tended to view a fictional homosexual, lesbian, and gay client as less healthy on certain dimensions than a fictional heterosexual client. Eliason and Schope (2001) suggested that gay and lesbian individuals may feel hesitant about seeking therapy due to the negative attitudes and a lack of information among healthcare professionals.
Psychology is a broad and evolving discipline, encompassing various roles including clinical work, teaching, research, and consultation (Robiner et al., 2014). In Pakistan, although the profession of clinical psychology is well-established, yet it lacks guidelines for professionals to effectively deal with sensitive and marginalized populations, such as the LGBTQI community (Mitchell et al., 2015). To the best of our knowledge, the reason is the under-exploration of the therapeutic alliance between young clinical psychologists and LGBTQI clients in Pakistan. The existing literature suggests that therapists' own biases and lack of cultural competency may unintentionally disseminate heterosexist ideologies (Arambula, 2015; Ronzon-Tirad et al., 2023). The impact of such practices may result in wrong-diagnosis, insufficient care, or event reluctance among LGBTQI individuals to seek psychological treatment (Bowers & Bieschke, 2005; Eliason & Schope, 2001). Furthermore, early-career psychologists in Pakistan are not given formal training or supervision on LGBTQI-related issues, leading to challenges when addressing the clients' sexual orientation in practice. Moagi et al. (2021) highlighted how these difficulties can affect a clinician’s effectiveness and psychological resilience. Thus, exploring the voices of early-career clinical psychologists in depth would serve the foundational purpose of developing culturally informed services.
Research QuestionWhat are the experiences of young clinical psychologists working with people having different sexual orientations?
Method
Research DesignA qualitative (phenomenological) research design was employed to execute this study.
Data Collection Sample and Sampling TechniquePurposive sampling technique was employed in this study. The sample included eight professionals working in the mental health field (all young clinical psychologists) in Pakistan. Semi-structured interviews were conducted till the point of saturation.
In total, seven female psychologists participated in the interviews. The interviews consisted of semi-structured questions to gain an in-depth understanding of the challenges faced by these psychologists when working with clients of different sexual orientations. Following the protocol of interview guidelines, open-ended and non–directive questions were devised so that the participants could comfortably and extensively share their experiences concerning different sexual orientations.
Inclusion Criteria- Only young clinical psychologists living and working in Pakistan were included in this study.
- b) Only young clinical psychologists in the initial years of their career were included.
- b) Clinical psychologists with a minimum one-year experience were included.
- Clinical psychologists working in the academia were excluded.
Demographic information sheet filled by the participants included their name, age, gender, education, marital status, family status, job experience, and the nature of employment (government or private). All the demographic information collected from the participants is given below in Table 1.
Table 1
Demographic Characteristics of the Participants with Pseudo Names (N = 7)|
Name |
Age |
Gender |
Education |
Practicing Experience |
Family System |
Marital Status |
Job Type |
|---|---|---|---|---|---|---|---|
|
Aliya |
26 |
Female |
Ms. Clinical psychology |
1year |
Nuclear |
Single |
Private |
|
Kiran |
27 |
Female |
Ms. Clinical psychology |
1 year |
Nuclear |
Single |
Private |
|
Saima |
28 |
Female |
Ms. Clinical psychology |
1year |
Nuclear |
Single |
Private |
|
Asma |
25 |
Female |
Ms. Clinical psychology |
1 year |
Joint |
Single |
Private |
|
Atiqa |
30 |
Female |
Ms. Clinical Psychology |
1 year |
Joint |
Married |
Private |
|
Hareem |
29 |
Female |
Ms. Clinical psychology |
1year |
Joint |
Married |
Private |
|
Hajra |
27 |
Female |
Ms. Clinical psychology |
1year |
Joint |
Single |
Private |
The data were analyzed using the six-step approach of Braun and Clarke (2006). In the first phase, interviews were transcribed and read carefully. In the second phase, based on multiple careful readings, codes were generated resulting in the reduction of data into meaningful smaller units (Creswell, 2014). In the third phase, themes were identified based on grouping together similar codes. In the fourth phase, the initial themes were reviewed and a few were modified, such as the “lack of training” into “training barrier”. In the fifth and the last phase, the reviewed themes were used to report the findings.
