Emma Packer1, Sulaf Assi2, and Abdullah Al Hamid3*
1Faculty of Science and Technology, Bournemouth University, Bournemouth, United Kingdom
2Faculty of Science, School of Pharmacy and Biomolecular Sciences, Liverpool John Moores University, Liverpool, United Kingdom
3College of Clinical Pharmacy, Department of Pharmacy Practice, King Faisal University, AlAhsa, Saudi Arabia
*Corresponding Author: [email protected]
Asthma and Chronic Obstructive Pulmonary disease (COPD) have been classified as non-communicable diseases by the World Health Organization (WHO). These diseases contribute to the occurrence of around 4.2 million deaths globally. Medicine related problems (MRPs) refer to incidents associated with medicine therapy that interfere in the desired health outcomes. Patients with asthma and/or COPD are likely to encounter MRPs due to ineffective treatment, adverse drug reactions (ADRs), and/or medication errors (MEs). Therefore, the current study aimed to identify the prevalence, causes, and risk factors of MRPs among adult patients with asthma and/or COPD. A systematic literature review was conducted using 13 databases. These databases included PubMed, NELM, Embase, Scopus, ISI Web of Knowledge, ScienceDirect, PsycInfo, British Nursing Index, Global heath, International Pharmaceutical Abstracts, PsycExtra, and Cochrane Library. ‘Medicine related problems (MRPs)’ ‘adults’ ‘asthma’ ‘adverse drug reactions (ADRs)’ ‘drug related problems (DRPs)’ ‘adverse drug events (ADEs)’ ‘medication errors (MEs)’, and ‘Chronic Obstructive Pulmonary Disease’ ‘(COPD)’ were used as search items. Only quantitative studies, which investigated MRPs in adult patients with asthma and/or COPD, were included. The results of the review retrieved initially 1146338 titles that were considered. The analysis of the titles of these studies identified 55 relevant abstracts, of which, 15 were included in the review. The data extracted from these studies showed that the MRPs had a prevalence rate of 39.8%, ADRs 4.6%, while MEs had a prevalence rate of 66.9%. The comparison of these prevalence rates showed that MEs and MRPs had a higher prevalence than ADRs. Theophylline was reported to have the highest prevalence rate of MRPs which required special consideration to ensure its safe use by patients. The findings of the current study would potentially provide insights pertaining to the reduction of the high rate of MRPs.
Keywords: adults, asthma, Chronic Obstructive Pulmonary Disease (COPD), drug related problems (DRPs), medication errors (MEs)
Asthma causes inflammation and narrowing of the bronchial tube linings, resulting in reduced air flow in and out of the lungs. Globally, it has a higher prevalence rate with around 235 million cases. Asthma is prevalent in high-income countries; however, it causes more deaths in low and middle-income countries [1]. Approximately, 5.9% of the English population suffers from asthma which means that England has one of the highest prevalence rates for this disease in the world [2]. Asthma is a major cause of morbidity and mortality worldwide and also causes a considerable economic burden [3]. There is currently no cure for asthma. Instead, medicines are used to control the symptoms of asthma in patients [4].
Chronic Obstructive Pulmonary Disease (COPD), unlike asthma, is not a single disease. It is an umbrella term used to describe the diseases that cause chronic limitation to lung airflow. Chronic bronchitis and emphysema are among two of these diseases [5]. The main risk factors for COPD include smoking, pollution, and occupational dusts and chemicals. The major symptoms of COPD are breathlessness, a chronic cough, and an over production of mucus from respiratory tract [6]. This disease is under diagnosis. Research conducted in England has shown that the ratio between diagnosed cases and expected prevalence ranged between 0.20 and 0.95 [7]. COPD is also a respiratory disease with a higher prevalence. World Health Organization (WHO) has estimated that by 2030, COPD would be the third highest cause of deaths occurring globally [6]. Just like asthma, COPD is a disease that is incurable. Instead, a range of medicines are utilised in order to treat the symptoms of COPD [8].
Although, medicines are developed to treat diseases safely and effectively, it is still possible for medicines to cause unwanted effects or therapeutic failures [9]. Medicine Related Problems (MRPs) are therefore, an important issue for health care. Especially, since medicine therapy has become increasingly more complexed, the prevention of MRPs has also become more difficult. As MRPs are a part of pharmacovigilance, it is extremely important to understand them appropriately. Systematic reviews are one way through which the extent of MRPs effecting patient outcome can be assessed [10].
A problem with MRPs and their definition is that there is disagreement as to what can be classified as an MRP [9]. Some researchers consider medication error (ME) as an MRP, while others do not. A more up-to-date definition was produced by the PCNE [11]. PCNE defines MRPs as, “a drug-related problem is an event or circumstance involving drug therapy that actually or potentially interferes with the desired health outcomes”. MRPs are split into three categories, namely adverse drug reactions (ADRs), adverse drug events (ADEs), and medication errors (MEs). Table 1 shows the key definitions used in this review.
