| Review | Open Access |
|---|
Family-Based Exposure and Response Prevention (ERP) for Purely Compulsive (Pure-C) OCD : A Case Study |
 |
|---|
![]() Momina Yahya1* and Sadaf Saleem2
Momina Yahya1* and Sadaf Saleem2
1Syed Babar Ali School of Science and Engineering, Lahore University of Management Sciences, Pakistan
2Punjab Institute of Mental Health, Lahore, Pakistan
Pure-C OCD is a new emerging domain of OCD, depicting purely compulsive behaviors in the absence of any obsession. This case study examines the efficacy of family-based exposure and response prevention (ERP) and solution-focused therapy (SFT) for a 19-year-old male with purely compulsive OCD, characterized by sensory-driven rituals (e.g., excessive handwashing, ritualized showering) without comorbid obsessions. Pre-treatment assessment revealed a Y-BOCS compulsion score of 15 (moderate severity), with compulsions supported by "not just right" sensations rather than fear-based obsessions. Key themes in the anxiety hierarchy were avoidance related to touching his body and using the washroom, ritualistic handwashing and showering, disruption in daily life activities, and avoidance of contact of body parts with each other during sleep. A diagnosis of F42.2. obsessive-compulsive disorder (OCD), with fair insight, was given. The patient’s childhood perfectionistic tendencies, age of onset, and familial history of compulsive traits served as predisposing factors. The first episode was precipitated by academic stress and hygiene-focused media coverage of COVID-19. Familial conflicts, enabling behavior of the family, and avoidance perpetuated the symptoms. However, fair insight, motivation, familial support, and moderate severity predicted a positive prognosis. Based on the symptoms and contributing factors, an eclectic approach was used, where high-intensity Family-based ERP was the primary intervention. It targeted six mini-anxiety hierarchies, each focusing on a specific theme. The solution-focused therapy (SFT) was then used to improve problem-solving skills related to academic stress and assertiveness training for familial conflicts. For long-term benefits, relapse prevention was applied. Overall treatment took 8 months, and a total of 95 sessions were conducted. It showed an average 80% improvement. The findings aligned with earlier literature and served as a guide for future research and therapists for dealing with Pure-C OCD. Limitations include long-term follow-up to assess the maintenance of achieved goals.
1. INTRODUCTION
Obsessive-compulsive disorder (OCD) affects 1.2 of % population in general and has a mean age of onset in adolescence (American Psychiatric Association [APA], 2022). Traditionally, it has been characterized as the presence of obsessions (i.e., unwanted, unpleasant, involuntary intrusive thoughts, urges, and images) and/or compulsions (i.e., repetitive behaviors or mental acts, as a result of obsessions, or aimed at reducing anxiety) (APA, 2022). Recent research has shown that OCD can exist in mutually exclusive (Pure Categories) of either obsessions or compulsions (Rodgers et al., 2015). Purely Compulsive (or Pure C) OCD is characterized by sensory-driven compulsive behavior (Summerfeldt, 2004), emerging from physical discomfort or “not just right” experiences (NJREs), manifested in the form of urges to perform certain behavior (Leckman et al., 1994; Miguel et al., 2000). The key difference between obsessional and compulsive urges is the fear-based, intrusive nature present in obsessional urges, which is absent in compulsive sensory-based urges. The focus of both urges is also different; compulsive sensory-driven urges focus on achieving a sense of completeness or ‘just right’ experience (Coles et al., 2003), while compulsions as a result of obsessional urges focus on reducing the chance of an imagined, feared event happening (Clark, 2019).
This is further explained by the Habit Hypothesis Theory of OCD, proposing that compulsions arise from “dysregulated goal-directed/habit systems”, which have neurobiological underpinnings. These compulsions, as a result, are “valence-independent habits”, persisting without obsession-related triggers (e.g., repetitive handwashing without the fear of contamination) (Gillan et al., 2011). Here, obsessions become a post-compulsion rationalization (e.g., to explain excessive handwashing, individuals may develop obsessional fears to justify compulsive behavior, creating a false belief that the behavior was driven by fear all along) (Gillan & Sahakian, 2014). This dual perspective, i.e., sensory-driven urges and habit dysfunction, makes compulsions the core feature of OCD, which challenges the traditional cognitive behavioral therapeutic (CBT) narrative.
Consequently, the traditional CBT treatment approach cannot work with Pure-C OCD. It highlights the need for more behavioral and problem-focused solutions (Yulish et al., 2017). Family-based ERP is the best-known behavioral treatment for compulsions. It is built on the principle of habituation and extinction, where repeated and prolonged exposure to triggers, without engaging in compulsion, eventually leads to a reduction in anxiety over time and breaks the cycle of OCD (Jacoby & Abramowitz, 2016). But whether it works with pure compulsions, in the absence of obsession, is still unknown. This case study combines family-based ERP to reduce compulsive behaviors and SFT to deal with the real-life stressors that worsen the symptoms of pure-c OCD.
Objectives- To evaluate the effectiveness of behavior-focused Family-based ERP in reducing compulsive and avoidance behaviors in pure-c OCD.
- To alleviate the contributing factors (e.g., academic stress, dealing with family conflicts, etc.) using SFT.
- Family-based ERP will lead to a significant reduction in compulsive and avoidance behaviors compared to baseline (pre-treatment phase).
- The SFT will reduce familial/academic stress and increase adaptive coping.
Method
Research DesignSingle-case A-B-A quasi-experimental research design was used to assess the effectiveness of an eclectic approach to treat the symptoms of pure-C OCD.
Operational DefinitionsObsessive-Compulsive Disorder (OCD)
OCD is a disorder explained by DSM-5-TR as the presence of either obsession, or compulsions, or both, which are time-consuming (i.e., take more than 1 hour a day), and cause significant distress in social or occupational areas of life (APA, 2022).
Pure CompulsionsPure Compulsion is explained by DSM-5-TR as, repetitive behavior or mental acts that are performed according to some rules that must be applied rigidly (APA, 2022).
Exposure and Response Prevention (ERP)The ERP was introduced by Meyer (1966). It involves prolonged exposure to triggers, without engaging in compulsion, which eventually leads to a reduction in anxiety over time and breaks the cycle of OCD (Jacoby & Abramowitz, 2016).
Solution-Focused Therapy (SFT)The SFT was first introduced by Watzlawick et al. (1974), and later formally developed by de Shazer and Berg (1997). It focuses on identifying previous solutions that have been tried and failed, finding maintenance factors, then trying out different solutions, and finally implementing those solutions that work for the client (Jerome et al., 2023).
SampleThe sample consisted of a single case (N=1).
