Balancing Relief and Pain: Effects of COX-2 Inhibitor Valdecoxib
Syed Mohammad Habib1*, Majid Ali1, and Long Chiau Ming2
1College of Medicine, Sulaiman Al-Rajhi University, Al-Bukayriah, Saudi Arabia
2School of Medical and Life Sciences, Sunway University, Malaysia
Abstract
Valdecoxib, a selective cyclooxygenase-2 (COX-2) inhibitor, was initially acclaimed for its gastrointestinal safety and effectiveness in managing chronic inflammatory conditions and pain. It reduced gastrointestinal complications compared to other anti-inflammatory drugs, benefiting patients with complex medication regimens. The injectable form, parecoxib, was seen as promising for acute post-surgery pain management. However, clinical trials in high-risk cardiovascular patients, particularly those undergoing coronary artery bypass grafting, revealed increased risks when using higher doses of parecoxib. These findings led to the re-evaluation of valdecoxib’s safety profile and its subsequent market withdrawal due to cardiovascular concerns and reports of serious skin reactions. Despite its withdrawal, valdecoxib has garnered interest for repurposing in other conditions. Its pharmacodynamic and pharmacokinetic properties suggest potential in qualifying palmitate-induced insulin resistance in type 2 diabetes and inhibiting matrix metalloproteinases for wound healing. Its efficacy against SARS-CoV-2 highlights drug repurposing strategies for health crises like COVID-19. Valdecoxib's established success in arthritis, dysmenorrhea, and postoperative pain, along with its potential in treating glaucoma, underscores the value of repurposing existing drugs for new therapeutic purposes. In conclusion, valdecoxib exemplifies the balance between drug safety, clinical utility, and innovative repurposing. The aim of this study is to fully harness drug potential in medical science through a concerted effort made by the scientific community, regulatory bodies, and industry stakeholders to navigate the technological and regulatory hurdles.
Introduction
Product recall is a process that involves the withdrawal of a drug from the market due to the defect or danger it poses to9consumers or due to a violation of federal law. On the contrary, market withdrawal is a process that involves the removal of a drug from the market to correct a minor issue that does not pose danger9to consumers and is not technically subject to legal action by the US Food and Drug Administration (FDA). The difference between these two processes lies in the risk of harm that the particular drug causes to the consumers. A product recall is initiated when there is a significant risk of harm posed by the drug, while a market withdrawal is carried out when there is no significant risk of harm9posed by the particular drug. Various reasons can lead to drug recalls, such as concerns related to safety, mislabelling, contamination, or deviations in strength or potency. Drug recalls can be initiated voluntarily by the supplier or the9manufacturer, at the request of the FDA, or as a legally mandated9order from the FDA [1–2].
Valdecoxib (BEXTRA®) is a nonsteroidal9anti-inflammatory drug (NSAID) approved9by the FDA on November 20, 2001 for the treatment of conditions such as dysmenorrhea, rheumatoid9arthritis, and most commonly, osteoarthritis [3, 4]. It was manufactured and marketed by G. D. Searle, a subsidiary of Pfizer in 2005 under the brand name BEXTRA®. In 2005, Pfizer voluntarily9withdrew valdecoxib from the market due9to the concerns of an increase9in the risk of stroke and heart attack [5]. A study published in The New9England Journal of Medicine found the drug to be associated with9an increased risk of cardiovascular9events [6]. The recall of valdecoxib was an important event in the history of drug recalls. It highlighted the importance of monitoring drug safety after it being approved by regulatory agencies, such as FDA. It also indicated the need for physicians and patients to be aware of the potential risks associated9with drugs and9to weigh these risks against their potential benefits when making treatment decisions.
1.1. Pharmacology of Valdecoxib
The chemical name of valdecoxib9is 4-(5-methyl-3-phenyl-4-isoxazolyl) benzene sulphonamide. It is a9diaryl-substituted isoxazole with a molecular weight of 314.36 g/mol. Its chemical9formula is C16H14N2O3S. The skeletal structure of valdecoxib is shown in9Fig. 1 [7].