Table 1. Definitions of Keywords used in this Review
|
Term |
Definition |
Reference |
|
MRP |
“A drug-related problem is an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes”. |
[11] |
|
ADR |
A reaction “to a drug that is noxious, is unintended, and occurs as doses normally used in man”. |
[12] |
|
ME |
“An error in the process of prescribing, preparing, dispensing, administering, monitoring or providing advice on medicines”. |
[13] |
|
ADE |
An injury related to the use of a medicine that may not be causally related. |
|
|
Non-Adherence |
"The extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider". |
[16] |
|
Poly-pharmacy |
Can be defined as the use of five or more drugs. North Central London region hospitals use this definition. However, globally there is no agreed definition. Four or more drugs are also used. |
[17] |
|
Co-morbidities |
“Two or more coexisting medical conditions or disease processes that are additional to an initial diagnosis”. |
[18] |
|
Asthma |
Asthma is a chronic disease characterized |
[6] |
|
Asthma attacks |
“Recurrent attacks of breathlessness and wheezing” “the lining of bronchial tubes swell, causing the airways to narrow and reducing the flow of air into and out of the lungs”. |
[1] |
|
COPD |
“Chronic Obstructive Pulmonary Disease (COPD) is not one single disease. However, it is an umbrella term used to describe chronic lung diseases that cause limitations in lung airflow. The more familiar terms, that is, 'chronic bronchitis' and 'emphysema' are no longer used, however, they are now included within the COPD diagnosis. The most common symptoms of COPD are breathlessness, or a 'need for air', excessive sputum production, and a chronic cough. However, COPD is not just simply a "smoker's cough", but an under-diagnosed, life-threatening lung disease that may progressively lead to death”. |
[19] |
|
Cause |
“Usually refers to the behaviour that has caused the problem which is most often a medication error”. |
[20] |
|
Problem |
“The expected or unexpected event or circumstance that is, or might be wrong, in therapy with drugs”. |
[20] |
|
Elderly |
“At the moment, there is no United Nations standard numerical criterion, however, the UN agreed cut off to be 60+ years to refer to the older population”. “Most developed world countries have accepted the chronological age of 65 years as a definition of 'elderly' or older person”. To conduct the current research, 65+ shall be used to define elderly patients. |
[19] |
|
Adult |
For the purpose of this review, an adult was defined as any person of 16 years or older. |
Very limited evidence is available about the global prevalence of MRPs in asthma or COPD. Lewinski et al recorded a prevalence rate of 21% for MRPs in their study on a German population [21]. In US, there is a prevalence of MRPs ranging between 1.19% and 7.26% among nursing home residents [22]. However, further studies are required to fully understand the MRPs in asthma and COPD. Therefore, the current study aimed to identify the prevalence, causes, and risk factors of MRPs among adult patients with asthma and/or COPD.
A systematic review was conducted using 14 various databases. These databases included PubMed, Medline, National Electronic Library for Medicines, Embase, Scopus, ISI Web of Knowledge, Science direct, PshcInfo, British Nursing Index, Global Health, CINAHL, International Pharmaceutical Abstracts, PsychExtra, and Cochrane Library. The review produced relevant articles. The articles were critically reviewed to determine the prevalence, severity, preventability, causes, risk factors, and main medicine classes involved in MRPs. These results would identify the patterns and characteristics of MRPs.
2.1. Search Strategy
The search terms included ‘MRPs, ‘asthma’, ‘COPD’, and their analogues (Table 2). The hits produced for each database and term combination were recorded. The inclusion and exclusion criteria were then applied to the articles. The inclusion and exclusion criteria are given in detail, in sections 2.1.2 and 2.1.3. This produced the final articles used in the systematic review.
2.2. Search Terms
The search terms were classified into five main categories including MRPs, adults, and hospital disease review. The terms shown in Table 2, that is, ‘MRPs’, ‘adults’, ‘hospital’, ‘disease’, and ‘review’ along with their variations were used in a variety of different combinations.
Table 2. Search Terms used in Systematic Review
|
Term |
Variations |
|
Medicine Related Problems |
DRP(s) Drug Related Problem(s) (DRPs) MRP(s) Medicine Related Problem(s) ADR(s) Adverse Drug Reaction(s) ADE(s) Adverse Drug Event(s) ME(s) Medication Error(s) |
|
Adults |
Adult patient(s) Elderly Adult(s) |
|
Hospital |
Hospital admission Hospitalization(s) Hospitalisation(s) |
|
Disease |
Asthma COPD chronic obstructive pulmonary disease pulmonary disease(s) respiratory disease(s) |
|
Review |
Systematic review(s) Meta-analysis |
2.3. Inclusion Criteria
Articles were included if:
It is also important to note that articles were included with no language restrictions.
2.4. Exclusion Criteria
Articles were excluded if:
2.5. Data Extraction
The number of articles produced by this systematic review are described in the results. Once the articles were found, each one was read and the information was extracted and tabulated. The classification for DRPs’ report by the PCNE was read as guidance for the classification of problems and causes [20].
