Madeeha Fatima1, Aamna Habib2*, Faiza Habib3, Kashaf Saleem1, Ramsha Riaz1, Sana Gulnaz1, Aqsa Ahmed1, Zaryab Fatima1, Momina Shahid1, Sadaf Waseem1, Nayab Sajid4, and Aneeb Nadeem1
1Department of Pharmacy, The University of Faisalabad, Pakistan
2Madina College of Pharmacy, The University of Faisalabad, Pakistan
3Avicenna Medical College, Lahore, Pakistan
4University of Lahore, Pakistan
* Corresponding Author: [email protected]
Hepatitis C infection is a global health issue. It is a growing challenge in Faisalabad, Pakistan, where at least 24% of the population is currently suffering from hepatitis C. If left untreated, HCV infection may lead to liver cirrhosis and hepatocellular carcinoma. The current study aimed to describe the various prescription trends of hepatitis C medication therapy in Faisalabad, Pakistan. It also aimed to evaluate the effectiveness of therapy and the satisfaction level of patients with their treatment. A comparative cross-sectional survey was carried out among patients receiving HCV medication therapy. For this purpose, a structured and close-ended questionnaire was completed by 270 patients. Comparative data analysis was performed based on selected variables, namely age, gender, marital status, current medication and its adverse effects. The prevalence of HCV in age group >40 was 63.3% and in age group <40, it was 36.7%. While, the prevalence of HCV in married individuals was 91% and its prevalence in unmarried individuals was 8.5%. Moreover, it was found that sofosbuvir was used by 24.8% of patients, daclatasvir was used by 24.4% of patients, entacavir was used by 0.4% of patients, acyclovir was used by 0.7% of patients, ribavirin was used by 7.8% of patients, and pegylated alpha 2b was used by 1.5% of patients. The trend of using combination therapy comprised interferon+ribavirin (1.5%) and velpatasvir+sofosbuvir (38.9%). The use of combination drug was found to be more common in patients of age group >40 (34.1%) than patients in age group <40 (8.8%). It was observed that lack of constant medical care and cost of therapy are major problems in the eradication of disease.
Keywords: current trends, hepatitis C virus (HCV), patients, pharmacotherapy trends
Globally, more than 3% of the world’s population is infected with HCV [1]. The reported prevalence of hepatitis C infection varies in different countries and remains highest in Asia, North Africa, and the Middle East. While, it is moderate in South Asia, Sub Saharan Africa, Central and South America, Carribbean, Oceania, Australasia, Central, Eastern, and Western Europe, and remains lowest in Tropical Latin America and North America [2]. Notably, 15-20% of HCV patients experience recovery but 75-85% progress towards hepatitis C [3]. According to various studies, about 24% population of Faisalabad suffers from hepatitis C and this ratio is still increasing, as compared to other cities of Pakistan [4]. Hepatitis C is the foremost cause of liver-related morbidity, liver transplantation, and mortality [5]. In Pakistan, the treatment rate of hepatitis is only 1%. The reason behind the increasing ratio of hepatitis and its low treatment rate is the lack of awareness about the causes and modes of transmission of the disease, costly treatment, and lack of trained health care professionals [6].
Interferon (IFN) was first employed in 1986 [7] and in the year 2001, a combination of ribavirin (RBV) and interferon (IFN) was prescribed for the first time. In the year 2004, the combination therapy of PEGylated interferon (PEG-IFN) alpha with ribavirin was introduced as standard treatment [8]. The use of interferon was discontinued due to its major side effects that overshadowed its therapeutic effect (1-6SI). Despite decreasing its dose, the problem of its toxicity remained persistent [9, 10]. Early observed side effects were myalgias, abdominal cramps, insomnia, anorexia, and fever. On long term use, the side effects observed were bone marrow suppression, urinary tract infections, lung abscess, brain abscess, hyperthyroidism, hypothyroidism, and delirium [11].
Hence, during the years 2001-2011, the standard drug used for the treatment of HCV was a combination of interferon and ribavirin. However, in 2015, Food And Drug Administration (FDA) and European Medical Agency (EMA) approved several combinations of direct acting antiviral (DAA) drugs and these combinations showed better response in the treatment of infection with a lower rate of adverse effects [12]. The use of direct acting antivirals for the management of HCV improves the condition of patients, significantly. Various inhibitors of viral proteins (NS3/4A protease, NS5A, and NS5B polymerase) help to eliminate HCV infection from biological systems [13].
The observed side effects of antivirals used to treat HCV infection are chills, ulcers, sores, weakness, pale skin, changing behavior, dizziness, insomnia, shortness of breath, headache, nausea, allergic reactions, constipation, fever, and body ache [14].
