Moderating Effects of Optimism, Happiness, and Psychological Well-being on Resilience and Pain Catastrophizing among Chronic Pain Survivors
Owais Ahmad*, Shamsa Siddiq, and Farhana Kazmi
Department of Psychology, Hazara University, Mansehra, Pakistan
ABSTRACT
The current study aimed to examine whether optimism, happiness, and psychological well-being impact resilience and pain catastrophizing. It is widely recognized that individuals with chronic pain often catastrophize about their condition, which can lead them into more distressing situations. The study determined that resilience has a relationship with pain catastrophizing and positive constructs, for instance, optimism, happiness, and psychological well-being moderate this relationship. Using a cross-sectional research design, the study recruited 375 participants through purposive sampling from different public and private hospitals in Abbottabad and Swabi. Bivariate correlations, independent sample t-test, and multiple moderation analyses were run to analyze the data using SPSS version 29. The study revealed a handful of insights that resilience, optimism, happiness, and psychological well-being are positively related to each other significantly. It was concluded that optimism, happiness, and psychological well-being significantly moderated the relationship between resilience and pain catastrophizing. The study empowered counselors, community workers, and medical experts to implement resilience training programs at community levels so that individuals would be mentally equipped before facing any health crisis due to chronic pain.
1. INTRODUCTION
Chronic pain is a common illness that has several negative repercussions. It affects more than 30% of the world's population. Its prevalence percentages differ depending on health state and pain cause, with multiple sclerosis (44% to 80%), spinal cord injuries (80%), neuromuscular disease (73%), and post-polio syndrome (91%). Chronic pain has long been connected to physical, psychological, and social functioning (Furrer et al., 2017).
Chronic pain is among the utmost communal problems encountered in emergency departments. Undertreatment persists even though between 70 and 90% of emergency department visits are related to pain complaints. Lack of treatment raises the possibility of chronic pain. Pain that lasts longer than three months is one of the many definitions of chronic pain that have been put forth. Chronification is the process by which acute discomfort develops into long-term, chronic pain. This chronification of pain may have a variety of negative consequences, including decreased quality of life, excessive pharmaceutical use, lost productivity, and the risk of opioid dependence (Voon et al., 2017).
Chronic pain considerably impacts one's physical and psychological health. Individuals who suffer from chronic pain frequently report coexisting psychological problems, such as depression and low mood. This is concerning because the patients' degree of functioning and the overall well-being is significantly impacted by both concurrent pain and depression (Flink et al., 2015). Similarly, Khan et al. (2020) investigated the role of fear-avoidance beliefs, which are closely associated to pain catastrophizing, in people with chronic low back pain (CLBP) in Pakistan. The findings revealed that catastrophizing strongly mediated the connection between pain intensity and disability, accounting for 81% of pain intensity's total impact on disability. This emphasizes the importance of psychological elements, such as catastrophizing, in the experience and management of chronic pain among the Pakistani population.
Pain catastrophizing is one psychological component specific to pain. It is the propensity to spend time in rumination and hopelessness. Individuals who are prone to exaggerate their pain are more likely to experience the amplification of their current pain, the development of chronic pain, and a decline in their physical function (Alschuler et al., 2013). Pain catastrophizing, according to empirical research, contributes to increased pain severity, disability, and mental distress. When people are fighting a physical illness, they are also fighting psychological effects. This fighting has a far-reaching effect on many aspects of patients' lives, which may lead towards a reduction in quality of life (Afrashteh et al., 2023).
In individuals suffering from chronic pain, catastrophizing is associated with lower positive affect and higher levels of negative affect. Therefore, one major risk factor for mental distress among individuals managing a chronic pain is pain catastrophizing. Individuals who participate in resilience-building programs after having undergone severe physical injuries return to work in less time (Nwankwo et al., 2021). Additionally, optimism seems to be a construct that represents the degree to which people have generally positive future expectations. Optimism is important in adapting to challenging situations. When faced with a task, optimists demonstrate greater perseverance, even if progress is arduous and sluggish. Previous research has shown that optimism is a characteristic that contributes to resilience. Moreover, it has also been recognized as the most effective factor in reducing the negative effects of pain (Boselie & Peters, 2023).
Furthermore, psychological well-being is characterized as a state of health that leads towards a comprehensive understanding of personal integrity, including spiritual aspects of life. According to Trompetter et al. (2016), psychological well-being is a significant and independent factor affecting chronic pain as well as distress and physical disability. A person's main goal is to maintain their psychological well-being, which includes their life objectives, sense of potential, and interpersonal relationships.
Research indicates that psychological well-being and pain are negatively correlated. On the other hand, optimism is positively correlated with pain outcomes and thus, improves quality of life in individuals with chronic illnesses. The study further stated that there is a substantial association between pain severity and optimism. Accepting their discomfort helps patients feel better psychologically and experience less severe pain (Hopper et al., 2016).
In contrast, happiness is described to be a long-term mental state that encompasses not just feelings of joy, satisfaction, and other pleasant emotions but also a sense that one's life is meaningful and useful (Lyubomirsky, 2001). Emotions, thoughts, and behaviors are connected to indicators that may indicate a reward. Moreover, these are intended to increase the likelihood of a reward and are guided by a behavioral activation system. Systematically focusing on hopeful or joyful memories activates the Behavioral Activation System (BAS) and reduces pain (Lefebvre & Jensen, 2019). Another study emphasized the presence of meaning in life and searching for meaning in life. Both of these affect resilience which ultimately affects mental well-being. They are linked with positive emotions that falls under the heading of happiness. Additionally, this study investigated how resilience influences individuals' mental well-being positively and directly (Rasheed et al., 2022).