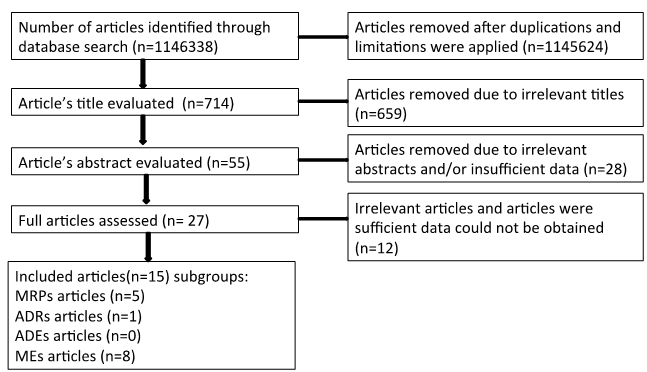
In total, the search yielded 11,46338 articles before applying limitations of age group (≥ 16 years old) (Figure 1). Studies investigating in other languages other than English were translated into English using a back-translation technique. Subsequently, 714 were obtained and their titles were evaluated. This resulted in 55 articles determined as relevant. The remaining articles were assessed from the abstract and 28 were excluded. This resulted in 27 articles, which were assessed in full, and 12 were excluded. Consequently, the search resulted in 15 relevant articles, which were included in the current study and comprised of five MRPs, one ADR, zero ADE, and eight MEs.
Figure 1. Data Extraction and Article Selection Process
3.2. Demographics
Of the 13 studies that reported MRPs, nine different countries had research conducted there (Table 3). They are as follows: Nigeria [23], Australia [24], Canada [25, 26], Japan [27–29], Italy [30], Saudi Arabia [31], USA [32, 33], Sweden [34] and Spain [35]. Japan published most of the articles. The average age in the studies ranged from 22 years [34] to 72 years [26]. The average age of all studies was 46.3 years. The results of two studies also did not report/the mean age. Only two studies gave age ranges, 16-83 [29] and 20-78 [35].
Three studies reported education levels. Al-Jahdail et al. [31] determined that most participants acquired education till high school level. In contrast, Axelsson et al. [34] determined that the vast majority of participants were educated above compulsory level. Barrueco et al. [35] did not report only quantitative results, however, only mentioning lower education levels can be problematic.
Two studies had data on occupation. Unfortunately, Abramson et al. [24] reported that 11.8% of the sample was unemployed. However, Axelsson et al. [34] was much more detailed. According to the report, 4.1% had compulsory education, 50.4% had grammar/high school education, and 45.5% had college/university education.
Ethnicity was only reported by two studies. Press reported that 5% of the population had Hispanic or Latino ethnicity [32]. Spitz [33] conducted a case study on a black female.
Table 3. Demographics of the Articles Populations
|
Study ID |
Country |
Average age (Years) |
Age |
Gender |
Education level |
Occupation |
Ethnicity |
|
[23] |
Nigeria |
39 |
≥18 |
Males 32% |
NR |
NR |
NR |
|
[24] |
Australia |
38.2 |
≤60 |
Males 54.9% |
NR |
Unemployed 11.8% |
NR |
|
[25] |
Canada |
82 |
≥66 |
Males 51.9% |
NR |
NR |
NR |
|
[26] |
Canada |
72 |
72 |
Males 56.8% |
NR |
NR |
NR |
|
[27] |
Japan |
57.4 |
≥16 |
Males 42.8% |
NR |
NR |
NR |
|
[30] |
Italy |
NR |
≥ 16 years |
Males 53.3% |
NR |
NR |
NR |
|
[28] |
Japan |
57 |
≥ 16 years |
Males 42.5% |
NR |
NR |
NR |
|
[31] |
Saudi |
42.3 |
NR |
Males 39.1 |
University 13.8% |
NR |
NR |
|
[36] |
USA |
51.7 |
NR |
Male 27% |
NR |
NR |
Hispanic or |
|
[36] |
USA |
64.6 |
NR |
Male 35% |
NR |
NR |
Hispanic or |
|
[36] |
USA |
43.1 |
NR |
Male 22% |
NR |
NR |
Hispanic or |
|
[34] |
Sweden |
22 |
22 |
Males 38.4% |
Compulsory school 4.1% |
Employee 44% |
NR |
|
[29] |
Japan |
45 |
16-83 |
Males 47.3% |
NR |
NR |
NR |
|
[35] |
Spain |
NR |
20-78 |
Males 68% |
Low education level |
NR |
NR |
|
[33] |
USA |
35 |
35 |
Males 0% |
NR |
NR |
Black |
This systematic review evaluated the prevalence, severity, and preventability of MRPS, ADEs, ADRs, and MEs.
3.4. Medicine Related Problems (MRPs)
Five studies investigating MRPS were identified [23–27] (Table 4). The studies identified MRPs, such as increasing obesity in patients using medicines [27], patients suffering from pneumonia caused by the medicine, and adverse effects on the oropharynx [26]. Abramson et al. [24] identified therapeutic failure occurring in asthmatic patients, causing deaths. Desalu et al. [23] studied MRPs in general, as did Stephenson et al. [25].
Three of the studies’ populations suffered from asthma [23, 24, 27], while the remaining two studies included patients with COPD [25, 26]. The range of sample sizes in the five studies could be considered very large ranging from 100 participants to 18 million. The major difference in sample size was between the studies collecting data via questionnaires [23, 24, 26, 27] with sample sizes ranging between 100 and 3146. The only study that utilized data from medical records had a significantly larger sample size, that is, 18 million [25].
The duration of studies ranged from two months [27] to 84 months [25]. MRPs were identified in four countries, that is, Canada [25, 26], Nigeria [23], Australia [24], and Japan [27]. Of the references, one was classified as a prospective study [23], while the other references [24–27] were classified as retrospective studies.