This cross-sectional study was conducted in tertiary care hospitals of Faisalabad, Pakistan from January 2019 to April 2019. Inclusion criterion was patients diagnosed with HCV infection and currently receiving HCV medication therapy without any discrimination of age. A self-structured questionnaire was designed according to the National Standard Treatment Guidelines for Hepatitis and distributed among 270 patients prescribed with medications for HCV infection in Allied Hospital, Liver Center, District Head Quarters Hospital Faisalabad, Social security Hospital, and Aziz Fatima Hospital Faisalabad. The location for patients’ interviews was decided after approval from the coordinators of different hospitals. Medical staff was present while the questionnaire was completed. The questionnaire included questions about medication, route of administration, adverse effects, satisfaction level with the treatment, cost effectiveness of the treatment, and diagnostic tests. Furthermore, information about age, gender, marital status, occupation, qualification, and knowledge about high risk factors (blood transfusion, intravenously drug abuse, and sexual behavior) was collected.
2.1. Statistical Analysis
Quantitative variables are analyzed by using Student’s t-test. Differences were considered to be significant when p <0.05. SPSS version 21 was used for all calculations.
2.2. Ethical Approval
Ethical committee of the University of Faisalabad approved the study. Patients and their guardians who participated in this study provided their written informed consent. Interview was conducted according to the principles of the Declaration of Helsinki.
The current retrospective study was conducted in different hospitals of Faisalabad with the aim to assess the prescription trends of hepatitis C among individuals of different age groups and occupations and to check the cost effectiveness of the therapy. Table 1 depicts that out of 270 patients who participated in this survey, 156 (57.8%) were female and 114 (42.2%) were male patients. The patients were categorized into two age groups, that is, < 40 years and > 40 years of age. The first age group included 99 (36.7%) patients and the second included 172 (63.3%) patients. Furthermore, 247 (91.5%) patients were married and 23 (8.5%) were single.
Table 1. Comparison of Demographic Data
|
Category |
Frequency |
Percentage Data |
p-value |
|
Age |
|
|
<0.001 |
|
<40 years |
99 /270 |
36.7% |
|
|
>40 years |
171/270 |
63.3% |
|
|
Gender |
|
|
<0.001 |
|
Female |
114 |
42.2% |
|
|
male |
156 |
57.8% |
|
|
Marital status |
|
|
<0.001 |
|
Married |
247 |
91% |
|
|
Single |
23 |
8.5% |
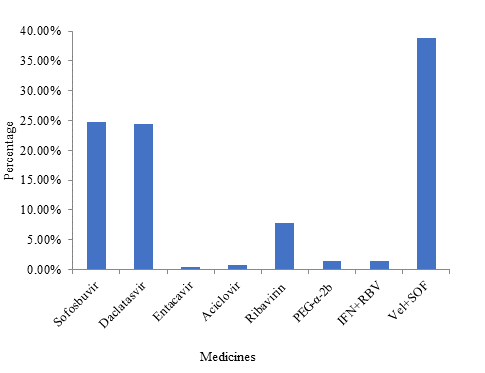
Figure 1. Prescription Trends
Figure 1 shows that physicians usually prescribed direct acting antivirals, namely sofosbuvir (24.8%), daclatasvir (24.4%), entacavir (0.4%), and aciclovir (0.7%). The usage ratio of ribavirin and PEG-alpha 2b was 7.8% and 1.5%, respectively. A combination of velpatasvir and sofosbuvir was prescribed with the highest ratio, that is, 38.9%. On the contrary, the usage ratio of the combination of interferon and ribavirin was only 1.5%, with p-value < 0.001.
Figure 2 shows that out of 270 patients, the trend of mono-therapy was 27.8% (n=75) and the percentage of combination drug was 8.8% (n=24) in patients of age less than 40 years. The trend of using a single drug was 34.1% (n=92) and of using combination drug was 29.3% (n=79) in patients of age above 40 years. The p- value was < 0.001.
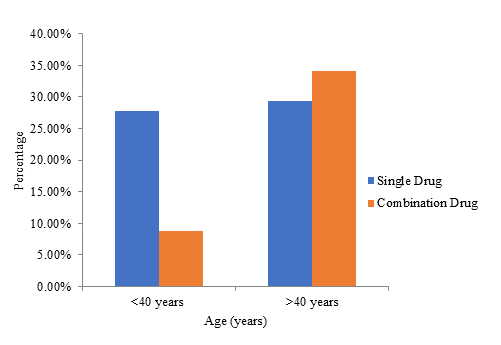
Figure 2. Trends of Using Combination Drugs among Different Age Groups
Table 2 depicts that HCV infection can become complicated with comorbid conditions. Out of 270 patients, 160 patients showed comorbidity. Among comorbid conditions, hypertension ranked first with 70 patients (58.5%) suffering from it. The second condition was diabetes with 58 patients suffering from it (25.9%), while anemia was observed in 32 patients (11.9%). On the comntary, 110 patients were free from any comorbidity, with p-value < 0.001.