Similarly, optimism may help prevent pain catastrophizing by encouraging a positive attitude towards the treatment of pain and its recovery. Optimistic people are more likely to use active coping mechanisms and have greater resilience which may help alleviate the negative effects of chronic pain. Happiness can boost resilience by promoting emotional well-being and lowering stress. High levels of psychological well-being may boost resilience by giving people a sense of purpose and meaning, even in a state of chronic pain. Individuals with high psychological well-being have greater emotional regulation and more adaptive responses to pain, which could help minimize pain catastrophizing (Acciari et al., 2019).
Broaden-and-Build Theory of Positive EmotionsPositive emotions have frequently been ignored in favor of more generic inclinations to approach or continue, to be crammed into models of emotions that are supposedly emotion-general, or to be confused with closely related affective states. Furthermore, positive emotions were not adequately represented by these methods. Hence, a different model for positive emotions was developed that more accurately depicts their special impacts. This is known as the "broaden-and-build theory of positive emotions". The theory suggests that experiencing pleasant emotions can increase people's short-term thought-action repertoires as well as their long-term personal resources (Fredrickson, 2001).
The broaden-and-build theory describes how positive emotions manifest as expanded thought-action repertoires and how they contribute to the development of durable human resources. In doing so, the hypothesis offers a fresh viewpoint on the adaptive value of happy emotions throughout evolution. Resultantly, our predecessors who gave in to the desires to play, explore, and other activities that are driven by happy emotions would have amassed more personal resources. Their higher personal resources would have translated into greater odds of surviving, and hence greater odds of living long enough to reproduce, when these same ancestors confronted inevitable hazards to life and limb later on (Fredrickson, 2004).
Biopsychosocial ModelIn 1977, George Engel introduced the biopsychosocial model, which argues that understanding a person's medical status requires considering psychological and social components in addition to biological aspects (Engel 1977; as cited in Gatchel et al., 2007). Chronic pain is commonly treated using this paradigm, which maintains that pain is a psychophysiological behavioral pattern that cannot be exclusively linked to biological, psychological, or social factors. It is proposed that psychological treatment be incorporated into physiotherapy to address all the factors that contribute to the experience of chronic pain (Miaskowski et al., 2019). It has been demonstrated that positive psychological constructs, such as optimism play a significant role in biopsychosocial models that predict how people would cope with both acute and chronic pain episodes. According to studies, those who accept their pain better over time actually have a tendency to report far less pain and pain-related disability (McCracken et al., 2007). Similarly, a meta-analysis by White et al. (2024) found a moderate negative relationship between chronic pain acceptance and pain-related impairment. This emphasizes the clinical importance of acceptance-based interventions to improve functional outcomes for patients of chronic pain.
Pain catastrophizing has been studied in the literature alongside numerous positive psychological constructs, such as optimism and positive emotions. Similarly, resilience has been studied using different constructs to see if it has any effect on psychological well-being, psychological distress, and pain catastrophizing. This investigation unearthed a negative association between resilience and psychological distress. Similarly, there is an inverse relationship between optimism and psychological distress (Yaseen et al., 2022). To assess their current emotional state, resilient people pay more attention inward and have a better understanding of emotions. Resultantly, they may try to increase their own good affect in order to lessen the emotional influence that their present discomfort has over them. They might show an optimistic perspective on life, a stronger conviction that life has purpose, and a readiness to endure pain and its aftereffects (Nwankwo et al., 2021).
The study of Sabouripour et al. (2021) indicated that resilient people use tactics that create positive feelings, such as benefit finding and positive reappraisal. Several studies revealed significant gender differences in pain catastrophizing which stated that women tend to score higher on pain catastrophizing than men. Moreover, they also stated that the income of the family plays a significant role in pain catastrophizing which revealed that those whose income was recorded as high had scored low on pain catastrophizing and vice versa (Ong et al., 2010). Possible gender variations in pain catastrophizing were identified in the investigation conducted by Lee et al. (2024). It was demonstrated that women tend to catastrophize pain more than men do. Moreover, their findings indicated that in both men and women, the likelihood of chronic pain was boosted by pain catastrophizing. The results, which showed that women tend to catastrophize more, were in line with earlier research. According to these investigations, women reported more catastrophic thinking in both chronic pain sufferers and healthy individuals (Forsythe et al., 2011). However, no significant differences of gender on resilience and pain catastrophizing were identified (Slepian & France, 2017).
Furthermore, a study's findings demonstrated statistically significant variations in pain severity and pain catastrophizing between employed and unemployed individuals (Núñez-Cortés et al., 2023). In addition to this, Acciari et al. (2019) identified that resilience and psychological well-being have a direct link, resilient people can generally retain their bodily and psychological health, as well as the ability to recover from traumatic experiences more rapidly. There is evidence that resilience can help improve psychological well-being. Reports from young people and healthcare staff revealed the need to sustain resilience during the pandemic to protect an individual's mental, emotional, and psychological health (Croghan et al., 2021). One significant element that lowers the quality of life and negatively impacts well-being is chronic pain. The findings of the study suggested that pain degrades the quality of life which has a negative impact on psychological well-being of an individual. Taking this into account, efficient pain management techniques may improve well-being and quality of life by enabling people to continue with their everyday activities. Simultaneously, nursing interventions should focus to improve pain management and offer patients additional support in order to effectively manage their pain (Topcu, 2018).
In contrast, the relationship between resilience and pain catastrophizing discovered that participants who scored higher on resilience evaluated lower on pain catastrophizing. This indicated that both domains are adversely connected. This same study also found that psychological resilience boosts positive emotions, which predicts a decrease in pain catastrophizing. However, it was not investigated which distinct positive emotions play how much of a role in enhancing resiliency on an individual basis (Ong et al., 2010). Furthermore, studies on people with major depressive disorder determined that catastrophic thinking is a substantial contributor to occupational impairment. The study discovered that reducing catastrophic thinking predicted a successful return to work, emphasizing the importance of cognitive factors on job status (Sullivan et al., 2011).