The mean prevalence rate of MRPs was calculated to be 39.8%. The prevalence rate ranged between 3.2 [25] and 86% [26]. Unfortunately, the severity of MRPs was not reported in any of the five studies.
All the studies that reported MRPs gave a form of definition [23–25, 27]. However, many studies did not provide a clear definition of ‘MRPS’. Desalu et al. [23] simply stated the side effects as either short or long-term. Abramson et al. [24] used ‘asthma as the cause of death’ to indicate the therapeutic failure. Stephenson et al. [25] investigated cholinesterase inhibitors and spoke about how an adverse respiratory event could occur in the form of bronchoconstriction. Suissa et al. [26] had a similar approach, only defining a serious pneumonia event. Youkou et al. [27] is another example of this. Obesity was defined using the definition produced by the Japan Society of the Study of Obesity.
Table 4. Characteristics of Studies that Investigated Medicine Related Problems (MRPs)
|
Study ID |
MRP |
Country |
Settings |
Population |
Definition |
Duration |
Sample |
Prevalence |
Severity |
|
[23] |
MRPs |
Nigeria |
Cross sectional study Questionnaire study |
Adults mean age 39 (≥18 years), diagnosed with asthma for a minimum of 6 months |
Long term side effects or Short term side effects |
6 |
150 |
30.7 |
NR |
|
[24] |
Therapeutic |
Australia |
Case-control survey Victorian registry |
Adults mean age 38 years(≤60 years), diagnosed with acute asthma |
Asthma is the cause of death |
24 |
332 |
27.6 |
NR |
|
[25] |
MRPs |
Canada |
Cohort study data from Institutes for clinical evaluative sciences Danepezil Galantamine Rivastigmine |
Adults mean age 82 (≥66 years), |
Bronchoconstriction |
84 |
18000000 |
3.2 |
NR |
|
[26] |
Pneumonia |
Canada |
Case control survey Qubéc |
Adults (72 years), diagnosed with COPD using International classification of diseases |
A serious pneumonia |
30 |
100 |
86 and 71 |
NR |
|
[27] |
Obesity |
Japan |
Survey Data from hospitals in Niigata Prefecture |
Adults (≥16 years) diagnosed with Bronchial asthma |
Japan Society for the Study of Obesity (JASSO) 25kg/m^2 ≤BMI |
2 |
3146 |
20 |
NR |
Table 5. Characteristics of Studies that Investigated Adverse Drug Reactions (ADRs)
|
Study ID |
ADR |
Country |
Settings |
Population |
Definition used |
Duration of study (months) |
Sample size |
Prevalence rate (%) |
Severity (%) |
|
[30] |
Type A: usually predictable including medicine interactions Type B: usually not predictable including intolerance to a specific medicine |
Italy |
Clinical records review |
Adults (≥ 16 years) diagnosed with either asthma or COPD |
Untoward clinical manifestation consequent to and caused by the administration of a particular drug or interacting drugs including accidental overdose substance abuse and therapeutic failure. |
83 |
5183 |
4.6 |
28 |
3.5. Adverse Drug Reactions (ADRs)
One study investigating ADRs was included in this systematic review. This retrospective study analysed the clinical records and used the frequency of bronchodilators [30] (Table 5). The study used a clinical records review as the research design. The research was conducted over an 83-month time span in Catanzaro, Italy. Two hospitals were used, namely Italy Mater Domini University Hospital Pugliese and Ciaccio Hospital. About 5183 clinical records of adult patients, who were 16 years or older, with a diagnosis of either asthma or COPD, were reviewed. This produced a prevalence rate of 4.6% and an MRP severity of 28%. Preventability was not reported in this case.
3.6. Adverse Drug Events (ADEs)
This systematic review did not find any studies that reported ADEs.
3.7. Medication Error (ME)
This review yielded eight studies (Table 6). The MEs identified in these studies include non-adherence [23, 29, 31, 34–35], prescribing error [28, 33], and patients not using the correct technique for their inhaler device [31, 32]. By far, the most prevalent ME was non-adherence. Five of the eight studies recorded this as an ME. The studies were conducted in six countries. These countries include Nigeria [23], Japan [28, 29], Saudi Arabia [31], USA [32, 33], Sweden [34], and Spain [35]. The studies identifying MEs had a variety of methods. Four studies collected the data by reviewing clinical records [29, 31, 34, 35]. Two studies conducted surveys of patients in order to produce results [23, 28]. One reference used interviews [31] along with clinical record review. Finally, Spitz [33] used a case study. The range of sample sizes as was the case with MRPs was broad. This range was between 50 [29] and 3000 [28] with a mean of 57. However, a case study used one patient [33]. The included researches used three types of study designs, that is, prospective [23, 28], observational studies [31], and retrospective [29, 33–35]. Only two studies used patients suffering from COPD [32, 35]. While, seven studies comprised populations of patients suffering from asthma [23, 28], Press et al. [32, 29, 33, 34]. The age of participants included in the studies was difficult to analyse. Some studies reported average age, while others reported the age range. The average prevalence rate was 66.9% with a range of 10%-94.6% [29, 34]. Severity and preventability went unreported in all cases.
