Formulation and Clinical Evaluation of a Novel Polyherbal Anti-Acne Cream
Asma Manzoor1*, Uzma Niaz2, and Syed Atif Raza2
1School of Pharmacy, University of Management and Technology, Punjab, Lahore, Pakistan
2Punjab University College of Pharmacy, University of the Punjab, Lahore, Pakistan
Abstract
Natural skin products are safer and more acceptable in the management of various skin diseases. Hence, there has been a shift towards natural products owing to the adverse effects of synthetic medicinal agents. Acne vulgaris is the disorder which occurs mostly through pilosebaceous unit. It is caused by whether, hormonal, microbiological, and immunological factors. The disorder impacts people of all age groups, with the highest prevalence in teenagers (aged 13-19 years) (85%), followed by those aged 25-34 years (8%), and 3% in then individuals aged 35-44 years (3%). This disorder is characterized by the presence of the bacteria Staphylococcus aureus, Staphylococcus epidermidis, and Propionibacterium acnes. This skin disease becomes worse with the passage of time and with age. The current study was aimed to formulate three different combinations (F1, F2, and F3) of anti-acne cream containing alcoholic tinctures of Azadirachta indica, Glycyrrhiza glabra, Calendulla officinalis, Echinacea angustifolia Aloe socotrina, Rumex crispus, Symphytum officinale, Thuja occidentalis, and Ginseng panax. Their subsequent evaluation on human subjects was aimed to estimate their efficacy in the management of acne. The clinical efficacy of the formulated polyherbal cream containing alcoholic tinctures and non-comedogenic ingredients was established in this prospective randomized study on 60 human volunteers. The results obtained were statistically significant and revealed the efficacy of the tested formulation, which reduced the acne after 4 weeks of application. Additionally, 70% of participants reported visible improvement in skin texture, while 55% showed a significant reduction in associated inflammation and redness. These findings support the efficacy of the tested formulation in managing AV.
Introduction
The most common disease of the skin is acne vulgaris. The symptoms usually appear at adolescence and become severe at the age of 14 to 19 years [1]. Acne vulgaris is a chronic inflammatory condition that typically develops earlier in women than in men [2]. It is frequently associated with other skin disorders or conditions including cystic acne, nodular acne that can lead to permanent scarring, often affecting the chest and back [3], Acne Conglobate (AC), a chronic, widespread acne with abscesses, commonly seen in men [3], Post-Inflammatory Hyperpigmentation (PIH) characterized by dark spots that develop after acne heals, prevalent in darker skin tones [4], and Pyoderma facials, which is limited to the face and primarily affects young women [3]. Due to the long-term treatment time of products causing significant side effects, the usual methods used for the treatment of acne including the topical application of drug, oral medication, or systemic antibiotics or retinoids have become less effective. This is because these treatments can cause various side effects including the burning and drying of the skin, erythema, nausea and gastric problems, and peeling of skin. So, to overcome this condition, there is a need to develop therapeutic modalities which may include herbal therapies or any other alternative medicinal system [5]. Many antibiotics and chemotherapeutic agents are applied topically or taken orally, such as benzoyl peroxide, erythromycin, clindamycin, and tetracycline to control the bacteria. Currently, on the basis of clinical type and severity, acne is treated either by monotherapy or by combination therapy with chemotherapeutic agent [6]. The currently available treatments have many unwanted side effects, such as skin dryness, puritis, burning sensation, occasional hyperpigmentation, erythema, local irritation, and photosensitization [7].
Keeping in view the above, the current study was conducted to validate the safety and efficacy of a number of polyherbal formulations on modern scientific parameters and the subsequent evaluation of their anti-inflammatory and antibacterial effects [8]. Previously, various experimental trials showed that the selected herbal plants exhibited antibacterial activity against a variety of microorganisms which cause acne [9]. It was reported that many clinical trials conducted using polyherbal formulations showed significant effectiveness for the improvement of acne [10, 11].