It is evident that, in both age groups, females exhibit greater resilience-related qualities than males. The findings corroborate those of another study which discovered that males had comparatively lower resilience than their female counterparts (Hidayat et al., 2022). According to (Lundman et al., 2007), the results also showed that resilience rises with age in both males and females. Resilient qualities may be more common in self-dependent individuals. An individual with a hardwired optimism and positive outlook could naturally be more resilient than others (Behera et al., 2020). Furthermore, McCarthy et al. (2020) found that those with chronic pain self-perceived an increase in pain severity when compared to the period before the UK's most severe lockdown (mid-April to early-May 2020). They reported higher levels of self-perceived increase in anxiety and sadness along with higher levels of loneliness and lower levels of physical activity when compared to individuals without pain. Reduced activity and pain catastrophizing are two crucial elements of the fear-avoidance paradigm of chronic pain. In this way, pain catastrophizing encourages behavioral reactions that worsen pain and other symptoms in people with chronic pain, ultimately lowering their quality of life (Crombez et al., 2012).
Moreover, literature shows that resilience has a significant relationship with pain catastrophizing. This identified that the more the individual catastrophizes about the pain the less resilient that individual is. However, no such research has been conducted yet that measures all these study constructs at one time. Similarly, many chronic pain survivors have been observed who catastrophize more about their pain which ultimately leads towards many psychological issues and stress. Therefore, determining the effect of catastrophizing is very important as it would empower the chronic pain survivors to work on their psychological health and enhance their well-being. This, in turn, would help them avoid catastrophize and use this energy more positively.
Research ObjectivesThe current study aimed to address the following research objectives:
- To investigate the relationship among resilience, optimism, happiness, psychological well-being, and pain catastrophizing among chronic pain survivors.
- To determine the moderating effects of optimism, happiness, and psychological well-being on resilience and pain catastrophizing among chronic pain survivors.
- To find gender differences in resilience and pain catastrophizing.
- To determine the differences in resilience and pain catastrophizing between working and non-working individuals.
- Resilience, optimism, happiness, and psychological well-being would be inversely related to pain catastrophizing among chronic pain survivors.
- Optimism, happiness, and psychological well-being would moderate the relationship between resilience and pain catastrophizing among chronic pain survivors.
- Women would tend to score higher on pain catastrophizing and resilience than men.
- Working individuals would score lower on pain catastrophizing than non-working individuals.
Method
Research DesignTo conduct this study, the researcher employed a cross-sectional correlation research design.
SampleThe current study used purposive sampling to collect the data. The Raosoft sample size calculator was used to calculate the sample size. The entire sample size was calculated to be 375 by putting the total population unknown and the confidence interval as 95%. As a result, data was collected from 375 individuals across different hospitals in Abbottabad and Swabi to conduct this study. Moreover, permission for data collection was granted from every hospital and the data was obtained from OPDs of every hospital. Participants were approached at the hospitals in OPD where they came for checkups regarding their pain. The researcher provided in-depth instructions to them as well as they were assured of confidentiality regarding their privacy. Moreover, they were informed that participation in the study is voluntary, and they can withdraw from the study anytime.
Inclusion CriteriaOnly those individuals were included in the study who faced chronic pain at any stage of their lives.
Exclusion CriteriaThere were no age or gender restrictions in the study. However, individuals who never faced chronic pain in their lives were not included in the study.
Table 1
Frequency Distribution of Demographic Variables (N = 375)
|
Variables |
f |
% |
M |
SD |
|---|---|---|---|---|
|
Age |
|
|
23.86 |
5.67 |
|
16 to 31 |
336 |
90 |
|
|
|
32 to 47 |
39 |
10 |
|
|
|
Gender |
|
|
|
|
|
Male |
152 |
29 |
|
|
|
Female |
223 |
71 |
|
|
|
Family Monthly Income |
|
|
|
|
|
10k to 100k |
254 |
67 |
|
|
|
100k to 200k |
84 |
22 |
|
|
|
Above 200k |
41 |
11 |
|
|
Table 1 indicates that there were a large number of females as compared to males. Furthermore, majority of the participants were fall between 16 to 31 years of age. Moreover, 154 participants were recorded as employed, while the remaining 221 were unemployed. The monthly income of a large number of study participants were between the range of 10k to 100k.
InstrumentsThe following instruments were used for data collection in this research. All the scales were used in the study after the permission of the respective authors.
Brief Resilience Scale (BRS)This scale was used to assess participants' resilience. This was developed by Smith et al. (2008) which consists of total 6 questions, of which 3 are positively written and 2 are reverse-coded. It is a 5-point Likert scale with responses ranging from strongly disagree to disagree, neutral to agree, and strongly agree. Strongly disagree would be scored as 1 and strongly agree as 5. Its scoring is that all the responses are added and then divided by the number of questions answered by that participant. The observed alpha reliability for the scale is given below in Table 2.
Pain Catastrophizing Scale (PCS)Pain catastrophizing influences how people perceive pain. According to Sullivan et al. (1995), those who catastrophize perform 3 actions, all of which are assessed by this questionnaire. These 3 actions are ruminating about the pain, magnifying the pain, and feeling helpless to manage their pain. In comparison to additional methods of assessing pain-associated thoughts, this scale is unusual in that it does not need the respondent to be in pain at the time of completion.