Clinical PresentationThe patient was a 19-year-old male, the eldest of four siblings, enrolled in an engineering diploma, and had been an intelligent student throughout. The household environment was distant and conflict-prone. His father, a government employee, was anxious and aggressive, often reacting harshly to the patient’s behaviors. His mother, a stay-at-home parent, was more understanding but often scolded him. He relies heavily on her and his younger sisters for reassurance and in avoiding discomfort related to the experience of compulsions. He did not have any perinatal trauma. The patient described that from childhood he had always done things in a certain way, as it gave him a sense of pleasure (e.g., keep things arranged in a certain way, etc.). Some behaviors were even rewarded (e.g., arranging things back right after a minor disturbance). The majority of these behaviors either died down on their own or were replaced with some other behaviors. These behaviors gave him a sense of internal pleasure and did not cause any disturbance in his routine. His family history also included signs of anxious traits (e.g., grandmother’s excessive washing of clothes) but no diagnosed psychiatric conditions.
The current problematic symptoms date back to March 2020. Initially, the patient enjoyed making soap bubbles during hand washing, as it gave him a feeling of ‘pure cleanliness’. Later, it became a habit, which he could not get rid of, and it made him spend 15-20 minutes handwashing. During exams, he was under pressure to secure exceptional marks and was often scolded by his parents for wasting time. So, to save time, he restricted handwashing to the left hand only (as it was used for cleaning body). This led to the belief that his right hand was perpetually dirty. He had a rule that if something was dirty, it should not be touched and needed to be cleaned thrice, as per Islamic principles of cleanliness. So, he avoided touching anything or any body part with the right hand. After the exams, he engaged in excessive hand washing, following the Islamic principles (wudu and ghussal). However, he did not feel 100% clean, so he did wudu multiple times, resulting in spending 20 to 25 minutes for every hand washing session. This behavior continued for almost 7-8 months. Since he had multiple similar habits in the past that died down on their own, he believed that this would also change or cease to exist on its own.
However, during COVID-19 (December 2020), excessive media coverage heightened his fear of contamination, and he started doing the ablution (i.e., Islamic ways of cleaning, involving cleaning each part 3 times) every time he used the washroom. After each ablution, he waited and noticed whether he felt clean enough or not. Mostly, he did not feel clean enough by doing it once, resulting in him doing it again and spending almost 30 minutes. This led to physical fatigue. Although no formal treatment option was sought but the parents tried to restrict these behaviors by restricting the water, but it only increased familial conflicts. During this episode, no intrusive thoughts were reported to initiate compulsive behavior. Instead, the patient reported an internal sensation of incompleteness, which could only be satisfied if he felt ‘clean enough’; if not satisfied, a physical discomfort was experienced.
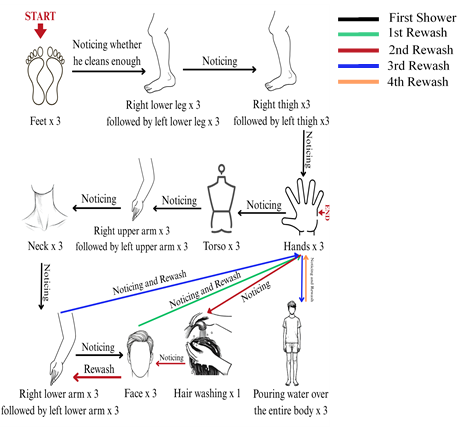
In April 2021, water splashed on the patient’s body from a broken washroom pipe, leading to an instant compulsive shower (consisting of multiple ghussal, as he still felt dirty after the first ghussal), lasting 90 minutes. Over time, he avoided the washroom entirely, except when absolutely necessary, which then triggered excessive hand and body washing rituals, leaving him physically drained. He also began to follow an elaborate, time-consuming bathing ritual that could take up to 3 hours (as shown in Figure 1), during which, if any step felt incomplete, he would restart the entire process.
Figure 1
21-Step Showering Ritual of the Patient with Pure-C OCD
By December 2021, he had completely avoided touching his lower body (as it was used in urination and defecation). As it triggered internal discomfort, driving him to elaborate hand washing and sometimes showering. It wasted his time and frustrated his parents. This peaked at night, prompting him to place pillows between his arms and torso to prevent accidental contact while sleeping.
By May 2022, his avoidance started affecting his daily activities, like eating or using a mobile phone. He avoided doing basic activities until a proper ritual of hand washing was performed beforehand. He tried to regain control by attempting one prolonged ritualistic shower (lasting 6 hours), to permanently eliminate the discomfort and incompleteness. It provided temporary relief (1 compulsion-free week), but the symptoms recurred abruptly.
Due to excessive scolding from his parents, he developed a fear of experiencing these internal sensations of physical discomfort and incompleteness, resulting in a rigid posture to prevent accidental body contact. Sleep disturbances also emerged. Further, his mother also tried to restrict his water access during bathing to reduce the time spent in showers, which worsened family conflicts. He noticed that emotional distress heightened his need to perform these rituals instead.
By January 2023, he developed more rules to feel ‘just right’, around how he wore his clothes, spending around 30 minutes ensuring his pants were worn correctly. For him, feeling complete or just right was necessary; failure of which would lead to persistence of internal discomfort in hands and body. To fasten his belt and tie, he relied on his mother. He believed that if he touched the belt excessively, then it would also force him to wash his hands to feel clean again.
In August 2024, his uncle, a pharmaceutical company manager, identified his condition and recommended that his mother seek treatment at a reputable psychiatric hospital. He presented with complaints of loss of control over his cleaning-related behaviors, avoidance of entering the washroom, avoidance of touching the lower body by placing pillows in between torso and arms, excessive ritualistic washing (30 minutes for hand-washing) and cleaning (3-4 hours showering), repetitive checking of cleanliness (15–20 minutes post-wash), social withdrawal and family conflicts. The family was worried for his condition and often scolded him for showing such behavior. His access to mobile phones, food, and water was often restricted as a form of punishment. Since such punishments only increased the intensity of the symptoms, the parents discontinued it. Concludingly, overall family conflict and stress levels increased.
Pre-Treatment Psychological AssessmentThe major goal of the assessment was to evaluate if any intrusive thoughts preceded cleaning-related compulsions, along with the severity of the problem and distress. For this, the patient was formally and informally assessed.
Clinical InterviewA clinical interview gathered data on etiological factors (shown in Table 1). The patient was compliant and consented voluntarily, after his confidentiality rights were explained.