ProcedureA permission letter was obtained from the pertinent university for collecting data and delivered to different professionals. Data was collected from young clinical psychologists. The process included a written consent for interview and recording the interview, while the subjects were briefed about the purpose and nature of the study and the amount of time needed for the interview. An interview guide was developed for conducting the interviews with the participants. Initially, the interviews were translated following the forward translated method from Urdu to English. Afterwards, the interview data was entered into NVivo14 for coding and theme extraction. Pseudo names were used to present the narratives of the study participants as provided below.
Results
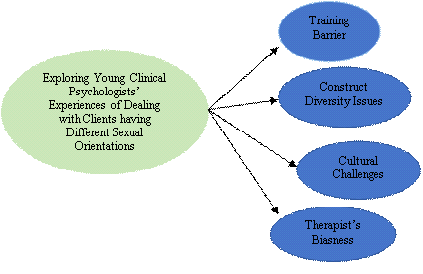
In this study, four themes were generated after the process of NVivo 14 data analysis, including (i) Training Barrier, (ii) Construct Diversity Issues, (iii) Cultural Challenges, and (iv) Therapist’s Biasness. A summary of all the themes is provided by Figure 1.
Figure 1Thematic Map
This theme was identified by five participants. Many of the participants reported training barrier, as well as ethical consideration about sexual diversity as a subordinate theme, due to multiple issues while dealing with clients. The verbatim of Asma depicted this theme in the following way,
“Not really sexual orientation related training was provided. Even, no material was provided by our supervisor. But I did related studies with LGBTQI clients.”
Another participant reported about the lack of education and professional training during the study,
“No training was given on LGBTQI by our supervisor during placement although I had patients of homosexuality now this type of patient is present everywhere. Even many people get shy while talking about LGBTQI.”
A third participant’s named Hajra verbatim also depicted that the training barrier impacts on developing therapeutic alliance,
The biggest challenge I faced, I did not have the adequate knowledge to deal with these clients. It’s very tough to build rapport with females. Female are Very Resistant such as they will not give you eye contact. Females did not use the element of humor with you because they kept themselves very conscious so that transference doesn't take place. Females are quite afraid as compare to men.
While emphasizing professional training a participant stated, “Even in hospitals, sexual training is not given on IGBTQI, even in universities, and psychotherapy education related to it is not given.”
Five of the eight participants reported ethical consideration as a subordinate theme while working with these clients using the following verbatim, “There is also a factor of confidentiality. Which you have to do inside rapport building. The client should be given enough regard to trust you.”
While considering the related studies with sexual orientation, eight research participants supported the subordinate theme with the following examples,
“We were given general idea to deal with sexual orientation. We covered half book in the syllabus course. Our placement supervisor provided us books related to sexual disorder.”
“I had theoretical knowledge related to LGBTQI. Placement supervisor guided us other than this I studied myself related to this topic and exposure was developed with related knowledge.”
Construct Diversity IssuesThis subordinate theme was identified by the eight participants of the study. LGBTQI individuals are often misrepresented or not represented at all in the media, literature, and other cultural representations. This lack of visibility perpetuates stereotypes and erases their diverse experiences, contributing to further marginalization (McInroy & Craig, 2017). One of the study respondents Hareem reported that
“Young clinical psychologists should have diverse knowledge dealing with LGBTQI clients. Media also misrepresent these individuals and our society don’t accept them as normalize human beings.”
While talking about LGBTQI terminology, another participant described the lesbian, gay, bisexual, transgender, queer, and inter-sexual community as follows,
Basically, there are different sexual orientations. We define them as people who are attracted to gender. People who are little different from our societal norm. For example, L stands for lesbian, the woman who is attracted to women. G for gay, men find men attractive for bisexual, people who are attracted towards both genders. T is for transsexuals, people who change their gender/sex by any kind of medicine/surgery. I am for intersex, people who are born with any kind of biological deformity, which falls under the criteria of not being a male or female. They don't have a defined gender/sex which is called intersex. Other than that there are asexual people who are not sexually attracted to any gender.