2. MATERIAL AND METHOD
2.1. Plant Material
The samples of all medicinal plants including Azadirachta indica, Glycyrrhiza glabra, Calendula officinailis, Echinacea angustifolia, Aloe socotrina, Rumex crispus, Symphytum officinale, Thuja occidentalis, and Ginseng panax were supplied and authenticated through Dr. Masood Homeopathic Pharmaceutical Pvt. Ltd. All the samples were obtained using the specified pharmaceutical methods and methanolic extract was prepared using a rotary evaporator. These samples were then evaluated and standardized through pharmacognostic, phytochemical, and physicochemical analyses.
For stability testing of the cream formulation, several key parameters were evaluated to assess its stability over time and under different conditions. These included 1) Homogeneity: Ensuring uniform distribution of ingredients within the cream, 2) Appearance: Observing for any changes in texture, color, or separation over time, 3) pH: Monitoring the pH of the formulation to ensure that it remains within a stable range for skin application, 4) Smear Test: Assessing the cream's spread ability and consistency when applied to the skin, and 5) Stability at Different Temperatures: Subjecting the cream to different temperature conditions (e.g., room temperature, refrigeration, and elevated temperature) to evaluate its performance and stability under varying environmental factors. These tests helped to determine the formulation's shelf life and its suitability for use under typical storage conditions.
2.2. Composition of Anti-Acne Cream
The composition of three anti-acne creams is shown in tables 1-3. Vanishing cream is used for its base purpose and active tincture. Enhancers, also used in tincture form, are added to the base and then thoroughly mixed manually or by using shaker, to ensure the formulation is well blended. Three formulations were made with differences in their composition formula, that is, active tinctures were different in each cream named as F1, F2, and F3, respectively
Table 1. Composition of Anti-Acne Cream F1
|
Components |
Amount |
|
1. Active Ingredients |
|
|
Azadirachta indica |
0.5 gm |
|
Glycyrrhiza glabra |
0.5 gm |
|
2. Enhancers |
|
|
Aloe vera |
0.5 gm |
|
Symphytum officinale |
0.5 gm |
|
Rummex crispus |
0.5 gm |
|
Thuja occidentalis |
0.5 gm |
|
Ginseng panax |
0.5 gm |
|
3. Base |
|
|
Methyl paraben |
0.2 gm |
|
Propyl paraben |
0.10gm |
|
Sodium hydroxide |
0.1 gm |
|
Glycerine |
6ml |
|
Stearic acid |
15gm |
Table 2. Composition of Anti-Acne Cream for F2
|
Components |
Amount |
|
1. Active Ingredients |
|
|
Azadirachta indica |
0.5 gm |
|
Calendula officinalis |
0.5 gm |
|
2. Enhancers |
|
|
Aloe vera |
0.5 gm |
|
Symphytum officinale |
0.5 gm |
|
Rummex crispus |
0.5 gm |
|
Thuja occidentalis |
0.5 gm |
|
Ginseng panax |
0.5 gm |
|
3. Base |
|
|
Methyl paraben |
0.2 gm |
|
Propyl paraben |
0.10gm |
|
Sodium hydroxide |
0.1 gm |
|
Glycerine |
6ml |
|
Stearic acid |
15gm |
Table 3. Composition of Anti-Acne Cream F3
|
Components |
Amount |
|
1. Active Ingredients |
|
|
Glycyrrhiza glabra |
0.5 gm |
|
Calendula officinalis |
0.5 gm |
|
2. Enhancers |
|
|
Aloe vera |
0.5 gm |
|
Symphytum officinale |
0.5 gm |
|
Rummex crispus |
0.5 gm |
|
Thuja occidentalis |
0.5 gm |
|
Ginseng panax |
0.5 gm |
|
3. Base |
|
|
Methyl paraben |
0.2 gm |
|
Propyl paraben |
0.10gm |
|
Sodium hydroxide |
0.1 gm |
|
Glycerine |
6ml |
|
Stearic acid |
15gm |
2.3. Clinical Assessment
In collaboration with Pakistan Homeopathic Medical College (PHMC), Lahore (affiliated by Islamia University Bahawalpur), a randomized, single-blind, standard, controlled study was carried out. A total of 60 healthy volunteers, of different age groups and including both men and women, participated for the in vivo determination of anti-acne effects. These effects were determined on several areas of face including forehead, chin, and cheeks. All patients signed an inform consent before enrolling in the study.