Table 1 Predisposing, Precipitating, Perpetuating, and Prognostic Factors of the Patient
|
Factors |
Explanation |
|---|---|
|
Predisposing Factors |
Adolescence, familial history of anxious compulsive traits, childhood perfectionistic tendencies |
|
Precipitating Factors |
Academic stress, media coverage of COVID-19 |
|
Perpetuating Factors |
Stress from familial conflicts, immediate relief after performing compulsion, avoidance of triggers, enabling or accommodating behaviors of the family (e.g., helping him in avoidance by placing pillows, adjusting clothes, etc.) |
|
Prognostic Factors |
Good insight, willingness for therapy, familial support, moderate severity of the symptoms |
Mental Status Examination (Roberts et al., 2013)
Initial mental status examination concluded that the patient was a young boy with a neat appearance and weather-appropriate dressing. He initially displayed irritability and reluctance to engage, with his father answering most questions. By the second session, his willingness to take part in the therapy improved. His speech was coherent with normal pacing. He reported no suicidal ideation but expressed hopelessness about his problems and family conflicts. His thoughts focused on ensuring proper washing, with compulsions of washing, and avoidance. No obsessions, delusions or hallucinations were noted, and cognitive functions were intact. He showed insight into his condition, recognizing the irrationality of his behaviors and the need for treatment.
Anxiety Hierarchies (Hyman & Pedrick, 2010)
To assess the patient’s discomfort related to various stimuli, a main anxiety hierarchy was collaboratively developed, identifying six key themes causing major discomfort (shown in Table 2). Each situation was rated using the Subjective Units of Discomfort Scale (SUDS). Based on this, further sub-hierarchies were built during the intervention for gradual exposure to varying intensities of urges (as discussed in the therapeutic intervention section).
Table 2 Main Anxiety Hierarchy of the Patient with Pure-C OCD
|
Anxiety Causing Stimuli |
SUD (1-100) |
|---|---|
|
Entering and using the washroom |
100 |
|
Sleeping without placing pillows between his arms and torso |
90 |
|
Doing daily activities without ritualistic hand washing |
80 |
|
Reducing steps in ritualistic showering |
70 |
|
Not following ritualist handwashing (and post-washing rituals) |
70 |
|
Touching the body with the hand and not washing afterwards |
60 |
As no preceding obsession was reported, a thought record was introduced for purely compulsive OCD symptoms, with the supervisor’s approval (given in Table 3). Its functional analysis identified that the major triggers for the patient were accidentally touching the lower body and using the washroom, which gave rise to tension and irritability in the hands. This tension persisted until, relieved by 15-20 minutes of handwashing. With good insight, he recognized the consequences (skin damage, familial discord, and time waste).
Table 3 Modified OCD Thought Record for Pure C Compulsions
|
Prompt |
Explanation |
|---|---|
|
Situation (Trigger) |
Touched left thigh accidentally while eating |
|
Internal Sensation/Urge |
Felt tension/itching/ scratching in hands, tried to bear it but could not for more than 1 minute. |
|
Compulsive Behavior |
Washed hands for around 15- 20 minutes, then spent 5 minutes making sure I felt calm and didn't have any tension/itching anymore. |
|
Short-term Relief |
Temporary relief and completeness |
|
Long-term Consequences |
My hands became dry and cracked; I got scolded by my parents, and was also late for my tuition |
|
Alternative Response* |
Tolerated the discomfort in the hands for 5 minutes, then distracted myself with a task. |
Note. *Alternative Response was introduced later in the sessions, when ERP was introduced.
Compulsive Activities Checklist-Revised (CAC-R) (Steketee & Freund, 1993)
It is a 28-item measure used to gain insight into all compulsive strategies of the patient and their associated distress. The most prominent compulsive behavior was washing, avoidance, and reassurance-seeking from self and others. No magical/undoing, perfectionistic, touching, counting, self-mutilative, or mental compulsions were present. These results illustrated the compulsions to target response prevention.
Yale-Brown Obsessive Compulsive Scale (Y-BOCS) (Goodman et al., 1989)
It is a standardized semi-structured interview to assess obsessive-compulsive symptom severity. The patient scored 15, depicting moderate severity. Prominent compulsive themes related to cleaning and washing. He engaged in excessive hand washing, arm washing, and a ritualized showering routine, spending more than 8 hours on compulsions, leading to moderate disruption in daily activities and a moderate level of distress. Some unsuccessful resistance against compulsions and only slight control over compulsive rituals were reported. Furthermore, no obsessive theme was present prominently. A slight concern of disgust with bodily waste was present, which was limited only to how it might feel instead of the actual consequences of contamination. In summary, obsession is not applicable in this case, as the patient’s symptoms were purely compulsive, resulting in a score of 0 across all obsession-related categories.
DiagnosisF42.2. Obsessive-Compulsive Disorder, with fair insight.
Case ConceptualizationThe case was conceptualized using the habit hypothesis of compulsion, discussing the sensory-driven urges to perform cleaning and washing rituals until achieving a sense of feeling "just right" (Miguel et al., 2000). His symptoms began during a period of academic stress, with handwashing escalating to ritualistic showers lasting up to 6 hours, driven by internal sensory tension rather than obsessive fears (Coles et al., 2003). The compulsions provided temporary relief but led to significant functional impairment, including disrupted daily routines and family conflicts (Summerfeldt, 2004).
The predisposing factors could be genetic vulnerability, as a family history of OCD-like behaviors was present (Rajendram et al., 2017). Further, his childhood perfectionistic tendencies towards orderliness and symmetry might have increased his susceptibility to sensory-driven compulsions (Coles et al., 2003). Academic stress might have exacerbated compulsive behaviors (Cervin, 2022; Rodgers et al., 2015), which were then reinforced by COVID-19 media coverage (Hassoulas et al., 2021). In a research study, pure-compulsive OCD depicted a lower age of onset and was mainly related to school-related stress (Rodgers et al., 2015). These factors combined precipitated the first episode of clinical OCD. Stress from familial conflicts (Peris et al., 2008) and immediate relief of sensory tension after performing the compulsive acts negatively reinforced the compulsive behaviors (Foa et al., 1995), resulting in an increased frequency of compulsions. Further, avoidance of triggers (Simpson & Hezel, 2019) and enabling behaviors of the family (Palo & Hertz, 2024; Storch et al., 2007) supplemented the perpetuation of the symptoms.
Since the patient had a good insight regarding the irrationality of his compulsive behavior and despite familial conflicts, parents were willing to collaborate therapeutically; this could enhance treatment engagement (Foa et al., 1995; Storch et al., 2007). The prognosis of the patient was good, with moderate severity of symptoms (Goodman et al., 1989).
Based on the conceptualization, treatment should focus on ERP to target compulsions and reduce reliance on rituals, alongside family counseling to address enabling behaviors, Cognitive Restructuring to address any dysfunctional beliefs, and enhancing problem solving skills to adequately deal with academic and familial stress (Palo & Hertz, 2024; Simpson & Hezel, 2019; Uhre et al., 2019).