Moving on to gender identity, it could be determined as the understanding of gender identity has developed over time to encompass individuals who do not identify exclusively as female or male. Gender identity refers to a person's self-perception of their gender, irrespective of their biological sex (Rubin et al., 2020).
According to one of the study respondents, “I got a bisexual male saying that I belong to the LGBTQI community, he said that he has HIV/AIDS problem and I am in a different sexual relationship with boys.”
The 5th and 6th participants reported about resultant infertility consequences through the manifestation of several statements respectively, “There is no issue of their physical health. If physical organs are used before time, then when the time comes when you have to have sex with your partner, infertility can occur.”
Another participant described the relationship between sex and gender using the following examples,
Sex is defined at birth and it is actually depending on our sexual organs in which our sex is assigned to us at birth. However, gender is psychological identification with certain gender groups then biological one. We can say that sex is biological in nature and gender is more psychological.
One of the research respondents, while sharing views about pubertal milestones, stated that
Basically, children start puberty in teenage, then children do not have any sense of knowledge, what they see from social media, they are unable to discuss with anyone. Children don’t know how to tell their interest. They develop sexual urges in teen age. They start masturbation due to early developed milestones.
Social and Religious ScriptsAfter analyzing all the factors responsible for cultural changes, this subtheme emerged from the subordinate themes. In this study, several obstacles such as cultural and religious values, stigma, social discrimination, and problems faced by minority communities have been identified. These problems unpleasantly affect these minority groups, such as the LGBTQI community, particularly in developing countries like Pakistan. The verbatim of the participants have been included to further clarify the theme. One of the study participants reported that
“People with different sexual orientation struggle in Pakistan as compared to foreign countries for their acceptance. Mainly psychologist should focus on unconditional positive regard, active listening so that trust should develop.”
The second participant also reported about cultural challenges in the following words,
“There were also challenges of societal norm. Secondly bunch of psychologists didn't remain neutral while dealing such clients. Due to our culture and religion pressure, they don’t disclose their secrets. Therefore, therapist need to developed rapport to provide them safe space.”
The manifestation of another participant with reference to the cultural biasness barriers is described in the following verbatim,
“The case (different sexual orientation) is very common now. It is legalizing and normal in foreign countries but in our country and religion it’s not normal. So, it is black area if we talk about LGBTQI in our culture.”
It is extremely challenging to completely evade encountering the stigma surrounding sexual minorities. The experiencing of stigma and discrimination has been described as minority stress, which can have harmful effects on the physical and emotional well-being of individuals belonging to sexual minority populations (Meyer, 2013). The hurdles related to social discrimination and stigmatization are reported by one of the participants as follows,
Yes, a case was related to sexual orientation. People come to us like this, but there are hidden things because there is a lot of stigmatizations in our society, people are unable to improve their mental health due to societal stigmatization and people do not have awareness of mental health.
Pakistan is a Muslim country. Islam strictly prohibits haram relationships as expressed by one of the participants as follows,
“In Islam it is (different sexual orientation) not called halal when DSM call it normal and this is a challenge. Religiously it is very difficult to accept people are attracted towards bisexual, homosexual.”
Another participant’s response considering Islam is given under,
“Religious plays a sensitive role in our society. These things (different sexual orientation) are common in children of age 13 to 20 years. The thing which is prohibited in Islam, we cannot accept it on any ground.”
Therapist BiasnessIn this study, the participants reported that they experienced biased behavior from their senior peers and therapists. Moreover, unconditional positive regard should also be considered. The verbatim of the participants have been included to clear any ambiguity. All of the eight participants reported this subordinate theme while working with individuals of different sexual orientations. Considering therapist biasness, their verbatim are as follows,
“Wherever every person is working, there are seniors. Let's take this issue further with the senior. Seniors take this matter in their own way due to which the junior therapist gets confused that how to deal with this client.”