The patients were divided randomly into four groups, with 15 patients in each group, for testing 3 polyherbal formulations (Formulation F1, Formulation F2, and Formulation F3) and one control group for comparison. In all groups, the formulations were applied topically to the affected area for a period of about 4 weeks. The effectiveness of the treatment was evaluated against the severity of the disease by comparing the results with control parameters (before treatment) [12, 13].
2.4. Study Protocol
During the study, each volunteer followed the same face cleaning routine: twice a day, in morning and evening. Clear guidance regarding the quantity of the respective formulation used, as well as how to apply and remove it, were provided. No other cosmetic product was used on the tested area [14].
2.5. Statistical Method
After collecting data, questionnaires were decoded and the results were assessed using SPSS. All the results were assessed statistically using t test for paired data of different levels of significance. The results were presented as mean± standard error.
3. RESULTS
In the current study, a total of 60 volunteers participated. Among them, 58% were women and 42% were men, having different skin textures. Some of them had oily skin and some had dry skin. The percentage is seen in the given graphs (1-2), tables (1-3), and figures (1-3) that show 58% participants with oily skin and 42% with dry skin.
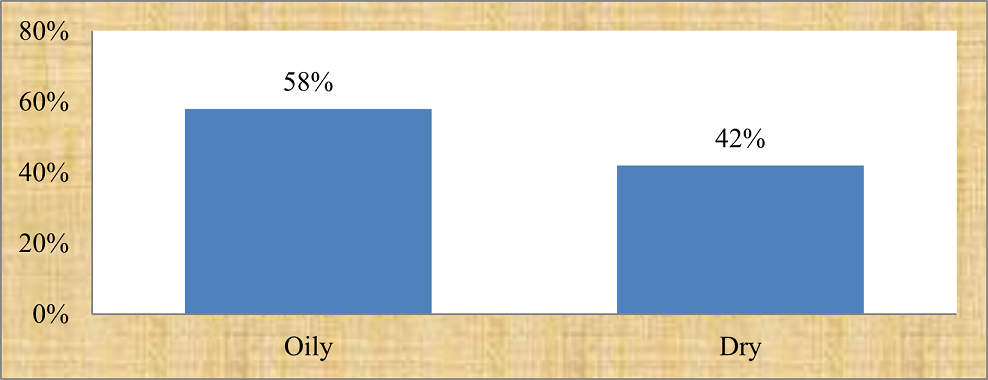
Figure 1. Percentage of Oily and Dry Skin texture
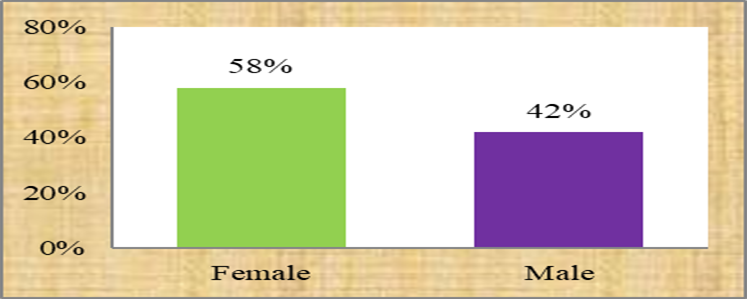
Figure 2. Percentage of Men and Women

Figure 3. Results of Formulation F1 (before and after four week study)
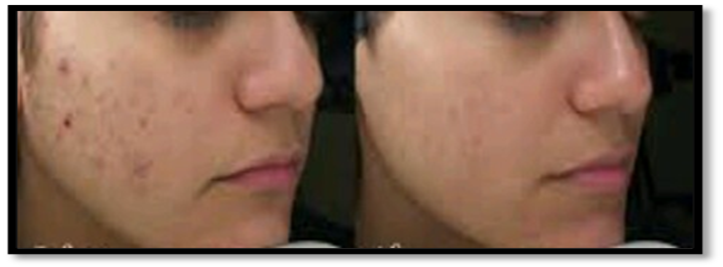
Figure 4. Results of Formulation F2 (before and after four week study)

Figure 5. Results of Formulation F3 (before and after four week study)

Figure 6. Results of Control Group without Any Formulation (after four week study)
Table 4. Level of Significance (before and after treatment with Formulation F1)
|
p-values |
Baseline Before treatment |
2nd week After treatment |
3rd week After treatment |
4th week After treatment |
|
0.140 |
0.012 |
0.002 |
0.000 |
Table 5. Level of Significance (before and after treatment with Formulation F2)
|
p-values |
Baseline Before treatment |
2nd week After treatment |
3rd week After treatment |
4th week After treatment |
|
0.41 |
0.038 |
0.037 |
0.057 |
Table 6. Level of Significance (before and after treatment with Formulation F3)
|
p-values |
Baseline Before treatment |
2nd week After treatment |
3rd week After treatment |
4th week After treatment |
|
0.621 |
0.093 |
0.076 |
0.078 |
Table 7. Level of Significance (of control group)
|
p-values |
Baseline Untreated |
2nd week Untreated |
3rd week Untreated |
4th week Untreated |
|
0.339 |
0.275 |
0.389 |
0.504 |
4. DISCUSSION