Ethical ConsiderationIn adherence to the APA ethics code, the confidentiality and anonymity of the patient were maintained. Informed consent was taken before assessment, and during each level of therapy, the patient was educated about the treatment protocol, risks, and benefits to ensure voluntary participation.
Duration and Treatment ProtocolA total of 95 sessions were conducted for 8 months. Family-based ERP was used as the main modality to reduce compulsive and avoidance behaviors. Recent research has shown that ‘High Intensity ERP’ (Trent et al., 2025), works better with adults and youth, with numerous compulsions. It involves longer and more frequent sessions than traditionally weekly 1 hour-long sessions (Trent et al., 2025). Since a number of different compulsions (as shown in Table 2) were reported, each of the problematic behaviors needed a specific dedicated ERP. So, high-intensity ERP was used, resulting in a longer duration of treatment. An average of 3 sessions was conducted each week, except for ritualistic showering, which required 4 sessions per week (a total of 79 sessions was conducted). On average, each ERP delivered effective results in 13 sessions. A detailed breakdown of sessions is given in Table 4. It continued for 6 months. The next 2 months implemented SFT and cognitive restructuring to buffer the long-term results of ERP, by reducing the problems related to academic and familial stress, and self-referent beliefs, respectively. A total of 16 sessions (2 per week) were conducted.
Table 4 No. of Sessions Conducted for each Symptom-Specific ERP
|
Symptom-Specific ERP |
Sessions |
|---|---|
|
ERP for Touching the Body Parts |
12 |
|
ERP for Ritualistic Hand Washing |
12 |
|
ERP for Ritualistic Showers |
16 |
|
ERP for Reduction of Avoidance Related to Daily-Life Activities. |
12 |
|
ERP for Reduced Inter-Body Parts Pillow Use During Sleep |
18 |
|
ERP for Washroom Exposure |
09 |
The primary goal of the therapy was to reduce compulsive behaviors and the associated distress, to increase the tolerance of internal sensory-driven urges without performing rituals, and improve daily-life functioning. It also focused on restructuring the maladaptive self-referent beliefs related to compulsions, encouraging a supportive family environment, and promoting long-term recovery. The eclectic therapeutic techniques used to achieve these goals are summarized in Table 4 below.
Table 4 >Treatment Plan for a 19-Year-Old Patient with Pure-C OCD
|
Therapeutic Goal |
Intervention |
|---|---|
|
To build trust and therapeutic alliance |
Rapport Building Active Listening Empathy Unconditional Positive Regard |
|
To educate the patient about the symptomatology of Pure-C OCD, treatment protocol, homework compliance, and discuss the expectations of the therapist, patient, and family |
Psychoeducation Socialization |
|
To reduce compulsive behavior and encourage a supportive environment |
Family-Based ERP |
|
To restructure the maladaptive self-referent and other positive beliefs related to compulsions |
Cognitive Restructuring Downward Arrow Evidence For and Against |
|
To help the patient deal with academic and familial problems in a healthy way |
SFT Time Management Assertiveness Training |
|
To educate the patient about relapses and ensure long-term recovery |
Relapse Prevention |
Psychoeducation involves educating the patient and the family about the diagnosis, triggers, symptoms, and treatment options for OCD. Homework compliance was emphasized, and collaborative problem-solving was encouraged to ensure better treatment outcomes. They were educated about ERP and the role of the family. Further, the ABCDE model (explained in Figure 2) was elaborated in terms of the vicious cycle of internal sensory urges, compulsion, and temporary relief.
Figure 2
ABCDE Model of Pure Compulsions or Pure-C OCD
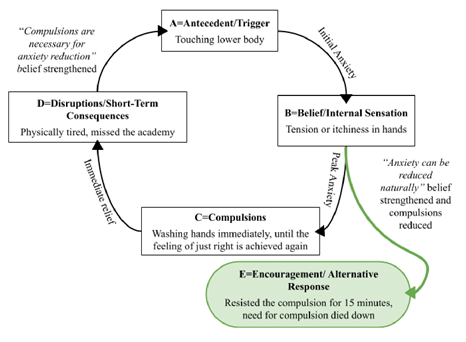
The patient was educated about the anxiety cycle, i.e., the anxiety reduces naturally after reaching the peak, without any external effort to break it. A behavioral experiment was conducted to understand ERP. The patient was asked about something he felt the least discomfort with, i.e., touching his chest. Then he was asked to touch it, resist the internal urge to wash his hands, and let the urge pass naturally. The patient succeeded in doing it, and the need to wash hands died after 15 minutes, which served as a basis for the effectiveness of ERP. To build on this, he was given an OCD thought record based on the ABCDE model, in which E = Empowerment (alternative response) was introduced after starting ERP. Lastly, the patient was educated about the persistent nature of anxiety, i.e., feeling anxiety below 20 SUDs is normal throughout the sessions.
Family-Based Exposure and Response Prevention (ERP)It involves making mini-hierarchies based on the themes of the main hierarchy (given in Table 2). Exposure activity with moderate anxiety (above 40) is selected. The patient is exposed to it, discomfort is allowed to rise, and any kind of response is prevented until the anxiety reduces naturally. A Daily Exposure Monitoring Form (Hyman & Pedrick, 1999) was assigned for every ERP. A total of 6 mini hierarchies were formed, starting from the least anxiety-provoking hierarchy, i.e., avoidance of touching body parts.
ERP for Touching the Body Parts. The goal was to reduce the avoidance and enable the patient to touch his various body parts and resist the compulsion to wash his hands afterward. A mini-exposure hierarchy with SUDs was built, shown in Table 5. The exposure started by touching the face and not washing hands afterwards. Also, the patient did not wash his hands before the exposure. The SUD was reduced to 20, for this step, in 2 weeks (40 attempts). For the rest of the exposure activities, it only took 1 month to reduce the SUD level, depicting a good prognosis. During this period, brief virtual counseling sessions were conducted every 2 days to record the progress and provide the necessary support.
Table 5 Mini-Anxiety Hierarchy List for ERP for Touching the Body Parts
|
Exposure Activity |
SUD (0-100) |
|---|---|
|
Touching inner thighs |
90 |
|
Touching the lower legs |
80 |
|
Touching feet |
70 |
|
Touching belly |
60 |
|
Touching chest |
50 |
|
Touching face |
40 |
|
Touching neck |
30 |
|
Touching arms |
20 |
The family acted as “coaches” instead of helpers to monitor, encourage, and reinforce response prevention. However, parental involvement was gradually reduced to promote independent management of compulsions (Palo & Hertz, 2024).