Table 2. Comparison of Comorbidity
|
Sr. # |
Variables |
Number of Patients n=270 |
Percentage |
p-value |
|
1 |
Hypertension |
70 |
58.5% |
<0.001 |
|
2 |
Diabetes |
58 |
25.9% |
<0.001 |
|
3 |
Anemia |
32 |
11.9% |
<0.001 |
|
4 |
No disease |
110 |
40.7% |
<0.001 |
Figure 3 shows that out of 270 patients, 124 (45.5%) were housewives, 15 (5.6%) were government employes, 13 (4.8%) were farmers, 17 (6.3%) were buisnessmen, 29 (10.7 %) were teachers, 3 (1.1%) were mill workers, 2 (0.7%) were bankers, 6 (2.2%) were wholesalers, 51 (18.9%) were labourers, and 10 (3.7%) were students. The p-value was 0.522.
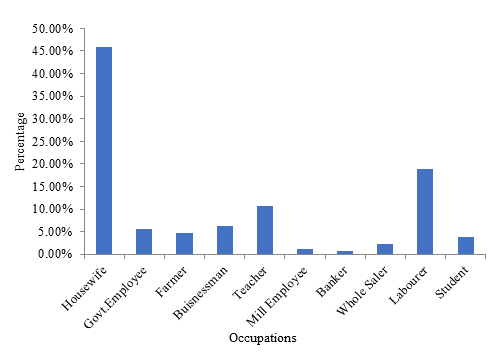
Figure 3. Occupational Distribution of HCV
Figure 4 shows the duration of HCV medication in the selected 270 patients. It shows that 167 (61%) patients had been receiving medication for 1 to 6 months, 38 (14.1%) patients for 6 months to 1 year, 28 (10.4%) patients for 1 to 2 years, 18 (6.7%) patients for 2 to 4 years, 8 (3%) patients for 4 to 5 years, and 11 (4.1 %) patients for 5 to 10 years. The p-value was < 0.123.
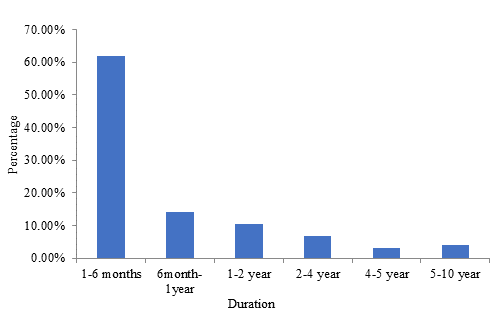
Figure 4. Duration of HCV Medication
Figure 5 depicts that patients receiving antiviral therapy were observed with several adverse effects (AEs). The most common AEs were weakness (19.6%), constipation (20.0%), dizziness (12.6%), fever (9.6%), and insomnia (9.6%). Mild AEs were bodyache (8.5%), allergic reactions (4.8%), nausea (5.2%), and headache (4.4%). Minor AEs were chills (2.2%), sores (0.4%), pale skin (1.9%), and shortness of breath (1.1%). The p-value was < 0.001.
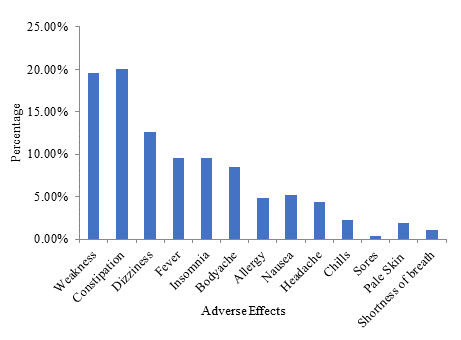
Figure 5. Adverse Effects (AEs) by HCV Regimen
Figure 6 depicts that 100 patients (37%) showed positive response towards family history and 170 patients (67%) had no family history of hepatitis C. The p-value was < 0.001.
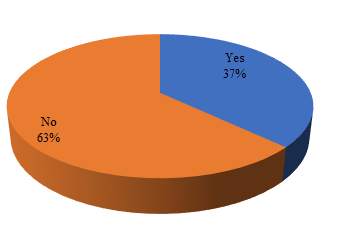
Figure 6. Family History
Figure 7 shows that 94.4% patients were satisfied with the medication therapy but 5.6% patients were not satisfied with it. The p-value was < 0.001.