Acne, also labelled as acne vulgaris (AV), is a persistent skin disease that appears when hair follicles are blocked with oil and dead skin cells. It is characterized by blemishes or whiteheads, pimples, oily skin, and probable skin damage. This disease is presumably mediated by IGF1, as diets and smoking increase insulin/IGF1-signaling [15]. Acne patients suffer from impaired life quality owing to the anxiety, low self-esteem, and depression associated with the disease. In the current study for clinical assessment, four groups of participants were selected for the application of creams showing anti-acne activity. The participants included 58% women and 42% men with oily and dry skin textures, respectively. All the four groups had the acne issue. A questionnaire was filled by each patient to assess their habits, routine, and other factors which might affect their condition. A follow-up questionnaire was then shared with the patients to determine the study outcomes that helped to strengthen the results. Three polyherbal creams were applied on each group. The fourth group served as control. The findings were then evaluated to identify the statistical significance of the results.
Owing to a greater understanding of acne pathogenesis, various new treatment approaches, as well as permutations and combinations, have been devised. Among the topical agents, substantiated agents include benzoyl peroxide, while antibiotics and retinoids can be given alone and in combination [16]. Depending upon the patient's condition, preferred systemic agents include oral antibiotics, isotretinoin, and hormonal therapy. Physical treatment in the form of lesion removal and phototherapy are also helpful.
Due to convenience, lower cost, and the difficulty associated with getting an appointment with a dermatologist, the use of natural remedies for acne management has increased over time [17]. Table 4 presents the effect of F1 on treated subjects. The results of the paired sample t-test showed that Formulation F1 had the maximum significance level, as compared with 1st week before treatment to 2nd week after treatment, and also till the 4th week. The results showed a high level of significance (p<0.005) after the 4th week of treatment, as compared to the 2nd and 3rd weeks. The effects of cream are visible in Figure 1 (both before and after treatment results). Table 5 displays that F2 also showed good effects and significance level, but not as good as F1. The p-values (Table 5) and visual image (Figure 2) represent before and after treatment results. Whereas, for the third formulation F3, the results were less significant than formulations F1 and F2, as depicted by Table 6 and Figure 3. The findings of F1, F2, and F3 were compared with the negative control group and the results were found to be significant. The three formulations contained different combinations comprising Azadirachta indica, Glycyrrhiza glabra, and Calendula officinalis, respectively. These plants exert antibacterial effect against both gram-positive and gram-negative strains. Moreover, they have been reported to decrease the hyperpigmentation associated with acne. They do so by inhibiting the melanogenesis, that is, the biosynthetic pathway responsible for hyperpigmentation [18]. Polyherbal formulations can be a potential alternative to curtail the upsurge in bacterial resistance to principal antimicrobials, eradicate or diminish the probable adverse effects of conventional remedies, boost observance to therapy, and discourse insufficient retorts to acne treatment.