The verbatim of another participant are coded as under,
“Other than this unconditional positive regard is very crucial so that client can trust you. Apart from this, there is also a factor of confidentiality. Therapist should be non-judgment.”
Another respondent reported that
“Therapists should work collaboratively with senior clients, involving them in decision-making processes and jointly developing treatment plans. This collaborative approach can help address confusion and foster a sense of ownership in the therapeutic process.”
Two of the eight participants reported the subordinate theme of workplace hierarchy in the following words,
My personal views are that Pakistan is an Islamic country. People also struggle in foreign countries for their acceptance. Relatively Pakistan in foreign countries acceptance is there. Judgment is here. Mainly psychologist should focus on unconditional positive regard, active listening so that trust should develop. New therapist doesn’t want to work with LGBTQI clients.
Discussion
This study examined the assessment-related difficulties experienced by therapists when working with LGBTQI clients. The research produced a number of themes, such as the use of informal assessments, the need for expertise in assessing sexual orientation, difficulties in establishing trust and disclosing information, co-occurring conditions, diagnostic-related barriers, construct diversity issues, cultural difficulties, training barrier, and reported symptomology in LGBTQI clients. The findings were examined in connection to the body of literature in existence and their implications for clinical practice were addressed.
The study's key conclusion is that many participants relied heavily on informal assessment techniques including interviews. This is consistent with earlier studies showing the preference for informal approaches to determine sexual orientation (Smith et al., 2017). On the other hand, one participant claimed they did not employ any particular instruments linked to sexual orientation, which may be explained by the dearth of standardized tests created especially for this community. However, the participants acknowledged the value of employing formal diagnostic tests based on accepted guidelines including the DSM when they are required. This outcome is in line with the literature, which emphasizes using clinical judgement in addition to formal evaluation techniques for assessing mental health concerns (Meyer et al., 2008).
This study identifies the necessity for competence in identifying sexual orientation as a crucial subject. The participants emphasized the importance of using interviews to learn about childhood experiences and attractions as well as enhancing their clinical abilities. This finding is consistent with previous research emphasizing the value of using a thorough approach to comprehend the complexity of sexual orientation (Meyer, 2013). In light of the growing number of instances and the demand for specialized expertise, the participants suggested pursuing professional training in the field of LGBTQI. This outcome is consistent with earlier research that argued for the inclusion of LGBTQI-related instruction and material in psychology programmes to improve the clinicians' ability to interact with this community (Goldfried & Drescher, 2012; Haldeman, 2016). Also, the assessment procedure with LGBTQI clients must take into account issues with transparency and trust building. The participants emphasized how the patients were uncomfortable disclosing their sexual orientation and afraid of being judged for it. This result is in line with earlier studies showing that LGBTQI people are reluctant to disclose their sexual orientation due to worries about discrimination and stigma (Hatzenbuehler et al., 2020). As a key tactic used by the participants to build rapport and encourage disclosure, the need for creating a safe and judgment-free environment arose. This is consistent with literature that highlights the value of establishing a therapy setting that is affirming and promotes transparency and trust (Meyer, 2013).
It has been noted that a key factor in assessing LGBTQI clients is the existence of mental illnesses, such as depression and anxiety. This result is in line with recent research showing higher rates of mental health issues in this demographic (Marshal et al., 2011). Hence, The need of a thorough evaluation to guide treatment planning and interventions was emphasized by the participants, coupled with the need to address these co-occurring conditions during the assessment process. Furthermore, the absence of sexually associated diseases in the diagnostic criteria, particularly the DSM, was specifically cited by the participants as a diagnostic hurdle. This result highlights the inadequacies of the current diagnostic paradigms in capturing the particular experiences and mental health requirements of LGBTQI people. It supports earlier research that called for the expansion and updating of diagnostic criteria to more accurately reflect the varied sexual orientations and associated mental health issues (Levounis & Drescher, 2010).