This scale has a total of 13 items with responses ranging from 0 to 4. Zero means not at all and 4 means all the time. Item scores are added together to form a total score (PCS-T) and three subscale scores. PCS-R Rumination: Items 8, 9, 10, and 11. PCS-M Magnification: Items 6, 7, 13, PCS-H (Helplessness): Items 1, 2, 3, 4, 5, and 12. Higher score on pain catastrophizing interprets that the individual is catastrophizing more about his/her pain.
Subjective Happiness Scale (SHS)This scale was amplified by Lyubomirsky and Lepper (1999). It measures the subjective happiness of an individual and is also known as a general happiness scale. A 4-item questionnaire is operated to rate subjective happiness. Each item is finished by choosing one of 7 possibilities that complete a specific sentence fragment. Item 4 is a reverse scoring item. The reliability of the scale was observed as .71 as given in Table 2.
Psychological Well-being ScaleThis scale was developed by Ryff (1995). The revised version of the scale that is often used now has 18 items divided into 6 subscales. Autonomy (items 15, 17, and 18), environmental mastery (items 4, 8, and 9), personal growth (items 11, 12, and 14), positive relations (items 6, 13, and 16), life purpose (items 3, 7, and 10) and self-acceptance (items 1,2, and 5) are the six subscales. Item numbers 1, 2, 3, 8, 9, 11, 12, 13, 17, and 18 are reverse coded. This is a 7-point Likert scale, with 1 being strongly disagree, and 7 being strongly agree.
Life Orientation Test-revised ScaleLife orientation test-revised scale is applied to assess optimism in an individual. This scale was developed by Scheier et al. (1994). The revised form of the scale that is often used now has ten items divided into three subscales. However, the main scale created in 1992 has a total of 10 items. Optimism (items 1, 4, and 10), pessimism (items 3, 7, and 9), and fillers (items 2, 5, 6, and 8) are the subscales. Items 3, 7, and 9 are reverse coded. This is a 5-point Likert scale, with 0 equals strongly disagree, and 4 equals strongly agree. Cronbach's alpha of this questionnaire was calculated as .74.
Table 2
Psychometric Properties, Alpha Reliability of PCS, BRS, HAP, OPT, and PWB Scales (N = 375)
|
Scale |
k |
a |
M(SD) |
Range |
|
|---|---|---|---|---|---|
|
Min |
Max |
||||
|
PCS |
13 |
.92 |
16.90(12.15) |
02 |
43 |
|
BRS |
06 |
.73 |
17.95(4.63) |
07 |
29 |
|
HAP |
04 |
.71 |
16.76(5.23) |
04 |
26 |
|
OPT |
06 |
.74 |
13.26(4.38) |
03 |
21 |
|
PWB |
18 |
.71 |
83.61(13.19) |
39 |
117 |
Note. BRS = Brief Resilience Scale, HAP = Happiness, OPT = Optimism, PWB = Psychological Well-Being.
Results
The Cronbach's alpha value and psychometric properties of each scale were ascertained in the first phase, and these were deemed to be extremely good for all the measures. Following this, the frequency distribution was examined to ensure that the data on all scales was normally distributed and prepared for the administration of all parametric tests. Additionally, Pearson's moment correlation was used to examine the correlations between the continuous variables, and it was discovered to be significant for nearly all the variables.
As genders had two groups, an independent t-test was used to examine the effects of each on pain catastrophizing and resilience. Similarly, independent sample t-test was used to determine differences in work status on pain catastrophizing since there were two groups of participants in the working state, that is, employed and unemployed. Multiple moderation was employed to determine the moderating influence of psychological well-being, optimism, and happiness on resilience and pain catastrophizing.
Table 3
Pearson Correlation among PCS, BRS, HAP, OPT, and PWB (N = 375)
|
Measures |
M |
SD |
1 |
2 |
3 |
4 |
5 |
|---|---|---|---|---|---|---|---|
|
1.PCS |
15.66 |
12.96 |
1 |
|
|
|
|
|
2.BRS |
17.70 |
4.70 |
-.59** |
1 |
|
|
|
|
3.OPT |
13.25 |
4.38 |
-.57** |
.70** |
1 |
|
|
|
4.HAP |
16.78 |
5.20 |
-.63** |
.51** |
.48** |
1 |
|
|
PWB |
83.61 |
12.63 |
-.42** |
.42** |
.33** |
.47** |
1 |
Note. PCS = Pain Catastrophizing Scale, BRS = Brief Resilience Scale, HAP = Happiness, OPT = Optimism, PWB = Psychological Well-Being, ** means the correlations are significant at .01 level.
The relationships between pain catastrophizing, resilience, optimism, happiness, and psychological well-being are illustrated in Table 3. As hypothesized in hypothesis 1, there would be an inverse relationship between these variables and pain catastrophizing. The results determined a significant relationship between these variables at .01 level (r = -.59, -.57, -.63, -.42, p < .01).
Furthermore, the researcher's prediction that positive variables, such as resilience, psychological well-being, optimism, and happiness would be positively correlated with one another was confirmed in this study, as all of these variables were found to be positively correlated at the .01 significant level.