4.1. Conclusion
It was concluded that the Formulation F1 showed more anti-acne activity, as compared to other formulations, that is, F2 and F3. Moreover, it was also concluded that polyherbal creams used in the current study were effective and safe to use for treating acne. By applying advanced technologies (GC/MS, HPLC) on the selected plants, more and new Phyto-constituents can be discovered. For treating the chronic condition of acne, another line of treatment can be determined by using the current research protocol. On the basis of the preliminary phytochemical investigation, the selected plants can be used for treating many other diseases.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding details
This research did not receive grant from any funding source or agency.
Bibliography
- Strauss JS, Krowchuk DP, Leyden JJ, et al. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651–663. https://doi.org/10.1016/j.jaad.2006.08.048
- Adityan B, Thappa DM. Profile of acne vulgaris—a hospital-based study from South India. Ind J Dermatol Venereol Leprol. 2009;75:e272. https://doi.org/10.4103/0378-6323.51244
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945–973.
- Mayo Clinic Health System. Seeing spots: treating hyperpigmentation. Mayo Clinic Health System Web site. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/seeing-spots-treating-hyperpigmentation. Accessed December 23, 2024.
- Paramore LC. Use of alternative therapies: estimates from the 1994 Robert Wood Johnson Foundation national access to care survey. J Pain Symptom Manag. 1997;13(2):83–89. https://doi.org/10.1016/S0885-3924(96)00299-0
- Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a Global Alliance to improve outcomes in Acne. J Am Acad Dermatol. 2003;49(1):S1–S37. https://doi.org/10.1067/mjd.2003.618
- Bassett IB, Barnetson RSC, Pannowitz DL. A comparative study of tea‐tree oil versus benzoyl peroxide in the treatment of acne. Med J Aust. 1990;153(8):455–458. https://doi.org/10.5694/j.1326-5377.1990.tb126150.x
- Lone AH, Ahmad T, Anwar M, Sofi G, Naiyar AH. Clinical evaluation of efficacy and safety of a polyherbal formulation in acne vulgaris. Egypt Dermatol Online J. 2011;7(2):e2.
- Fabry W, Okemo PO, Ansorg R. Antibacterial activity of East African medicinal plants. J Ethnopharmacol. 1998;60(1):79–84. https://doi.org/10.1016/S0378-8741(97)00128-1
- Gopal MG, Farahana B, Pramesh R. Effectiveness of herbal medications in the treatment of acne vulgaris—a pilot study. Ind Pract. 2001;54(10):e723.
- Parveen S, Zafar S, Qureshi MA, Bano H. Clinical trial of Unani herbomineral cream to evaluate its topical effects on acne vulgaris. Ind J Tradition Know. 2009;8(3):431–436
- Kanlayavattanakul M, Lourith N. Therapeutic agents and herbs in topical application for acne treatment. Int J Cosmet Sci. 2011;33(4):289–297. https://doi.org/10.1111/j.1468-2494.2011.00647.x
- Moldovan M, Bogdan C, Ursu I, Ionescu MI, Crișan M. Evaluation of the efficacy and characterization of an anti-acne cream containing herbal extracts. Farmacia. 2016;64(4):217–223.
- Lalla JK, Nandedkar SY, Paranjape MH, Talreja NB. Clinical trials of ayurvedic formulations in the treatment of acne vulgaris. J Ethnopharmacol. 2001;78(1):99–102. https://doi.org/10.1016/S0378-8741(01)00323-3
- Mohiuddin AK. A comprehensive review of acne vulgaris. J Clin Pharm. 2019;1(1):17–45.
- Aghasi M, Golzarand M, Shab-Bidar S, Aminianfar A, Omidian M, Taheri F. Dairy intake and acne development: a meta-analysis of observational studies. Clin Nutr. 2019;38(3):1067–1075. https://doi.org/10.1016/j.clnu.2018.04.015
- Dreno B. What is new in the pathophysiology of acne, an overview. J Eur Acad Dermatol Venereol. 2017;31:8–12. https://doi.org/10.1111/jdv.14374
- Sharma S, Kumari K, Gupta H, Sah RK. Azadirachta Indica (Neem) a potential alternative for the treatment of acne: a systematic review of randomized controlled trials. Int J Novel Res Dev. 2023;8(3):111–115.