Furthermore, concerns about construct diversity emerged as a prominent theme, highlighting how crucial it is for clinical psychologists to have a diverse knowledge base when working with LGBTQI clients. The participants cited societal rejection and inaccurate media portrayals of these people as barriers. This outcome is consistent with earlier studies highlighting the importance of cultural competence and the comprehension of the sociocultural environment of LGBTQI people (American Psychological Association, 2012).
The findings of this study emphasize the significance of doctors being aware of the various sexual orientations and identities within the LGBTQI community, while encouraging understanding and valuing the varied experiences of their clients. Another issue found during the assessment process was cultural challenges. The participants talked about stigma, societal discrimination, cultural and religious norms, and the difficulties LGBTQI people encounter in societies that do not fully embrace them. These results are consistent with the material already published on the effects of cultural and societal influences on the mental health and general wellbeing of LGBTQI people (Meyer, 2013).
The participants emphasized the need of creating a safe environment that recognizes and respects the clients' cultural backgrounds, as well as giving them unconditional positive esteem. One major issue mentioned by the participants was the absence of training in working with LGBTQI clients. They emphasized the lack of specialized education and the demand for professional training in the field of sexual diversity. This finding is consistent with earlier research showing that mental health practitioners lack proper training and understanding when working with the LGBTQI community (Meyer et al., 2008). The participants in the discussion highlighted the significance of including LGBTQI-related content in psychology training programs and providing opportunities for ongoing professional development.
The participants also reported that many clients they see with different sexual orientations mostly come with depression, anxiousness, suicidal ideation, and body dysmorphic related issues. These results are consistent with the studies showing that the members of LGBTQI community have higher rates of mental health issues and suicidality (Marshal et al., 2011; Meyer, 2013). The reported symptoms highlight the importance of mental health practitioners having up-to-date knowledge of these problems and offering proper diagnostic and therapeutic procedures. Overall, the results of this study help us to understand the assessment-related difficulties that clinicians encounter, while working with LGBTQI clients.
Conclusion
Overall, the findings support prior research and highlight the need of specialized knowledge, cultural sensitivity, and the provision of a secure and supportive atmosphere in therapeutic practice. They also underline the significance of continued professional development, the inclusion of LGBTQI-related material in psychology programs, and the updating of diagnostic frameworks to more accurately reflect the experiences and mental health problems of LGBTQI people. Clinicians can better serve LGBTQI clients by addressing these challenges and improving the effectiveness and sensitivity of their examinations.
A number of evidence-based recommendations can be made in this stance. For example, FB groups and social media applications should be used to normalize the existence of this community. Different sexual orientations are a black area not only in our culture but Islam also prohibits it. Although, foreign communities consider it normal because it is not a sin. In future, studies could be carried out in collaboration with psychiatrist, social workers as well as with other professionals. In addition, this area of research could be examined through conducting quantitative research.
Implications and Suggestions
The results can be used to build training programs for aspiring clinical psychologists that incorporate specialized understanding and abilities to work with people of various sexual orientations. The insights gained from this study can be utilized to enhance ongoing professional development opportunities for clinical psychologists, ensuring that they remain competent in supporting clients with different sexual orientations. The study can help to inform the creation of rules and regulations to promote welcoming and affirming cultures within mental health organizations, encouraging equal access to treatment for people with various sexual orientations.
This study allowed us to explore the challenges facing young clinical psychologists while dealing with clients with different sexual orientations. Until mental health professionals have an excellent knowledge about factual concerns related to different sexual orientations and possess the attitudes and skills enabling them to treat such clients effectively, such clients will fail to receive the services they deserve and need.
Limitations and Future Direction
This study provides valuable insights into the challenges young clinical psychologists face with LGBTQI clients in Pakistan, particularly considering training gaps, cultural stigma, and biases. However, sample limitations, lack of theoretical framing, and insufficient methodological detail weaken its robustness. Future research should include a diversified participant sample, integrate theory, and explore actionable solutions for LGBTQI-affirmative care in restrictive settings.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding Details
No funding has been received for this research.