Table 4
Moderation of Optimism, Happiness, and Psychological Well-being on Resilience and Pain Catastrophizing (N = 375)
|
|
Model 1 |
Model 2 |
||||
|---|---|---|---|---|---|---|
|
Measures |
B |
b |
SE |
B |
b |
SE |
|
Constant |
16.91** |
|
.43 |
16.43** |
|
.49 |
|
Optimism |
-0.58** |
-.21** |
.14 |
-0.51** |
-.18** |
.15 |
|
Happiness |
-0.88** |
-.38** |
.10 |
-0.87** |
-.37** |
.10 |
|
Psychological Well-being |
-0.09* |
-.09* |
.03 |
-0.09** |
-.10** |
.03 |
|
Resilience |
-0.53** |
-.20** |
.14 |
-0.48** |
-.18** |
.14 |
|
Optimism x Resilience |
|
|
|
0.04** |
.11** |
.01 |
|
Happiness x Resilience |
|
|
|
-0.02 |
-.05 |
.02 |
|
Psychological Well-being x Resilience |
|
|
0.00 |
-.03 |
.00 |
|
|
R2 |
.52** |
|
|
0.53** |
|
|
|
DR2 |
|
|
|
0.008 |
|
|
The moderation of psychological well-being, happiness, and optimism between resilience and pain catastrophizing is displayed in Table 4. The predictors in model 1 were able to explain 52% of the variations in the outcome, as indicated by the R2 value of .52 [F (4, 370) = 100.01, p < .01]. The results indicated that optimism, happiness, psychological well-being, and resilience (B = -.58, p < .01), (B = -.88, p < .01), (B = -.09, p < .01), and (B = -.53, p < .01) negatively moderated the pain catastrophizing significantly.
The variables in model 2 explained 53% of the variations in the outcome, as indicated by the value of R2 .53 [F (7, 367) = 58.55, p < .01]. According to the results, psychological well-being, optimism, happiness, and resilience (B = -.09, p < .05), (B = -.51, p < .01), (B = -.87, p < .01), and (B = -.48, p < .01) negatively predicted pain catastrophizing significantly.
Similarly, optimism x resilience positively predicted pain catastrophizing (B = .04, p < .01), while happiness x resilience and psychological well-being x resilience did not significantly predict pain catastrophizing (B = -.02, p > .05), (B = -.00, p > .05). The DR2 value .008 showed .8% change in variation model 1 and 2 with DF (3, 367) = 2.09, p > .05.
Figure 1
Moderation Graph Between Optimism and Resilience
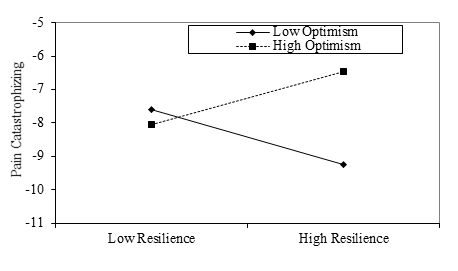
Figure 2
Moderation Graph Between Psychological Well-being and Resilience
Table 5
Gender Differences on Resilience and Pain Catastrophizing (N = 375)
|
Variable |
Male |
Female |
t(373) |
p |
Cohen's d |
|---|---|---|---|---|---|
|
M(SD) |
M(SD) |
||||
|
Resilience |
17.76(4.71) |
18.07(4.58) |
0.62 |
.53 |
|
|
PCS |
15.11(11.76) |
18.13(12.28) |
2.39 |
.01 |
0.25 |
Note. PCS = Pain Catastrophizing Scale
The mean score of females on resilience (M = 18.07, SD = 4.58) is greater than that of males (M = 17.76 SD = 4.71), in line to an independent sample t-test [t (373) = .62 p > .05]. However, the p value is greater than .05 which means that the differences are non-significant.
Moreover, the mean score of females on pain catastrophizing (M = 18.13, SD = 12.28) is greater than that of males (M = 15.11, SD = 11.76), in line to an independent sample t-test [t (373) = 2.39 p < .05]. The results demonstrated that significant gender differences exist on pain catastrophizing and females scored higher than males.
Table 6
Differences on Pain Catastrophizing between Working and Non-working Participants (N = 375)
|
|
Working |
Non-Working |
t(373) |
p |
Cohen's d |
|---|---|---|---|---|---|
|
Measure |
M(SD) |
M(SD) |
|||
|
PCS |
14.24(10.11) |
18.76(13.09) |
3.60 |
.00 |
0.38 |
Note. PCS = Pain Catastrophizing Scale
Table 6 indicates significant differences among two different groups on scores of pain catastrophizing with the value of t (373) = 3.60 and p-value is = .00. Hence, the analysis concluded that the differences between working and non-working participants on pain catastrophizing are significant and non-working participants scored higher than working participants.
Discussion
This study focused on the relationship between optimism, happiness, psychological well-being, resilience, and pain catastrophizing among patients of chronic pain. One of the main goals of this study was to examine the moderating effects of optimism, happiness and psychological well-being on resilience and pain catastrophizing among patients of chronic pain. Similarly, the study also investigated gender differences between working and non-working individuals on pain catastrophizing.
To determine the correlation between optimism, happiness, psychological well-being, resilience, and pain catastrophizing, bivariate correlations was run down. The results of the correlation supported the first hypothesis of the study. Resilience, optimism, happiness, and psychological well-being were analyzed to be significantly correlated to each other positively (See Table 4). These results aligned with the findings that the more resilient and happier an individual is, the more psychological well-being of that individual would be (Acciari et al., 2019: Yaseen et al., 2022).
Moreover, this analysis also identified a significant negative correlation of resilience, optimism, happiness, and psychological well-being with pain catastrophizing (Table 4). These results were relevant to the hypothesis as researcher in accordance with the literature predicted a negative significant correlation among these variables. Study of France et al. (2020) showed a negative association of resilience and pain catastrophizing. This concluded that the findings of the current study on resilience and pain catastrophizing are aligned with the previous literature.
Similarly, another study disclosed that pain catastrophizing is directly associated with negative constructs, such as loneliness and sadness and indirectly associated with positive constructs, for instance happiness (Boyette-Davis, 2023). It was also concluded that the more individuals catastrophize their pain the less resilient they were (Ong et al., 2010). The current study discovered a similar type of association of pain catastrophizing with positive constructs and explained that pain catastrophizing is negatively associated with resilience, optimism, happiness, and psychological well-being among chronic pain survivors (Table 4).