Table 6. Characteristics of Studies that Investigated Medication Error (ME), see appendix 3 for Abbreviations
|
Study ID |
Medication error |
Country |
Settings |
Population |
Definition used |
Duration |
Sample |
Prevalence |
Severity |
|
Prospective studies |
|||||||||
|
[23] |
Non-adherence |
Nigeria |
Cross sectional study (questionnaires) |
Adults mean age of 39 (≥18 years), diagnosed with asthma for a minimum of 6 months |
NR |
6 |
150 |
81.3 |
NR |
|
[28] |
Prescribing error |
Japan |
Questionnaire survey All medical institutions in Nigata |
Adults (≥16 years), diagnosed with bronchial asthma |
NR |
240 |
3000 |
N/A |
NR |
|
Observational studies |
|||||||||
|
[31] |
Incorrect inhaler technique |
Saudi |
Cross-sectional study (interviews and review of clinical records) |
Adults mean age 42 years diagnosed by physician with asthma |
Poor asthma control |
9 |
450 |
59.1 |
NR |
|
[36] |
Incorrect inhaler technique |
USA |
Cross-sectional study |
Adults mean age 51 years hospitalized with asthma n=60 or COPD n=40 |
MDI: 12 item checklist Diskus: 10 item checklist |
30 |
100 |
MDI:86 |
NR |
|
Retrospective studies |
|||||||||
|
[34] |
Non-adherence, measured using the |
Sweden |
Clinical records review |
Adults 22 years old diagnosed with asthma and prescribed regular asthma medication |
NR |
NR |
268 |
94.6 |
NR |
|
[29] |
Non-adherence |
Japan |
Clinical records review |
Adults mean age 45 years admitted to hospital with asthma |
Medication adherence report scale (MARS) a five-item self-report scale |
71 |
112 |
10 |
NR |
|
[35] |
Non-adherence |
Spain |
Clinical records review |
Adults (20-78 years) who have had COPD for more than 5 years |
Incorrect use of treatment |
NR |
50 |
66 |
NR |
|
[33] |
Prescribing error |
USA |
Case study Pulmonary divisions Catanzaro Italy |
Female 35 years of age with bronchial asthma |
NA case study |
NA |
1 |
NA |
NR |
Of the 15 included studies, four identified comorbidities associated with MRPS [24-26, 29] (Table 7). Of these, two reported COPD to be a comorbidity of asthma [24, 29]. Baba et al. [29] reported the only secondary diagnosis of the review, which was airway infection, when asthma was the primary diagnosis. The comorbidities reported for COPD included dementia [25], cardiac diseases, diabetes, Parkinsons, and depression [26]. Comorbidities would appear to occur more frequently in older patients as Stephenson et al. [25] and Suissa et al. [26] had older populations in their research.
Table 7. Comorbidities Reported by Studies that Investigated MRPs, ADRs, ADEs, and MEs
|
Study ID |
Population |
Main diagnosis |
Secondary |
Number of comorbidities |
Comorbidities |
|
[24] |
Adults mean age 38 years, diagnosed with acute asthma |
Asthma |
NA |
1 |
COPD |
|
[29] |
Adults mean age 45 years admitted to hospital with asthma |
Asthma |
Airway infection |
1 |
COPD |
|
[25] |
Adults mean age 82 (≥66 years), diagnosed with COPD and dementia |
COPD |
NA |
1 |
Dementia |
|
[26] |
Adults (≥72 years), diagnosed with COPD using International classification of diseases |
COPD |
NA |
4 |
Cardiac disease Diabetes Parkinson's Depression |
The underlying causes of MRPs were reported by nine included studies [28, 29, 31, 33, 34] (Table 8). The main cause of MRPs was identified to be the lack of information with five studies reporting this as a cause [29], Al-Jahdali et al. [23, 31, 32, 35]. Logistics and the patients themselves were both reported twice in Spitz [33], Barrueco et al. [35] and Desalu et al. [23], Axelsson et al. [34], respectively. Guidelines [28], use [31], dose [35], and treatment effectiveness [24] were all reported once. Three studies reported that MRPs had unknown causes [23, 26, 27]. Gallelli et al. [30] had a cause classified as ‘other’.
The problems associated with MRPs were reported by 12 of the 15 studies. These problems include dosing problems [29, 31], medicine choice problems [28], medicine use problems [33], adverse reactions [23, 26, 27, 30] less drugs taken than required [35], therapeutic failures [24], and treatment effectiveness [23, 32]. Of the problems found in this review, adverse reactions were the most frequently occurring problem.
Gallelli et al. [30] found through clinical records review that bronchodilators caused adverse reactions that were non-allergic side effects. These included cutaneous (47.7%), gastrointestinal (15.6%), and cardiovascular (15.2%). Gallelli et al. [30] was classified as other as there was no obvious cause. Youkou et al. [27] found that the MRP obesity caused problems, such as decreased inhaled corticosteroid therapy efficacy and leaukotroine related inflammation. Desalu et al. [23] reported that patients suffered from side effects. This, in itself, is a problem, while the cause of these side effects went unreported. Dosing problems were reported by Baba et al. [29] and Al-Jahdali et al. [31].
Al-Jahdali et al. [31] investigated inhaler technique in asthmatic patients and reported that 45% of patients did not use their inhalers appropriately. Furthermore, it was reported that 50.9% of patients who did not use their inhaler correctly visited A and E more than three times. About 51.6% of patients had no formal asthma education and 40.7% had no formal education about their medications or inhaler devices.