REFERENCES
Ahmed, M. B. (2006). Homosexuality: An Islamic perspective. Journal of the Islamic Medical Association of North America, 38(1), 27–33. https://doi.org/10.5915/38-1-6275
American Psychological Association. (2012). Guidelines for psychological practice with lesbian, gay, and bisexual clients. The American Psychologist, 67(1), 10–42. https://doi.org/10.1037/a0024659
Arambula, C. (2015). Heterosexism, harassment, discrimination, and coping mechanisms among lesbian, gay, bisexual, transgender, and questioning individuals (Publication No. 3731767) [Doctoral dissertation, Texas A&M University-Kingsville]. ProQuest Dissertations & Theses.
Bailey, J. M., Vasey, P. L., Diamond, L. M., Breedlove, S. M., Vilain, E., & Epprecht, M. (2016). Sexual orientation, controversy, and science. Psychological Science in the Public Interest, 17(2), 45–101. https://doi.org/10.1177/1529100616637616
Bowers, A., & Bieschke, K. J. (2005). Psychologists' clinical evaluations and attitudes: An examination of the influence of gender and sexual orientation. Professional Psychology: Research and Practice, 36(1), 97–103.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Cleveland Clinic. (2025, February 18). Psychologist. https://my.clevelandclinic.org/health/articles/22679-psychologist
Cook, C. C. (2021). The causes of human sexual orientation. Theology & Sexuality, 27(1), 1–19. https://doi.org/10.1080/13558358.2020.1818541
Creswell, J. W. (2014). Research design: Qualitative, quantitative and mixed methods approaches (4th ed.). Sage Publications.
Eliason, M. J., & Schope, R. (2001). Does “don't ask don't tell” apply to health care? Lesbian, gay, and bisexual people's disclosure to health care providers. Journal of the Gay and Lesbian Medical Association, 5, 125–134. https://doi.org/10.1023/A:1014257910462
Fowler, J. A., Buckley, L., Muir, M., Viskovich, S., Paradisis, C., Zanganeh, P., & Dean, J. A. (2023). Digital mental health interventions: A narrative review of what is important from the perspective of LGBTQIA+ people. Journal of Clinical Psychology, 79(11), 2685–2713. https://doi.org/10.1002/jclp.23571
Goldfried, M. R., & Drescher, J. (2012). What constitutes effective consultation for therapists working with lesbian, gay, and bisexual individuals? Professional Psychology: Research and Practice, 43(5), 478–485. https://doi.org/10.1037/0735-7028.36.1.66
Haldeman, D. C. (2016). Therapeutic competence in sexual orientation. In M. M. Lebowitz (Ed.), Competence in clinical practice: A guidebook for the competency-focused training of psychological practitioners (pp. 65–85). Oxford University Press.