Moreover, to explain Table 4 in detail, moderation effect of optimism, happiness, and psychological well-being on resilience and pain catastrophizing was explored. It was concluded that optimism, happiness, psychological well-being, and resilience significantly moderated pain catastrophizing negatively. The overall results identified that optimism, happiness, and psychological well-being cause 52% of significant variations in resilience and pain catastrophizing (Table 5).
In addition to this, table also yielded the interaction effects of optimism and resilience, happiness and resilience, psychological well-being and resilience with the coefficients, respectively. The overall model concluded .8% of significant variations in pain catastrophizing (Table 5). By comparing the findings in literature, it was explained that optimism as a moderator predicts resilience in individuals. Resultantly, optimism boosts resilience which ultimately decreases the catastrophizing level of pain in patients. It was also discovered that optimistic individuals tend to provide less attention to their pain which helps them use energy in a more positive way rather than just ruminating about their pain (Buckingham & Richardson, 2020).
Additionally, resilience and psychological well-being were found to be significantly correlated with each other which effects the pain catastrophizing level of individuals (Acciari et al., 2019). The study of Sabouripour et al. (2021) indicated that resilient people use tactics that create positive feelings, such as benefit finding and positive reappraisal. As a result of these tactics and their more resilience, they opted better ways to cope with their pain rather than catastrophizing it.
Furthermore, the researcher predicted that significant gender differences would exist on both resilience and pain catastrophizing. Additionally, in the light of literature, it was stated that women would score high on resilience as well as pain catastrophizing. It was concluded that women scored higher on pain catastrophizing than men and these differences were significant as the p-value was less than .05. In contrast, no significant differences existed between men and women on resilience as the p-value was concluded to be greater than .05 (Table 6). Gender differences on resilience and pain catastrophizing were contradictory in literature since it was disclosed that women exhibit greater resilience-related qualities than men. The findings corroborate those of another study which discovered that males had comparatively lower resilience than their female counterparts (Hidayat et al., 2022). However, in a meta-analysis, Gök and Koğar (2021) discovered that men reported higher levels of psychological resilience than women.
In opposite, no significant differences were identified on both resilience and pain catastrophizing. This is because it was stated that both women and men tend to catastrophize equally about their pain although, their ways of catastrophizing are different (Slepian & france, 2017). The findings of Hidayat et al. (2022) discovered that males had comparatively lower resilience than their female counterparts. It was evident that women exhibit greater resilience-related qualities than men. In this study, women scored high on pain catastrophizing and significant differences were extracted between men and women on pain catastrophizing, while no significant differences were concluded on resilience. Additionally, the study of Lee et al. (2024) demonstrated that women tend to catastrophize more about their pain than men. The current study proved these findings among patients of chronic pain.
Similarly, another goal of this study was to investigate significant differences of work status on pain catastrophizing. It was concluded that unemployed individuals scored significantly higher than the employed ones (Table 7). The researcher in accordance with literature predicted that unemployed individuals have more free time and they do not utilize it to their full potential. As a result, they tend to overthink and ruminate more. Moreover, when they face any uncertainty, such as stress or pain, they find themselves in more trouble and start worrying more. These findings are aligned with the study which demonstrated statistically significant variations in pain severity and pain catastrophizing between employed and unemployed individuals (Núñez-Cortés et al., 2023).
The findings are in accordance with the literature that explains the moderation effect of optimism, happiness, and psychological well-being on resilience and pain catastrophizing among the patients of chronic pain in Pakistani culture and context. The current study provided a handful insight to the practitioners and patients that catastrophizing degrades the overall mental health in many ways which affects the psychological and physical health later. Therefore, to enhance the mental well-being and health, it is important for a patient suffering from chronic pain to work on their optimism and resilience.
ConclusionThe current study concluded that optimism, happiness, psychological well-being, and resilience are positively correlated with each other among chronic pain patients. This provides a thorough understanding to the patients that to overcome the consequences of chronic pain they should attend resilience-building programs and enhance their psychological well-being by using their energy in effective ways unlike catastrophizing. This would decrease the overall effects of pain.
Implications- The current study concluded that optimism, resilience, happiness, and psychological well-being significantly decrease the pain in chronic pain survivors. Therefore, interventions are required to help people with chronic pain improve their coping mechanisms which may be benefited from an understanding of these relationships. For instance, therapeutic techniques could focus on cultivating optimism and resilience building programs in health centres. This is because optimism and resilience considerably lessen pain catastrophizing which encourages patients to face it more competently.
- In the context of chronic pain, it is helpful to explain how positive psychological constructs, such as optimism, happiness, and psychological well-being interact with one another and affect health outcomes. This is clear that pain do persists and sometimes its complete termination is not possible. However, being more optimistic and resilient the challenges caused by pain decrease to a significant level and the overall well-being and quality of life can be improved.
- A cross sectional research design was employed to conduct this study which does not reveal the causal effects. Similarly, a longitudinal experimental research design conducting on same participants across different span of time would strengthen the findings.
- The study examined the relationships and moderation effect of certain variables. However, the study did not develop an intervention to handle the chronic pain.
Conflict of Interest
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study is not available due to ethical, legal, or commercial restrictions.
Funding Details
No funding has been received for this research.