Researchers determined that patients did not have basic information about their medicine and did not receive written instructions regarding the intake of their medicine as well. It was supported by the findings of a study that lack of information is the cause of ME [32]. It was reported that patients were unable to use their inhaler correctly attributing to the lack of awareness about correct inhaler technique.
Table 8. Problems and Causes of Medicine Related Problems (MRPs)
|
References |
Problem |
N |
Causes |
|
[29] |
Dosing problem |
1 |
Information |
|
[34] |
NA |
1 |
Patient |
|
[28] |
Medicine choice problem |
1 |
Not following guidelines |
|
[31] |
Dosing problem |
2 |
Medicine use process Information |
|
[33] |
Medicine use problem |
1 |
Logistics |
|
[30] |
Adverse reactions |
0 |
Other |
|
[35] |
Less drug than required |
3 |
Dosage level Logistics Information |
|
[24] |
Therapeutic failure |
1 |
Treatment effectiveness |
|
[26] |
Adverse reactions |
0 |
Unknown |
|
[36] |
Treatment effectiveness |
1 |
Information |
|
[27] |
Adverse reactions |
0 |
Unknown |
|
[23] |
Adverse reactions |
0 |
Unknown |
|
[23] |
Treatment effectiveness |
2 |
Information Patient |
3.10. Risk Factors
Eight of the included studies identified some risk factors for MRPs (Table 9). These 16 identified risk factors included excessive smoking [24, 34], age [24, 28, 29] gender [24, 28, 29], family problems, excessive alcohol intake, family history, personality [24], non-adherence, comorbidities [29], socio economic status [35], symptoms severity [35], ethnicity [37, 38] duration of disease [28], dose [38], education, and obesity [32]. In general, age, gender, and socioeconomic status were identified as major risk factors. Many studies found that male patients, older patients, patients with a lower socio-economic background, and patients from a less awareness about their medicine and diseases were more likely to have MRPs.
Table 9. Present Risk Factors of MRPs, ADRs, ADEs, and MEs as reported by included Studies
|
References |
N |
Risk factors |
|
[24] |
6 |
excessive smoking age |
|
[34] |
2 |
excessive smoking personality |
|
[29] |
5 |
non-adherence gender age |
|
[35] |
4 |
socio economic status |
|
[37] |
2 |
ethnicity socio economic status |
|
[28] |
3 |
chronic diseases age gender |
|
Hedberg and Rossner |
2 |
gender obesity |
|
[38] |
3 |
gender ethnicity dose |
|
[36] |
1 |
healthcare education |
The current systematic review aimed to identify the prevalence, causes, and risk factors of MRPs among adult patients with asthma and/or COPD. MRPs had a prevalence rate of 39.8%, ADRs 4.6%, while ME had a prevalence rate of 66.9%. The comparison of these prevalence rates showed that MEs and MRPs have a higher prevalence rate than ADRs. Severity and preventability were not reported accurately in many studies. The findings potentially provided insight to reduce the higher rate of MRPs.
Theophylline was reported to have the highest prevalence of MRPs which requires special consideration to ensure its safe use by patients. Theophylline has quite a narrow therapeutic index and its interactions with a number of other medicines has limited its use. The serum concentrations of theophylline require close and regular monitoring to limit the toxicity and adverse effects of theophylline including life-threatening arrhythmias [39]. All healthcare professionals involved in prescribing, dispensing, and administration of this medication should be familiar with its adverse effects’ profile. Pharmacists who are the medicine experts should clinically verify the prescriptions of theophylline and provide counselling to patients about the adverse effects of this medication. Given the availability of other bronchodilators with better safety profile, the use of theophylline should be limited.
This review suggests that MRPs seem to be mainly related to MEs, especially non-adherence. Non-adherence is a complex research area since the causes are so complex. More research on the causes of non-adherence coupled with presentation of effective strategies would help address this issue. Moreover, it would also improve patient health outcomes. Weinstien 2004 demonstrated that non-adherence was associated with polypharmacy, comorbidities, anxiety, and expensive medicines. This is similar to the findings of this review which found polypharmacy and individual patient as causes for non-adherence. However, this review extended medicine characteristics beyond polypharmacy. It reported that medicines with narrow therapeutic margins and short time intervals between doses also contributed to non-adherence. On the contrary, review by Lindsay and Heaney reported that treatment type did not impact non-adherence. Half of the studies included in this review reported that male gender was a risk factor of MRPs, while the remaining studies linked female gender with MRPs. Lindsay and Heaney also reported similar findings. Other risk factors of MRPs included old age and poor socio-economic backgrounds [40].
The comparison of this systematic review with the previous systematic reviews showed that a review of all MRPs in asthma and COPD had not previously been attempted.
Furthermore, there is a need for good quality reviews that clearly report their search strategy [41]. While, this systematic review included all types of study designs and did not apply any language restrictions to make the findings comprehensive, it had some limitations. Using two researchers instead of one would have improved the quality as it would decrease bias in the selection of articles. Another limitation of this systematic review is the limited inclusion of studies investigating COPD. Furthermore, the included studies did not provide clear definitions of MRPs. This could have potentially decreased the accuracy of this review.