ERP for Ritualistic Hand Washing. The ritualistic handwashing consisted of washing hands and arms 3 times, checking whether he felt clean enough, and repeating the process until he felt just right. To reduce this, a strategic ERP was built, based on the Gradual Method (Hyman & Pedrick, 1999), with each step focusing separately on hand washing, arm washing, and delaying the checking (shown in Table 6). Further legal and illegal washes were also explained. If the patient was able to reduce handwashing for 3 days, the next exposure step was started (Hyman & Pedrick, 1999). It took around 1 month to reduce the anxiety level of each step below 20 SUD. Further frequency of arm washings was more easily reduced than hand washing, which was in turn more easily reduced than delaying the checking for just the right feeling.
During ritual delay attempts, he substituted checking with maladaptive self-reassurance after each wash, “he is feeling okay, it is not necessary to reduce the anxiety, the anxiety will die down, etc”. This is a frequent problem while dealing with compulsions (Hyman & Pedrick, 1999). As a solution, the self-reassurance was also delayed just like the checking behavior, making sure that the patient could experience anxiety without self-reassuring.
Table 6 Mini-Anxiety Hierarchy List for ERP for Ritualistic Hand Washing
|
Step |
Hand Washing |
Arm Washing |
Checking Delay |
Additional Modifications |
SUDS |
|---|---|---|---|---|---|
|
1 |
3 times |
2 times |
1 minute |
None |
45 |
|
2 |
2 times |
1 time |
3 minutes |
None |
55 |
|
3 |
1 time |
Skip 1 session each day |
5 minutes |
None |
65 |
|
4 |
1 time (legal washes) |
Skip 3+ sessions each day |
15 minutes |
Only essential legal washes (e.g., after using the toilet) |
75 |
|
5 |
1 time (legal washes) |
Skip a full day |
30 minutes |
Skipping arm washing |
85 |
|
6 |
1 time (using only half soap) |
Skip a full day |
1 hour |
Reduced soap use |
90 |
|
7 |
Washing only for 15 seconds |
Skip a full day |
2 hours |
Brief Hand washing |
95 |
|
8 |
1 time (<15 seconds) |
Skip a full day |
Rest of day |
Minimal hand washing |
100 |
ERP for Ritualistic Showers. Ritualistic Shower consisted of 21 steps, where each step was done 3 times (other than hair washing), and checking for feeling clean enough or just right followed every step (the detailed description is given in Figure 1). Using the Gradual Method, each step was reduced to half, i.e., 1 time, while the checking was delayed and reduced gradually, for the first week. In the second and third weeks, different steps were fused, while being done only 1 time. In the final fourth week, unnecessary steps were eliminated. After the establishment of a non-ritualistic shower, the showering was limited to only 1 shower per day. The detailed ERP is given in Table 7.
Table 7 Mini-Anxiety Hierarchy List for ERP for Ritualistic Showers
|
Step |
Washing Protocol |
Checking Protocol |
Key Modifications |
SUDS |
|---|---|---|---|---|
|
1 |
All steps 1 time |
Check after every 2 steps |
Initial reduction of unnecessary repetitions for each step |
40 |
|
2 |
Left/right body parts washed together |
Check after every 4 steps |
Combining Steps |
50 |
|
3 |
Upper/lower arms washed together (both sides) |
Check after each body part (e.g., arms, legs) |
Combining arm washing |
60 |
|
4 |
Neck + face + full arms in 1 go |
Check after each body section (upper/lower) |
Combining Upper body parts |
65 |
|
5 |
Torso + neck + face + full arms |
Check after each body section |
Combined full upper body |
70 |
|
6 |
Upper body + feet |
Check once + delay 5 minutes post-shower |
Introduces delayed checking |
75 |
|
7 |
Upper body + feet + lower legs |
Check once + after shower, delay 10 minutes |
Combines lower body parts |
80 |
|
8 |
Upper body + feet + lower legs + thighs |
No checking until 30 minutes post |
Eliminate mid-shower checks and combined upper and lower body wash |
85 |
|
9 |
Full body + hair in 1 go |
Delay check 1 hour post-shower |
Adds hair washing |
90 |
|
10 |
Full body (skip face rewash post-shower) |
Delay check 2 hours |
Begins omitting facial rewash |
95 |
|
11 |
Full body (skip face + arms rewash post-shower) |
Delay check rest of the day |
Eliminates arm rewash |
100 |
|
12 |
Full body 1 time (skip face/arms rewash post-shower) + rewashing hands only 1 time after shower |
No checking until the next day |
Establishment of a non-ritualistic shower |
100 |
ERP for Reduction of Avoidance Related to Daily-Life Activities. The patient avoided engaging in daily life activities, as they gave rise to an internal sensation to wash their hands or body. The ERP incorporated these daily life activities, without engaging in compulsion (as shown in Table 8). This ERP accompanied Step 3 of the ‘Gradual Method’(Hyman & Pedrick, 1999). To enhance ERP effectiveness, a targeted list of compulsions and safety behaviors to withhold was shared, based on previously observed problematic patterns. In 1 month, the patient was able to do the majority of daily activities with minimal anxiety.
Table 8 Mini-Anxiety Hierarchy List for ERP for Reduction of Avoidance Related to Daily-Life Activities
|
Step |
Exposure Task |
Key Prohibited Compulsions |
SUDS |
|---|---|---|---|
|
1 |
Touch personal items (5 mins) |
No wiping/cleaning items afterward |
40 |
|
2 |
Fasten the tie independently |
No post-tying hand washing/checking |
50 |
|
3 |
Fasten the belt independently |
No adjusting/retying to "feel right" |
60 |
|
4 |
Tie shoelaces independently |
No re-tying or foot cleaning |
70 |
|
5 |
Eat roti with hands (1 wash after) |
No excessive scrubbing/pre-washing |
75 |
|
6 |
Apply lotion to the dry upper body |
No pre-application washing/post-application washing rituals |
80 |
|
7 |
Apply lotion to upper body + lower legs/feet |
No pre-application washing/post-application washing rituals |
90 |
|
8 |
Apply lotion to the full dry body |
No pre-application washing/post-application full washing rituals |
100 |
ERP for Reduced Inter-Body Parts Pillow Use During Sleep. Pillow use caused extreme distress, as accidental body contact triggered either somatic tension or immediate compulsive washing. An ERP was built to gradually increase the contact of the body with itself during sleep (shown in Table 9). Further, sleep-enhancing strategies (based on cognitive behavioral strategies suggested by Morin (2004), i.e., maintaining sleep hygiene, stimulus control, and sleep restriction) were used to improve the quality of sleep and to fall asleep within 1 hour. It took 1.5 months for the patient to sleep without the use of any pillows, although the patient struggled to sleep early. So, sleep-enhancing strategies continued, until the patient was able to sleep within 30 minutes.