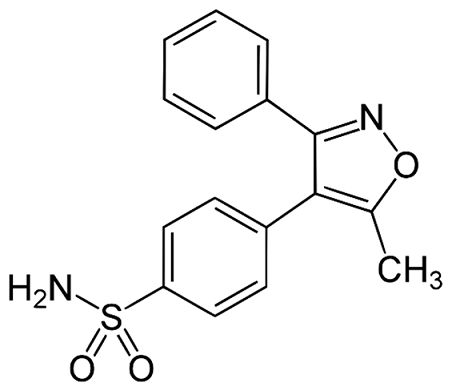
Figure 1. Chemical Structure of Valdecoxib (Adopted from Gupta V et al.)
Valdecoxib belongs to the nonsteroidal9anti-inflammatory drugs (NSAIDs) class and possesses anti-inflammatory, analgesic, and antipyretic properties. Its mechanism of action involves the inhibition of9prostaglandin synthesis which contributes to inflammation and pain. Specifically, valdecoxib selectively targets cyclooxygenase-2 (COX-2),9an enzyme-producing prostaglandins. It is important to note that at normal therapeutic plasma concentrations in humans, this drug has been known to have no action on COX-1. This fact distinguishes it from other NSAIDs. COX-2 inhibitors, unlike other NSAIDs, do not affect COX-1 enzymes that produce prostaglandins for stomach lining protection and blood clotting. COX-29inhibitors are specifically used9for treating arthritis and short-term pain caused by inflammation. A study published in BMC Anaesthesiology found that valdecoxib was quite effective in treating acute postoperative pain [3].
1.2. Pharmacokinetics of Valdecoxib
Valdecoxib attains its peak blood concentration approximately three (03) hours after oral administration as BEXTRA. When taken orally, about 83% of the drug is absorbed into the bloodstream, compared to intravenous infusion. The relationship between dose and exposure was established by administering single doses of the drug ranging from 1 mg to 400 mg, demonstrating dose proportionality. However, when taken multiple times a day for up to 14 days, exposure increases in9a more than proportional manner at doses exceeding 10 mg BID (two times a day), indicated by the area under the concentration-time9curve (AUC) value in Table 1. By the 4th day of administration, steady-state plasma concentrations of the drug are achieved [8]. The pharmacokinetic parameters set by the published work involving healthy male subjects (n=8, 20-42 years) are displayed in Table 1 [4].
Table 1. Descriptive of Steady-State9Pharmacokinetic Parameters of Valdecoxib in Healthy Male Subjects
|
Pharmacokinetics Parameters |
Mean (SD) |
|
AUC(0-24hr) (hr.ng/mL) |
1479.09(291.9) |
|
Cmax9(ng/mL) |
161.19(48.1) |
|
Tmax (hr.) |
2.259(0.71) |
|
Cmin9(ng/mL) |
21.99(7.68) |
|
Elimination9Half-life (hr.) |
8.119(1.32) |
Note. * Steady State Pharmacokinetic Characteristics9Following 14-Day OD Valdecoxib910 mg. yr: year, hr: hour, ng: nanograms, ml: milliliter (Adopted from FDA Database)
There are currently 351 drugs that are known to interact with valdecoxib. Of these, 06 are minor, 287 are moderate, and 58 are major interactions. Valdecoxib may increase the risk of bleeding when taken with aspirin, fish oil, or pregabalin. Moreover, it should not be taken concurrently with other NSAIDs such as celecoxib (as they belong to the same drug class) or clopidogrel, since their concurrent administration can heighten the risk of side9effects. Additionally, valdecoxib may reduce the effectiveness of folic acid, hydrochlorothiazide, furosemide, esomeprazole, pantoprazole, levothyroxine, and vitamin B12 when taken concomitantly. Combining valdecoxib with lisinopril, atenolol, metoprolol, losartan, or prednisone may increase the risk of side effects [9].