Hatzenbuehler, M. L., Rutherford, C., McKetta, S., Prins, S. J., & Keyes, K. M. (2020). Structural stigma and all-cause mortality among sexual minorities: Differences by sexual behavior? Social Science & Medicine, 244, Article e112463. https://doi.org/10.1016/j.socscimed.2019.112463
Isaiah, A. B. (2012). Knowledge and attitude of undergraduate students towards homosexuality and its implication on social adjustment: A study of Caritas university Amorji-Nike, Emene, Enugu State [Bachelor thesis, Caritas University]. Studocu. https://www.studocu.com/row/document/university-of-ibadan/clinical-psychology-materials/knowledge-and-attitude-of-undergraduate-students-towards-homosexuality/74675990
Kaczmarek, P. (2006). Counseling psychology and strength-based counseling: A promise yet to fully materialize. The Counseling Psychologist, 34(1), 90–95. https://doi.org/10.1177/0011000005282371
Levounis, P., & Drescher, J. (2010). Psychiatrists' attitudes toward DSM-5 proposals for paraphilias: Results from an online survey. Journal of Sexual Medicine, 7(5), 1886–1893. https://doi.org/10.1007/s10508-010-9657-5
Marshal, M. P., Dietz, L. J., Friedman, M. S., Stall, R., Smith, H. A., McGinley, J., Thoma, B. C., Murray, P. J., D’Augelli, A. R., & Brent, D. A. (2011). Suicidality and depression disparities between sexual minority and heterosexual youth: A meta-analytic review. Journal of Adolescent Health, 49(2), 115–123. https://doi.org/10.1016/j.jadohealth.2011.02.005
McInroy, L. B., & Craig, S. L. (2017). Perspectives of LGBTQ emerging adults on the depiction and impact of LGBTQ media representation. Journal of Youth Studies, 20(1), 32–46. https://doi.org/10.1080/13676261.2016.1184243
Meyer, I. H. (2013). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
Meyer, I. H., Schwartz, S., & Frost, D. M. (2008). Social patterning of stress and coping: Does disadvantaged social statuses confer more stress and fewer coping resources? Social Science & Medicine, 67(3), 368–379. https://doi.org/10.1016/j.socscimed.2008.03.012
Mitchell, R. C., Davis, K. S., & Galupo, M. P. (2015). Comparing perceived experiences of prejudice among self-identified plurisexual individuals. Psychology & Sexuality, 6(3), 245–257. https://doi.org/10.1080/19419899.2014.940372
Moagi, M. M., van Der Wath, A. E., Jiyane, P. M., & Rikhotso, R. S. (2021). Mental health challenges of lesbian, gay, bisexual and transgender people: An integrated literature review. Health SA Gesondheid, 26(1), 1–12.
Morrow, S. L. (2000). First do no harm: Therapist issues in psychotherapy with lesbian, gay, and bisexual clients. In R. M. Perez, K. A. DeBord, & K. J. Bieschke (Eds.), Handbook of counseling and psychotherapy with lesbian, gay, and bisexual clients (pp. 137–156). American Psychological Association.
Ngun, T. C., & Vilain, E. (2014). The biological basis of human sexual orientation: Is there a role for epigenetics? Advances in Genetics, 86, 167–184. https://doi.org/10.1016/B978-0-12-800222-3.00008-5
Robiner, W. N., Dixon, K. E., Miner, J. L., & Hong, B. A. (2014). Psychologists in medical schools and academic medical centers: Over 100 years of growth, influence, and partnership. American Psychologist, 69(3), 230–248. https://psycnet.apa.org/doi/10.1037/a0035472
Ronzón-Tirado, R., Charak, R., & Cano-González, I. (2023). Daily heterosexist experiences in LGBTQ+ adults from Spain: Measurement, prevalence, and clinical implications. Psychosocial Intervention, 32(1), 1–10. https://doi.org/10.5093/pi2022a15
Rubin, J. D., Atwood, S., & Olson, K. R. (2020). Studying gender diversity. Trends in Cognitive Sciences, 24(3), 163–165.
Smith, M. S., Fingerhut, A. W., Gamarel, K. E., O’Cleirigh, C., Joseph, H. A., & Kershaw, T. S. (2017). Measuring sexual orientation with the Kinsey Scale: A comprehensive systematic review. Journal of Sex Research, 54(4-5), 464–497. https://doi.org/10.1080/00224499.2016.1255872
Appendix A
Interview Protocol
Main interview questions
Questions that were asked from the participants are given below:
- Which type of cases you dealt with during your supervised adult clinical placements?
- Were you given trainings on dealing with clients having different sexual orientations?
- What do you know about LGBTQI clients?
- When did you start practicing as clinical psychologist after completion of your degree?
- Will you please describe your experiences as young clinical psychologist dealing with clients of different sexual orientations?
- Will you please explain your experiences while psychological assessment of such clients?
- Will you please explain your experiences of providing psychotherapy to such clients?
- Are there any other kind of barriers you experienced as young clinical psychologist dealing with such clients?
- What kind of suggestions and recommendations will you provide to young clinical psychologist who will be interested in dealing with such clients?