Table 9 Mini-Anxiety Hierarchy List for ERP for Reduced Inter-Body Parts Pillow Use During Sleep
|
Step |
Upper Body Exposure |
Lower Body Exposure |
Duration |
Prohibited Behaviors |
SUDS |
|---|---|---|---|---|---|
|
1 |
Exchange Pillow with Light fabric on the torso |
Full pillow use maintained |
All night |
No extra fabric layers |
30 |
|
2 |
Light fabric under both arms |
Full pillow use maintained |
All night |
No arm repositioning |
40 |
|
3 |
No fabric, arms slightly near torso |
Full pillow use maintained |
All night |
No verification of arms touching |
50 |
|
4 |
Arms lightly touch the torso |
Full pillow use maintained |
15 minutes |
No washing after contact |
60 |
|
5 |
Arms lightly touch the torso |
Exchange Pillow with light fabric between legs |
30 minutes |
Keep legs relaxed, no leg tensing |
65 |
|
6 |
Arms fully touch torso |
Legs wide apart (no fabric) |
30 minutes |
No verification of legs touching |
70 |
|
7 |
Arms fully touch torso (for 1 hour) |
Legs lightly touching |
15 minutes (for legs) |
No post-exposure rituals |
75 |
|
8 |
Arms fully touch torso (all night) |
Legs lightly touching |
30 minutes (for legs) |
No washing after contact |
80 |
|
9 |
Arms fully touch torso (all night) |
Legs fully touching |
30 minutes (for legs) |
No sheet barriers |
85 |
|
10 |
Arms fully touch torso (all night) |
Legs fully touching |
1 hour |
No distraction techniques |
90 |
|
11 |
Arms fully touch torso (all night) |
Legs fully touching (all night) |
Full night |
No next-day compensation |
95 |
ERP for Washroom Exposure. Washroom use provoked tension, so he avoided it until it was absolutely necessary, followed by an immediate washing or showering ritual. An ERP was built (given in Table 10), and the same principles as above were followed to reduce his avoidance. Each activity was done 5 times daily, and it took only 3 weeks to achieve the fully functional toilet-use with minimal anxiety. By this point, the therapist sessions were also spaced out, at least fortnightly, to increase the independence of the patient.
Table 10 Mini-Anxiety Hierarchy List for ERP for Washroom Exposure
|
Step |
Exposure Task |
Duration |
Prohibited Safety Behaviors |
SUDS |
|---|---|---|---|---|
|
1 |
Stand outside washroom door |
5 minutes |
No hand washing afterward |
40 |
|
2 |
Enter washroom and stand there, no touching |
2 minutes |
No deep breathing or self-reassurance while in the washroom |
50 |
|
3 |
Touch door handle (from inside) |
30 seconds |
No washing hands afterwards |
55 |
|
4 |
Touch and turn on faucet briefly |
15 seconds |
No immediate hand wash |
60 |
|
5 |
Sit on a closed toilet (fully clothed) |
3 minutes |
No self-reassurance during the activity, no shower or changing clothes afterwards |
65 |
|
6 |
Flush toilet (with fingers), with 1 legal handwash (15 sec) afterwards |
1 flush |
Handwashing not more than 15 seconds afterwards |
70 |
|
7 |
Use sink normally (water only) |
30 seconds |
No soap use No washing arms |
75 |
|
8 |
Full toilet use (clothed) |
5 minutes |
No post-use clothing change, or showering |
80 |
|
9 |
Actual urination |
Normal time |
No leg/body positioning rituals No excessive hand washing No excessive checking afterwards |
85 |
|
10 |
Defecation |
Normal time |
No leg/body positioning rituals No excessive hand washing No excessive checking afterwards |
90 |
|
11 |
Full washroom routine (enter-use-exit) |
Normal use |
Only 1 legal hand wash (20 sec max), No checking afterwards |
100 |
Self-referent beliefs are beliefs about oneself. They have long been considered the predictor of physical and mental health (Kaplan, 2007). These beliefs were elicited during therapy through the downward arrow technique, i.e., “I must be a mentally or emotionally weak person because I can’t control my compulsions”. Cognitive restructuring was done throughout the sessions to work on these beliefs. Evidence for and against technique was used to challenge this belief. Evidence was collected based on earlier ERPs, further, the OCD thought record functioned as solid proof that he indeed had control over his compulsive behaviors, and he was not mentally weak. Normalization was also applied to educate the patient about the non-clinical nature of compulsive behaviors and how common they were among the majority of individuals. By the end of the therapy, the patient had a strong alternative belief, i.e., “My compulsions are learned responses; I can train my brain to learn alternative responses. Everyone has some level of compulsions; it does not make anyone mentally weak.”
Solution-Focused Therapy (SFT)Lack of adequate time management marked the start of clinical OCD for the patient, while further familial conflicts worsened the symptoms. To ensure long-term recovery, active problem-solving skills were necessary to be mastered. For academic stress, effective time management skills were practiced one at a time, such as the Eisenhower matrix (Dmytryshyn & Goran, 2022), Pomodoro technique (Wang et al., 2010), memory tests, and study sprints (Roediger & Karpicke, 2006).
To deal with familial conflicts, family psychoeducation was provided to parents and siblings. Further assertiveness skills training (Speed et al., 2017) was used with the patient, where he learned to use ‘I’ sentences during conflicts, de-escalation strategies, the role of body language, and the use of open communication with family members. The patient and the family were trained throughout the therapy, and contrasted role plays (MacNeilage & Adams, 1979) were often used to enhance the learned strategies. All these strategies were proven to be effective.
Relapse PreventionRelapse prevention is an essential part of OCD psychotherapy. It consisted of three 90-minute-long sessions, in which the patient was trained for self-exposure, expectations of setbacks, cognitive restructuring, and planned lifestyle changes. The ‘chronic illness model’ was explained to challenge the belief that OCD will be cured, i.e., OCD is a long-lasting condition with fluctuating symptoms, and the patient is likely to experience full-blown compulsive symptoms in the future. To deal with it, written instructions were given, which included trigger identification, written sample ERP, alternative problem solving, and the alternative belief that “relapse is not a setback, rather an opportunity to practice newly learned coping skills”.
Results
Based on the post-assessment, there was an 80% decrease in the compulsions of the patient, which shows good recovery. Based on the score of Y-BOCS, the total score reduced from 15 to 6; details are given in Figure 3 below.