Despite the above-mentioned limitations, this review has several strengths. Using a narrative review would not be as appropriate, since systematic reviews are better at assessing the current literature. Systematic reviews are also a more scientific way of reviewing the literature to produce more valid results. The review unlike many other reviews, included all studies regardless of the language. This potentially means that this review would have assessed information previously missed by other reviews.
Further research with the inclusion of qualitative studies together with the inclusion of data about hospitalised patients is required. Since MRPs are considered to differ depending on the clinical setting [42], separating the data into clinical setting type would lead to dissemination of useful information.
4.1. Conclusions
This systematic review aimed to investigate MRPs in adult patients with asthma or COPD. The findings suggested that MEs and MRPs have a higher prevalence than ADRs. Theophylline was reported to have the highest prevalence of MRPs and requires special consideration to ensure its safe use by patients.
1. World Health Organisation. Chronic respiratory diseases: asthma. http://www.who.int/respiratory/asthma/en/. Updated May 3, 2021.
2. Department of Health. An outcomes strategy for chronic obstructive pulmonary disease (COPD) and asthma in England. https://assets.publishing.service.gov.uk/media/5a7cc010e5274a2f304efd6e/dh_128428.pdf. Updated July 2011.
3. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA dissemination committee Report. Allergy. 2004;59(5):469–478. https://doi.org/10.1111/j.1398-9995.2004.00526.x
4. Hon KLE, Leung TF, Leung AKC. Clinical effectiveness and safety of montelukast in asthma. what are the conclusions from clinical trials and meta-analyses? Drug Des Devel Ther. 2014;8(1):839–850. https://doi.org/10.2147/DDDT.S39100
5. World Health Organisation. Chronic obstructive pulmonary diseases (COPD). https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd). Updated March 16, 2023.
6. May SM, Li JT. Burden of chronic obstructive pulmonary disease: healthcare costs and beyond. Allergy Asthma Proc. 215;36(1):4–10. https://doi.org/10.2500/aap.2015.36.3812
7. Nacul L, Soljak M, Samarasundera E. COPD in England: a comparison of expected, model-based prevalence and observed prevalence from general practice data. J Pub Health. 2010;33(1):108–116. https://doi.org/10.1093/pubmed/fdq031
8. Slot AHM, ‘t Veen JCCM, Chavannes NH, et al. Effectiveness of the assessment of burden of chronic obstructive pulmonary disease (ABC) tool: study protocol of a cluster randomised trial in primary and secondary care. BMC Pulmon Med. 2014;37(1):5–14. https://doi.org/10.1186/1471-2466-14-131
9. Fernandez-Llimos F, Faus MJ, Gastelurrutia MA, Baena I, Martínez-Martínez F. Evolution of the concept of drug-related problems: outcomes as the focus of the new paradigm. Pharm Prac. 2005;3(4):167–188.
10. Souza TT, Saez-Benito L, Correr CJ, Fernandez-Llimos F. Critical assessment of the systematic review on hospitalization resulting from medicine related problems. Br J Clin Pharmacol. 2014;78(6):1465–1466. https://doi.org/10.1111%2Fbcp.12461
11. Pharmaceutical Care Network Europe. Classification for drug related problems. https://www.pcne.org/upload/files/417_PCNE_classification_V9-1_final.pdf. Updated May 2020.
12. World Health Organisation. International drug monitoring: the role of national centres Report of a WHO Meeting. https://who-umc.org/media/2680/who-technical-report-498.pdf. Updated 1972.
13. National Health Service England. Improving medication error incident reporting and learning. http://www.england.nhs.uk/wp-content/uploads/2014/03/psa-med-error.pdf. Accessed November 23, 2014.
14. van den Bemt PM, Egberts TC, de Jong-van den Berg LT, Brouwers JR. Drug-realted problems in hospitalised patients. Drug Safety. 2000;22(4):321–333. https://doi.org/10.2165/00002018-200022040-00005
15. World Health Organisation. Essential medicine and health products. http://www.who.int/medicines/areas/quality_safety/safety_efficacy/pharmvigi/en/. Accessed April 22, 2015.
16. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
17. Banerjee A, Mbamalu D, Ebrahimi S, Khan AA, Chan Foo T. The prevalence of polypharmacy in elderly attenders to an emergency department – a problem with a need for an effective solution. Int J Emer Med. 2011;4(1):e22. https://doi.org/10.1186/1865-1380-4-22
18. Mosby.Mosby's Dictionary of Medicine, Nursing, & Health Professions. Elsevier Health Sciences; 2012.
19. World Health Organisation. Definition of an elderly person http://www.who.int/respiratory/copd/burden/en/. Accessed November 20, 2014.
20. Pharmaceutical Care Network Europe. Classification for drug related problems (revised 14-01-2010vm) V6.2. https://www.pcne.org/upload/files/11_PCNE_classification_V6-2.pdf. Updated January 1, 2010.