Individuals with sulphonamide allergy are not recommended to take valdecoxib. Its use is also contraindicated in patients with urticaria or allergic-type reactions (including asthma) after the use of NSAIDs or the intake of aspirin. In such patients, severe but fatal anaphylactic-like reactions, although rare, are possible due to the use of NSAIDs. Hence, valdecoxib is not recommended for the alleviation of pain after a coronary artery bypass graft9(CABG) surgery [8].
1.3. Safety Profile of Valdecoxib
The impact of valdecoxib on renal safety has raised concerns due to the role of the COX-2 enzyme in renal vasodilation, facilitated by prostacyclin production in endothelial9cells. The renal safety profile of valdecoxib has9been extensively investigated in patients with rheumatoid arthritis and9osteoarthritis. In combined studies, the occurrence of common renal side effects associated with COX-2 inhibition, such as albuminuria, peripheral edema, and hypertension were more frequent as compared to placebo but did not show a statistically significant difference when compared to conventional NSAIDs [10, 6]. Studies in patients with severe renal9dysfunction and end-stage renal dysfunction undergoing hemodialysis revealed a decrease of 23% in mean plasma clearance as compared to a group of healthy control individuals. However, this reduction was not considered clinically significant enough to necessitate a dosage adjustment in cases of renal insufficiency. Nevertheless, it is strongly advised against the use of valdecoxib in individuals with advanced renal diseases. Most renal effects associated with this drug are dose-dependent and linked to the occurrence of edema and an increase in blood pressure. Consequently, when administering valdecoxib to individuals reliant on the renin-angiotensin system hemodynamics (such as those with cirrhosis or congestive heart disease), careful monitoring of the renal function is recommended [11].
One of the most significant side effects associated with valdecoxib is an increase in the risk of9cardiovascular and thromboembolic events, such as myocardial infarction, pulmonary embolism, and stroke. According to a study, patients taking this drug were shown to have a higher risk of cardiovascular events in comparison to those taking a placebo. Furthermore, they were shown to have a relative risk of 2.26 for confirmed thrombotic events (including myocardial9infarction, stroke,9and death) as compared to those taking a placebo [12]. Another study reported that valdecoxib is associated with an increase in the risk of serious skin reactions,9such as Stevens-Johnson syndrome, toxic epidermal9necrolysis, as well as the development of erythema multiforme [12]. The study analyzed data from the FDA's Adverse Event Reporting9System (AERS) and found that the drug was associated with9a higher proportion of serious skin reactions, as compared to other NSAIDs. Other side effects associated with this drug included gastrointestinal bleeding and liver toxicity. These side effects are summarized9in Table 2 below.
Table 2. Common Side Effects of Valdecoxib
|
Systems |
Side Effects |
|
Cardiovascular |
(< 2%) worsened hypertension, aneurysms, angina, arrhythmias, cardiomyopathies, heart failure, coronary9artery disorder, murmurs, and hypotension |
|
Nervous9system |
Dizziness, Migraines, and headaches |
|
Dermatological |
Rashes |
|
Endocrine |
Hyperglycemia |
|
Gastrointestinal |
Abdominal pain, diarrhea, dyspepsia, flatulence, nausea |
|
Hepatic |
Increased liver enzymes |
|
Metabolic |
Edema |
|
Musculoskeletal |
Back pain/lumbago |
1.4. Counterarguments and Repurposing of Valdecoxib
Drug repurposing, also known as drug repositioning, attempts to find alternate therapeutic benefits of many drugs. The advantage of this repurposing is that it is not only cost effective but also saves time. Rather than developing new drugs, these drugs have been approved already, have passed all the phases of clinical trials, and have been studied extensively for their efficacy and safety profile. Hence, they carry the potential to provide therapeutic benefits in case of refractory conditions and rare diseases that cannot be treated by conventional drugs [13]. One such example includes aspirin, a commonly used analgesic also used for its antiplatelet action in cardiac and other diseases. It has been discovered recently to block pro-inflammatory cytokine secretion from cancer cells and also helps in the clearance of cancer cell debris via the activation of macrophages [14, 15]. Similarly, another NSAID celecoxib was used originally in the treatment of osteoarthritis. It has been approved for reducing the risk of colon cancer by reducing the risk of the formation of more polyps. Moreover, it also reduces the risk of colorectal cancer in the general population [16].