Figure 3
Y-BOCS Scores of Pre-Assessment and Post-Assessment
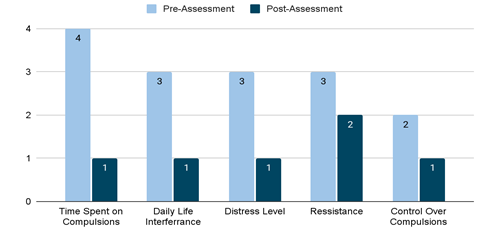
Figure 4
SUD Levels (0-100) of the Main Anxiety Hierarchy Pre-Assessment and Post-Assessment
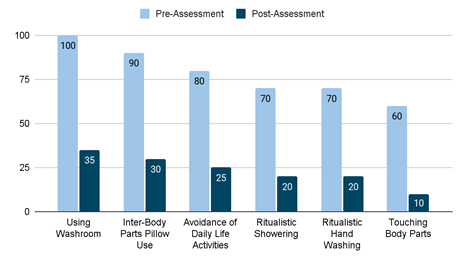
Major improvements occurred in the time spent on hand washing (from 30 minutes to 20 seconds), and showering (from 3 hours to 20 minutes). The major changes in the SUD level of the main anxiety hierarchy are given in Figure 4.
Discussion
The current study focused on reducing the compulsions and improving the problem-solving capabilities of the patient presenting with Pure-C OCD. The patient was assessed through both formal and informal assessments. He was diagnosed with OCD with fair insight, which predicted his prognosis to be good. The key themes of compulsion were avoidance and excessive ritualistic handwashing and showering. ERP started with exposure to touching body parts, the original SUDs decreased from 60 to 10. The success was majorly attributed to family members acting as coaches, instead of enablers (Storch et al., 2007). This change forced the patient to face anxiety alone, which, when successful, strengthened the belief that compulsions are just learned behaviors that can be changed or reduced. This belief improved the prognosis of the later ERPs. However, it soon gave rise to excessive self-reassurance during the second ERP aimed at ritualistic handwashing. The post-handwash checking behavior was replaced by excessive self-reassurance. This aligns with existing literature, as self-reassurance is most found in OCD-related disorders and guards the prognosis (Kobori & Salkovskis, 2012). So, the ERPs focused on withholding self-reassurance along with compulsive behavior by introducing ‘gradual delay’ (Clark, 2019). Similarly, the rest of the ERPs were targeted, showing significant improvement (see Figures 3 & 4).
ERP alone has limited short-term benefits. For long-term benefits, it is necessary to introduce skills so the patient can deal with real-life stressors. Patients with anxiety disorders show better outcomes for problem-focused treatments (Yulish et al., 2017). Two key problematic areas were found: academic stress and familial conflicts. The SFT was used to find out the solutions that worked for the patient (Jerome et al., 2023). Academic stress stemmed from perfectionistic standards set by parents and a lack of time management. Family psychoeducation (Storch et al., 2007), time management, and note-taking academic techniques alleviated his added stress. Further, assertiveness training helped him in dealing with familial conflicts with a better approach (Speed et al., 2017), resulting in a lower frequency. Lastly, cognitive restructuring was used to challenge any residual self-referent or dysfunctional beliefs about the patient’s capability or compulsions.
Limitations and SuggestionsOverall, the case study highlighted that pure compulsions may respond well to behavioral interventions and SFT. It has several important clinical implications, particularly because it acts as a guide for future research and therapists to work with “not just right” experiences (NJREs). While these results are promising for similar cases of purely compulsive OCD, further research should examine generalizability to other subtypes of compulsions. Long-term follow-up is important to assess the maintenance of results. Overall, this case provides compelling evidence that compulsions are a core, treatable part of OCD that can be effectively addressed even in the absence of obsessional thoughts (Leckman et al., 1994).
ConclusionThis case study combines ERP with SFT to treat pure compulsion in pure-C OCD. The results show behavioral treatments (such as ERP) as the most effective treatment for short-term compulsion relief. For long-term improvement, solution-focused techniques and cognitive restructuring techniques help to challenge any perpetuating factors. Overall, an eclectic approach to the treatment of purely compulsive OCD is recommended.
Conflict of Interest
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding Details
This study has not received funding.
REFERENCES
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425787
Cervin, M. (2022). Obsessive-compulsive disorder. Psychiatric Clinics of North America, 46(1), 1–16. https://doi.org/10.1016/j.psc.2022.10.006
Clark, D. A. (2019). Cognitive-Behavioral therapy for OCD and its subtypes. Guilford Publications.
Coles, M. E., Frost, R. O., Heimberg, R. G., & Rhéaume, J. (2003). “Not just right experiences”: perfectionism, obsessive–compulsive features and general psychopathology. Behaviour Research and Therapy, 41(6), 681–700. https://doi.org/10.1016/s0005-7967(02)00044-x
de Shazer, S., & Berg, I. K. (1997). ‘What works?’ Remarks on research aspects of solution-focused brief therapy. Journal of Family Therapy, 19(2), 121–124. https://doi.org/10.1111/1467-6427.00043
Dmytryshyn, M., & Goran, T. (2022). Proposal of an effective time management system. Management, 27(2), 283–298. https://doi.org/10.30924/mjcmi.27.2.15
Foa, E. B., Kozak, M. J., Goodman, W. K., Hollander, E., Jenike, M. A., & Rasmussen, S. A. (1995). DSM-IV field trial: Obsessive-compulsive disorder. The American Journal of Psychiatry, 152(1), 90–96. https://doi.org/10.1176/ajp.152.1.90
Gillan, C. M., Papmeyer, M., Morein-Zamir, S., Sahakian, B. J., Fineberg, N. A., Robbins, T. W., & De Wit, S. (2011). Disruption in the balance between goal-directed behavior and habit learning in obsessive-compulsive disorder. American Journal of Psychiatry, 168(7), 718–726. https://doi.org/10.1176/appi.ajp.2011.10071062
Gillan, C. M., & Sahakian, B. J. (2014). Which is the driver, the obsessions or the compulsions, in OCD? Neuropsychopharmacology, 40(1), 247–248. https://doi.org/10.1038/npp.2014.201
Goodman, W. K. (1989). The Yale-Brown Obsessive Compulsive scale. Archives of General Psychiatry, 46(11), 1006– 1011. https://doi.org/10.1001/archpsyc.1989.01810110048007
Hassoulas, A., Umla-Runge, K., Adams, O., Scurlock-Green, M., Zahid, A., Hassoulas, A., & Panayiotou, E. (2021). The impact of the COVID-19 pandemic on symptom subtypes of obsessive-compulsive disorder: A cross-sectional study. BJPsych Open, 7(Suppl 1), S253–S254. https://doi.org/10.1192/bjo.2021.679
Hyman, B. M., & Pedrick, C. (1999). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder. New Harbinger Publications.
Hyman, B. M., & Pedrick, C. (2010). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder (3rd ed.). New Harbinger Publications.