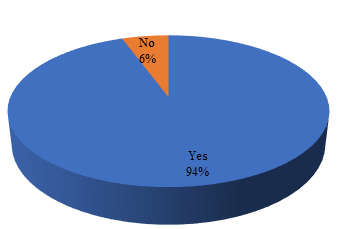
Figure 7. Level of Satisfaction
Figure 8 depicts that 233 patients (86.3%) responded that the medication of HCV is costly. Only 37 patients (13.7%) were not affected by the cost. The p-value was < 0.001.
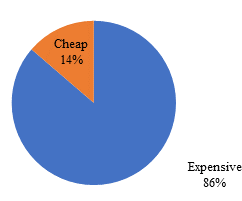
Figure 8. Cost of Therapy
The current study revealed that there is a significantly higher prevalence of hepatitis C among the age group of > 40 years as compared to the younger age group of < 40 years. Other studies also produced similar results [15–17]. These studies noted an increase in the prevalence of HCV with age.
The current study revealed that the prevalence of HCV was more common in female than male participants. A study conducted on 5543 patients found that the prevalence of HCV was higher in female (53.8%) than male (46.2%) patients. In contrast, another study found that the prevalence of HCV in male patients was higher (67.14%) than female (32.85%) patients during 2010-202[18].
The current study showed that HCV prevalence was higher in married individuals. The transmission of HCV in spouse may involve various factors, such as sex and sharing of households. The transmission of HCV via sex by Jacobson (2011) was supported previously by Osmond (1993), Piazza (1997), Vandelli (2004), and Tahan (2005) [19–23]. The possibility of non-sexual and non- parental household transmission involves the fact that HCV RNA was found in saliva, which is supported by Ackerman (1998) [24]. A study by Sood A in 2018 was conducted on 5543 patients, in which prevalence of HCV was higher in female (53.8%) than male (46.2%) [25]. In was in contrast to the observations of Maan MAl observations. In 2014, they have observed that prevalence of HCV in male is higher (67.14%) than female (32.85%) [18].
The current study also showed the highest comorbidity of HCV with hypertension, which is supported by the previous studies of Butt (2009) and Wong (2014) [26, 27]. Butt found that HCV infected patients have a higher risk of CAD as compared to HCV uninfected patients. Wong found a significantly higher prevalence of congestive heart failure in HCV infected patients. In contrast, Volzke (2004) found no significant association between HCV and cardiovascular disease events [28]. In the current study, comorbidity with diabetes was noticeable. Similar results were reported by Younas (2000) that diabetic patients, especially those with type 2 diabetes, are at a higher risk of catching HCV infection [29]. Comorbidity of HCV with anemia was also observed in the current study. An observational study reported that HFE gene mutation is more frequent in HCV patients and remains associated with increased iron storage in such patients [30]. In contrast, Thorburn (2002) performed liver biopsies on HCV infected patients and concluded that HFE mutation did not have a role in iron accumulation [31].
The current study showed that the use of the combination of velpatasvir and sofosbuvir is more common. Currently, data is not available in this regard, although a previous study showed that this combination is highly effective with SVR rates of 98-99% after 12 weeks of treatment [32].
The current study also revealed that adverse effects due to the antiviral therapy of hepatitis C are common. In this regard, the current study differs from the study conducted by Zamora in 2018 which reported the occurrence of fatigue (47.6%), GIT disturbance (38.1%), headache (14.3%), and dyspnea in only 2 patients [33].
World Health Organization (WHO) has set a target to treat 80% of HCV positive patients by 2030. The main treatment hurdle in many countries is the cost of medication therapy. In the current study, 86.3% of patients complained about the high cost of hepatitis C. Hill (2016) mentioned that the current price of sofosbuvir for a 12-week treatment is US$ 84000 in the USA, US$ 53000 in the UK, US$ 46139 in France, US$ 27921 in Spain and Portugal, US$ 7000 in Brazil, and US$ 483 in India [34]. Afzal (2017) stated that the price of 12-week treatment with generic sofosbuvir is around US$ 300 per month [35].
4.1. Conclusion
Progress has been made in the treatment of hepatitis C infection during the last few years, with considerable clinical efficacy and minimum adverse effects. However, the advantages of interferon free direct acting antivirals has been dampened by their extremely high cost. Most of the newly developed regimen needs to be cost effective. Widespread implementation of treatment is not affordable. Treatment and prevention of hepatitis C must become a national priority in Pakistan because one in every 20 Pakistanis is infected with this virus.