REFERENCES
Acciari, A. S., Leal, R. F., Coy, C. S. R., Dias, C. C., & Ayrizono, Maria de Lourdes, S. A. (2019). Relationship among psychological well-being, resilience and coping with social and clinical features in Crohn’s disease patients. Arquivos de Gastroenterologia, 56(2), 131–140. https://doi.org/10.1590/s0004-2803.201900000-27
Afrashteh, M., Abbasi, M., & Abbasi, M. (2023). The relationship between meaning of life, perceived social support, spiritual well-being and pain catastrophizing with quality of life in migraine patients: The mediating role of pain self-efficacy. BMC Psychology, 11(1), Article e17. https://doi.org/10.1186/s40359-023-01053-1
Alschuler, K. N., Jensen, M. P., Sullivan-Singh, S. J., Borson, S., Smith, A. E., & Molton, I. R. (2013). The association of age, pain, and fatigue with physical functioning and depressive symptoms in persons with spinal cord injury. The Journal of Spinal Cord Medicine, 36(5), 483–491. https://doi.org/10.1179/2045772312y.0000000072
Behera, R. R., Mohapatra, M., Maity, C. K., Bera, R., Panda, D., Panda, D., Karthik, R., & Borkataki, S. (2020). Gender difference in resilience among the students of IIT Kharagpur. Indian Journal of Positive Psychology, 11(2), 146–148.
Boselie, J. J. L. M., & Peters, M. L. (2023). Shifting the perspective: How positive thinking can help diminish the negative effects of pain. Scandinavian Journal of Pain, 23(3), 452–463. https://doi.org/10.1515/sjpain-2022-0129
Boyette-Davis, J. (2023). Pain catastrophizing is associated with a pattern of negative emotional states and a lack of positive emotional priming. The American Journal of Psychology, 136(1), 103–114. https://doi.org/10.5406/19398298.136.1.08
Buckingham, A., & Richardson, E. J. (2020). The relationship between psychological resilience and pain threshold and tolerance: Optimism and grit as moderators. Journal of Clinical Psychology in Medical Settings, 28(3), 518–528. https://doi.org/10.1007/s10880-020-09731-7
Croghan, I. T., Chesak, S. S., Adusumalli, J., Fischer, K. M., Beck, E. W., Patel, S. R., Ghosh, K., Schroeder, D. R., & Bhagra, A. (2021). Stress, resilience, and coping of healthcare workers during the COVID-19 pandemic. Journal of Primary Care & Community Health, 12, 215013272110084. https://doi.org/10.1177/21501327211008448
Crombez, G., Eccleston, C., Van Damme, S., Vlaeyen, J. W. S., & Karoly, P. (2012). Fear-avoidance model of chronic pain. The Clinical Journal of Pain, 28(6), 475–483. https://doi.org/10.1097/ajp.0b013e3182385392
Flink, I. K., Smeets, E., Bergboma, S., & Peters, M. L. (2015). Happy despite pain: Pilot study of a positive psychology intervention for patients with chronic pain. Scandinavian Journal of Pain, 7(1), 71–79. https://doi.org/10.1016/j.sjpain.2015.01.005
Forsythe, L. P., Thorn, B., Day, M., & Shelby, G. (2011). Race and sex differences in primary appraisals, catastrophizing, and experimental pain outcomes. The Journal of Pain, 12(5), 563–572. https://doi.org/10.1016/j.jpain.2010.11.003
Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. American Psychologist, 56(3), 218–226. https://doi.org/10.1037/0003-066x.56.3.218
Fredrickson, B. L. (2004). The broaden–and–build theory of positive emotions. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences, 359(1449), 1367–1377. https://doi.org/10.1098/rstb.2004.1512
Furrer, A., Michel, G., Terrill, A. L., Jensen, M. P., & Müller, R. (2017). Modeling subjective well-being in individuals with chronic pain and a physical disability: The role of pain control and pain catastrophizing. Disability and Rehabilitation, 41(5), 498–507. https://doi.org/10.1080/09638288.2017.1390614
Gatchel, R. J., Peng, Y. B., Peters, M. L., Fuchs, P. N., & Turk, D. C. (2007). The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychological Bulletin, 133(4), 581–624. https://doi.org/10.1037/0033-2909.133.4.581
Gök, A., & Koğar, E. Y. (2021). A meta-analysis study on gender differences in psychological resilience levels. Turkish Cypriot Journal of Psychiatry and Psychology, 3(2), 132–143.
Hidayat, U., Hidayat, N., Rehman, S., & Ullah, Z. (2022). Emotional distress, resilience and mental well-being among TB patients in Peshawar. Pakistan Journal of Chest Medicine, 28(1), 38–44.