Jacoby, R. J., & Abramowitz, J. S. (2016). Inhibitory learning approaches to exposure therapy: A critical review and translation to obsessive-compulsive disorder. Clinical Psychology Review, 49, 28–40. https://doi.org/10.1016/j.cpr.2016.07.001
Jerome, L., McNamee, P., Abdel-Halim, N., Elliot, K., & Woods, J. (2023). Solution-focused approaches in adult mental health research: A conceptual literature review and narrative synthesis. Frontiers in Psychiatry, 14, Article e1068006. https://doi.org/10.3389/fpsyt.2023.1068006
Kaplan, H. B. (2007). Self-Referent constructs and medical sociology: In search of an integrative framework. Journal of Health and Social Behavior, 48(2), 99–114. https://doi.org/10.1177/002214650704800201
Kobori, O., & Salkovskis, P. M. (2012). Patterns of reassurance seeking and reassurance-related behaviours in OCD and anxiety disorders. Behavioural and Cognitive Psychotherapy, 41(1), 1–23. https://doi.org/10.1017/s1352465812000665
Leckman, J. F., Walker, D. E., Goodman, W. K., Pauls, D. L., & Cohen, D. J. (1994). “Just right” perceptions associated with compulsive behavior in tourette’s syndrome. American Journal of Psychiatry, 151(5), 675–680. https://doi.org/10.1176/ajp.151.5.675
MacNeilage, L. A., & Adams, K. A. (1979). The method of contrasted role-plays: An insight-oriented model for role-playing in assertiveness training groups. Psychotherapy, 16(2), 158–170. https://doi.org/10.1037/h0086043
Meyer, V. (1966). Modification of expectations in cases with obsessional rituals. Behaviour Research and Therapy, 4(4), 273–280. https://doi.org/10.1016/0005-7967(66)90023-4
Miguel, E. C., do Rosário-Campos, M. C. D., da Silva Prado, H., do Valle, R. D., Rauch, S. L., Coffey, B. J., Baer, L., Savage, C. R., O’Sullivan, R. L., Jenike, M. A., & Leckman, J. F. (2000). Sensory phenomena in obsessive-compulsive disorder and tourette’s disorder. The Journal of Clinical Psychiatry, 61(2), 150–156. https://doi.org/10.4088/jcp.v61n0213
Morin, C. M. (2004). Cognitive-behavioral approaches to the treatment of insomnia. The Journal of Clinical Psychiatry, 65, 33–40.
Palo, A., & Hertz, A. (2024). Family-based exposure and response prevention for obsessive-compulsive disorder: A case study. Journal of Cognitive Psychotherapy, 38(4), 310–332. https://doi.org/10.1891/jcp-2023.0013
Peris, T. S., Bergman, R. L., Langley, A., Chang, S., Mccracken, J. T., & Piacentini, J. (2008). Correlates of accommodation of pediatric obsessive-compulsive disorder: Parent, child, and family characteristics. Journal of the American Academy of Child & Adolescent Psychiatry, 47(10), 1173–1181. https://doi.org/10.1097/chi.0b013e3181825a91
Rajendram, R., Kronenberg, S., Burton, C. L., & Arnold, P. D. (2017). Glutamate genetics in obsessive-compulsive disorder: A review. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 26(3), 205–213.
Roberts, L. W., Layde, J. B., & Balon, R. (2013). International handbook of psychiatry: A concise guide for medical students, residents, and medical practitioners. World Scientific Publishing Company.
Rodgers, S., Ajdacic-Gross, V., Kawohl, W., Müller, M., Rössler, W., Hengartner, M. P., Castelao, E., Vandeleur, C., Angst, J., & Preisig, M. (2015). Comparing two basic subtypes in OCD across three large community samples: A pure compulsive versus a mixed obsessive–compulsive subtype. European Archives of Psychiatry and Clinical Neuroscience, 265(8), 719–734. https://doi.org/10.1007/s00406-015-0594-0
Roediger, H. L., & Karpicke, J. D. (2006). Test-enhanced learning. Psychological Science, 17(3), 249–255. https://doi.org/10.1111/j.1467-9280.2006.01693.x
Simpson, H., & Hezel, D. (2019). Exposure and response prevention for obsessive-compulsive disorder: A review and new directions. Indian Journal of Psychiatry, 61(7), 85. https://doi.org/10.4103/psychiatry.indianjpsychiatry_516_18
Speed, B. C., Goldstein, B. L., & Goldfried, M. R. (2017). Assertiveness training: A forgotten evidence‐based treatment. Clinical Psychology Science and Practice, 25(1). https://doi.org/10.1111/cpsp.12216
Steketee, G., & Freund, B. (1993). Compulsive Activity Checklist (CAC): Further psychometric analyses and revision. Behavioural Psychotherapy, 21(1), 13–25. https://doi.org/10.1017/s0141347300017766
Storch, E. A., Geffken, G. R., Merlo, L. J., Jacob, M. L., Murphy, T. K., Goodman, W. K., Larson, M. J., Fernandez, M., & Grabill, K. (2007). Family accommodation in pediatric obsessive–compulsive disorder. Journal of Clinical Child & Adolescent Psychology, 36(2), 207–216. https://doi.org/10.1080/15374410701277929
Summerfeldt, L. J. (2004). Understanding and treating incompleteness in obsessive‐compulsive disorder. Journal of Clinical Psychology, 60(11), 1155–1168. https://doi.org/10.1002/jclp.20080
Trent, E. S., Zhou, R. J., Mammo, L., Goodman, W. K., & Storch, E. A. (2025). High intensity approaches to exposure and response prevention for obsessive-compulsive disorder. Behavioural Brain Research, 481, Article e115427. https://doi.org/10.1016/j.bbr.2025.115427
Uhre, C. F., Uhre, V. F., Lønfeldt, N. N., Pretzmann, L., Vangkilde, S., Plessen, K. J., Gluud, C., Jakobsen, J. C., & Pagsberg, A. K. (2019). Systematic review and meta-analysis: Cognitive-behavioral therapy for obsessive-compulsive disorder in children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 59(1), 64–77. https://doi.org/10.1016/j.jaac.2019.08.480
Wang, X., Gobbo, F., & Lane, M. (2010). Turning time from enemy into an ally using the pomodoro technique. In D. Šmite, N. Moe, & P. Ågerfalk (Eds.), Agility across time and space (pp. 149–166). Springer. https://doi.org/10.1007/978-3-642-12442-6_10
Watzlawick, P., Weakland, J. H., & Fisch, R. (1974). Change; Principles of problem formation and problem resolution. W. W. Norton.
Yulish, N. E., Goldberg, S. B., Frost, N. D., Abbas, M., Oleen-Junk, N. A., Kring, M., Chin, M. Y., Raines, C. R., Soma, C. S., & Wampold, B. E. (2017). The importance of problem-focused treatments: A meta-analysis of anxiety treatments. Psychotherapy, 54(4), 321–338. https://doi.org/10.1037/pst0000144