21. Lewinski D, Wind S, Belgardt C, Plate V, Behles C, Schweim HG. Prevalence and safety-relevance of drug-related problems in German community pharmacies. Pharmacoepidemiol Drug Saf. 2010;19(2):141–149. https://doi.org/10.1002/pds.1861
22. Handler SM, Wright RM, Ruby CM, Hanlon JT. Epidemiology of medication-related adverse events in nursing homes. Am J Geriat Pharmacoth. 2006;4(3):264–272. https://doi.org/10.1016/j.amjopharm.2006.09.011
23. Desalu OO, Onyedum CC, Adeoti AO, et al. Unmet needs in asthma treatment in a resource-limited setting: Findings from the survey patients and their physicians in Nigeria. PanAfrican Med J. 2013;16(1):e20. https://doi.org/10.11604/pamj.2013.16.20.2798
24. Abramson MJ, Bailey MJ, Couper FJ, et al. Are asthma medications and management related to deaths from asthma? Am J Resp Critical Care Med. 2001;163(1):12–18. https://doi.org/10.1164/ajrccm.163.1.9910042
25. Stephenson A, Seitz DP, Fischer HD, et al. Cholinesterase inhibitors and adverse pulmonary events in older people with chronic obstructive pulmonary disease and concomitant dementia. Drugs and aging. 2012;29(3):213–223. https://doi.org/10.2165/11599480-000000000-00000
26. Suissa S, Patenaude V, Lapi F, Emst F. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68(11):1029–1036. https://doi.org/10.1136/thoraxjnl-2012-202872
27. Youkou A, Hasegawa T, Suzuki K, et al. Influence of obesity on control in asthmatic Japanese patients defined by the Japanese definition of obesity. Int Med. 2011;50(1):1911–1916. https://doi.org/10.2169/internalmedicine.50.5474
28. Hasegawa T, Koya T, Sakagami T, Toyabe S, et al. Asthma control and management changes in Japan: Questionnaire Survey. Int Med. 2012;51(1):567–574. https://doi.org/10.2169/internalmedicine.51.6586
29. Baba K, Hattori T, Yagi T, et al. Adherence with long-term asthma management in patients who experienced hospitalized asthma exacerbation. Allergol Int. 2009;58(2):217–224. https://doi.org/10.2332/allergolint.08-OA-0012
30. Gallelli L, Ferreri G, Colosino M, et al. 2002. Retrospective analysis of adverse drug reactions to bronchodilators observed in two pulmonary divisions of Catanzaro, Italy. Pharmacol Res. 2002;47(6):493–499. https://doi.org/10.1016/S1043-6618(03)00003-3
31. Al-Jahdali H, Ahmed A, Al-Harbi A, et al. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clinic Immunol. 2013;9(1):e8. https://doi.org/10.1186/1710-1492-9-8
32. Press VG, Arrora VM, Shah LM, et al. Misuse of respiratory inhalers in hospitalised patients with asthma or COPD. J Gen Intern Med. 2011;26(6):635–642. https://doi.org/10.1007/s11606-010-1624-2
33. Spitz DJ. An unusual death in asthmatic patient. Am J Foren Med Pathol. 2003;24(3):271–272. https://doi.org/10.1097/01.paf.0000083522.05957.61
34. Axelsson M, Emilsson M, Brink E, Lundgren J, Torén K, Lötvall JJ. Personality, adherence, asthma control and health-related quality of life in young adult asthmatics. Respir Med. 2009;103(7):1033–1040. https://doi.org/10.1016/j.rmed.2009.01.013
35. Barrueco M, Otero MJ, Ferández DGM, et al. Theraputic non-compliance in patients with chronic airway obstruction. Rev Clín Esp. 1987;180(6):293–295.
36. Díaz AA, Celli B, Celedón JC. Chronic obstructive pulmonary disease in Hispanics. A 9-year update. Am J Respir Critical Care Med. 2018;197(1):15–21. https://doi.org/10.1164/rccm.201708-1615PP
37. Gilthorpe MS, Lay-Yee R, Wilson RC, Walters S, Griffiths RK, Bedi R. Variations in hospitalization rates for asthma among Black and minority ethnic communities. Respir Med. 1998;92(1):642–648. https://doi.org/10.1016/S0954-6111(98)90511-X
38. Shireman TI, Heaton PC, Gay WE, Cluxton RJ, Moomaw CJ. Relationship between asthma drug therapy patterns and healthcare utilization. Anal Pharmacoth. 2002;36(4):557–564. https://doi.org/10.1345/aph.1A067
39. Lal D, Manocha S, Ray A, Vijayan VK, Kumar R. Comparative study of the efficacy and safety of theophylline and doxofylline in patients with bronchial asthma and chronic obstructive pulmonary disease. J Basic Clin Physiol Pharmacol. 2015;26(5):443–451. https://doi.org/10.1515/jbcpp-2015-0006
40. Lindsay JT, Heaney LG. Nonadherence in difficult asthma – facts, myths, and a time to act. Patient Pref Adher. 2013;7(1):329–336. https://doi.org/10.2147/PPA.S38208
41. Jadad AR, Moher M, Brownman GP, et al. Systematic reviews and meta-analyses on treatment of asthma: critical evaluation. Brit Med J. 2000;320(1):537–540. https://doi.org/10.1136/bmj.320.7234.537
42. Wilt TJ, Niewoehner D, MacDonald R, Kane RL. Management of stable chronic obstructive pulmonary disease: a systematic review for a clinical practice guideline. Anal Inter Med. 2007;147(9):639–653. https://doi.org/10.7326/0003-4819-147-9-200711060-00009