Hopper, M. J., Curtis, S., Hodge, S., & Simm, R. (2016). A qualitative study exploring the effects of attending a community pain service choir on wellbeing in people who experience chronic pain. British Journal of Pain, 10(3), 124–134. https://doi.org/10.1177/2049463716638368
Khan, M. N. U., Morrison, N. M., & Marshall, P. W. (2020). The role of fear-avoidance beliefs on low back pain-related disability in a developing socioeconomic and conservative culture: A cross-sectional study of a Pakistani population. Journal of Pain Research, 13, 2377–2387. https://doi.org/10.2147/JPR.S258314
Lee, C., Kwoh, K., Park, J., Park, L., & Ahn, H. (2024). Racial disparities in pain between Non-Hispanic Whites and Asian Americans with knee osteoarthritis: The role of pain catastrophizing. Research Square. https://doi.org/10.21203/rs.3.rs-5228306/v1
Lefebvre, J. C., & Jensen, M. P. (2019). The relationships between worry, happiness and pain catastrophizing in the experience of acute pain. European Journal of Pain. https://doi.org/10.1002/ejp.1405
Lundman, B., Strandberg, G., Eisemann, M., Gustafson, Y., & Brulin, C. (2007). Psychometric properties of the Swedish version of the Resilience Scale. Scandinavian Journal of Caring Sciences, 21(2), 229–237. https://doi.org/10.1111/j.1471-6712.2007.00461.x
Lyubomirsky, S. (2001). Why are some people happier than others? The role of cognitive and motivational processes in well-being. American Psychologist, 56(3), 239–249. https://doi.org/10.1037/0003-066x.56.3.239
Lyubomirsky, S., & Lepper, H. S. (1999). A measure of subjective happiness: Preliminary reliability and construct validation. Social Indicators Research, 46(2), 137–155. https://doi.org/10.1023/a:1006824100041
McCarthy, H., Potts, H., & Fisher, A. (2020). Physical activity behaviour before, during and after COVID-19 restrictions: A longitudinal smartphone tracking study of 5395 UK adults. (Preprint). Journal of Medical Internet Research, 23(2). https://doi.org/10.2196/23701
McCracken, L. M., MacKichan, F., & Eccleston, C. (2007). Contextual cognitive-behavioral therapy for severely disabled chronic pain sufferers: Effectiveness and clinically significant change. European Journal of Pain, 11(3), 314–322. https://doi.org/10.1016/j.ejpain.2006.05.004
Miaskowski, C., Blyth, F., Nicosia, F., Haan, M., Keefe, F., Smith, A., & Ritchie, C. (2019). A biopsychosocial model of chronic pain for older adults. Pain Medicine, 21(9), 1793–1805. https://doi.org/10.1093/pm/pnz329
Núñez-Cortés, R., Cruz-Montecinos, C., Torreblanca-Vargas, S., Tapia, C., Gutiérrez-Jiménez, M., Torres-Gangas, P., Calatayud, J., & Pérez-Alenda, S. (2023). Effectiveness of adding pain neuroscience education to telerehabilitation in patients with carpal tunnel syndrome: A randomized controlled trial. Musculoskeletal Science and Practice, 67, Article e102835.
Nwankwo, V. C., Jiranek, W. A., Green, C. L., Allen, K. D., George, S. Z., & Bettger, J. P. (2021). Resilience and pain catastrophizing among patients with total knee arthroplasty: A cohort study to examine psychological constructs as predictors of post-operative outcomes. Health and Quality of Life Outcomes, 19(1), Article e136. https://doi.org/10.1186/s12955-021-01772-2
Ong, A. D., Zautra, A. J., & Reid, M. C. (2010). Psychological resilience predicts decreases in pain catastrophizing through positive emotions. Psychology and Aging, 25(3), 516–523. https://doi.org/10.1037/a0019384
Rasheed, N., Fatima, I., & Tariq, O. (2022). University students’ mental well-being during COVID-19 pandemic: The mediating role of resilience between meaning in life and mental well-being. Acta Psychologica, 227, Article e103618. https://doi.org/10.1016/j.actpsy.2022.103618
Ryff, C. D., & Keyes, C. L. M. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69(4), 719–727. https://doi.org/10.1037/0022-3514.69.4.719
Sabouripour, F., Roslan, S., Ghiami, Z., & Memon, M. A. (2021). Mediating role of self-efficacy in the relationship between optimism, psychological well-being, and resilience among Iranian students. Frontiers in Psychology, 12, Article e675645. https://doi.org/10.3389/fpsyg.2021.675645
Scheier, M. F., Carver, C. S., & Bridges, M. W. (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the life orientation test. Journal of Personality and Social Psychology, 67(6), 1063–1078. https://doi.org/10.1037/0022-3514.67.6.1063
Slepian, P. M., & France, C. R. (2017). The effect of resilience on task persistence and performance during repeated exposure to heat pain. Journal of Behavioral Medicine, 40(6), 894–901. https://doi.org/10.1007/s10865-017-9854-y
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15(3), 194–200. https://doi.org/10.1080/10705500802222972
Sullivan, M. J. L., Bishop, S. R., & Pivik, J. (1995). The pain catastrophizing scale: Development and validation. Psychological Assessment, 7(4), 524–532. https://doi.org/10.1037/1040-3590.7.4.524
Sullivan, M. J. L., Adams, H., Martel, M.-O., Scott, W., & Wideman, T. (2011). Catastrophizing and perceived injustice. Spine, 36(25Suppl), 244–249. https://doi.org/10.1097/brs.0b013e3182387fed
Topcu, S. Y. (2018). Relations among pain, pain beliefs, and psychological well-being in patients with chronic pain. Pain Management Nursing, 19(6), 637–644. https://doi.org/10.1016/j.pmn.2018.07.007
Trompetter, H. R., Bohlmeijer, E. T., Lamers, S. M. A., & Schreurs, K. M. G. (2016). Positive psychological well-being is required for online self-help acceptance and commitment therapy for chronic pain to be effective. Frontiers in Psychology, 7, Article e353. https://doi.org/10.3389/fpsyg.2016.00353
Voon, P., Karamouzian, M., & Kerr, T. (2017). Chronic pain and opioid misuse: A review of reviews. Substance Abuse Treatment, Prevention, and Policy, 12(1), Article e36. https://doi.org/10.1007/s10865-022-00347-w
White, K. M., Zale, E. L., Lape, E. C., & Ditre, J. W. (2024). The association between chronic pain acceptance and pain-related disability: A meta-analysis. Journal of Clinical Psychology in Medical Settings. Advance online publication. https://doi.org/10.1007/s10880-024-10061-1
Yaseen, F., Naeem, N., Jafri, S. K. A., & Jamal, Y. (2022). Optimism and psychological distress: The role of resilience as a moderator in COVID-19 recovered patients of Pakistan. Multicultural Education, 8(1), 241–248. https://doi.org/10.5281/zenodo.5940237