In the realm of rheumatology, valdecoxib distinguished itself as an efficacious medication, particularly for its lower propensity to cause gastrointestinal issues relative to its COX-2 inhibitor counterparts. This characteristic proved especially beneficial for rheumatology patients, who frequently are prescribed a regimen of multiple medications, some of which may have gastrointestinal side effects. The introduction of an injectable form of the drug further enhanced its value, offering a practical solution for the management of disease flare-ups in rheumatology patients’ post-surgery.
However, the primary advantage of valdecoxib, encapsulated in its parenteral form known as parecoxib, prompted its evaluation in a patient demographic characterized by a heightened risk of cardiovascular events. These trials focused on patients who had recently undergone coronary bypass graft surgery, a procedure intrinsically associated with an increased risk of thrombotic complications. In these trials, parecoxib was administered in doses significantly higher than those traditionally employed in rheumatologic care or explored within rheumatology-focused research, leading to a pronounced inhibition of COX-2 pathways [17].
Despite these cardiovascular9concerns mirrored in the case9of celecoxib, the latter remains extensively utilized in9clinical practice. The relatively9lower cardiovascular risk9associated with its usage might be attributed to the9specific contexts of its administration and application [18].
The clinical trials involving valdecoxib underscored9significant safety concerns, particularly emphasizing the elevated risk of thrombosis in patients9with cardiovascular conditions. These findings spurred9debate over the selective withdrawal of COX-2 inhibitors, including valdecoxib and rofecoxib, fuelled by the reports of potentially9fatal skin reactions and cardiovascular embolic events linked to9valdecoxib, though the accuracy of these reports has since been contested.
In light of these safety concerns, particularly the risk of9cardiovascular complications, selective COX-2 inhibitors such as9valdecoxib were withdrawn from the market. Nevertheless, there is a9burgeoning interest in repurposing these drugs for a variety of conditions,9ranging from cancer to epilepsy,9psychiatric9disorders, obesity, and Alzheimer's9disease.9This paradigm shift9underscores a holistic strategy aimed at9harnessing their therapeutic potential beyond their initial indications, advocating for a9unified and science-based approach to drug repurposing. This perspective not only reconciles with past controversies but also forecasts9a promising horizon for these compounds across9diverse medical applications [19].
The repurposing of valdecoxib, a9selective COX-2 inhibitor initially approved for pain and inflammation, unveils a spectrum of potential therapeutic applications9beyond its original designation. The9current research highlights its potential to address9various diseases including cancer,9epilepsy, psychiatric9disorders, obesity, and Alzheimer’s9disease, thus demonstrating its9expansive therapeutic implications [19]. This vast potential emphasizes the importance of re-evaluating well-established drugs for novel therapeutic9purposes, as well as leveraging their known9pharmacodynamics, pharmacokinetics, and safety profiles to accelerate the drug development9process.
Specifically, the structural properties of this drug have9been investigated for their potential against matrix metalloproteinases (MMPs),9indicating a promising path for enhancing wound healing9capabilities. This research points to the viability of repurposing existing drugs for new therapeutic targets, thus not only expanding9their application but also enhancing9patient care outcomes in areas9such as delayed wound healing [20].
Furthermore, the ongoing COVID-19 pandemic has9necessitated swift drug repurposing strategies. Valdecoxib has9been identified among compounds with potential efficacy against SARS-CoV-2, showcasing9the adaptability of drug repurposing efforts in9tackling the emergent global health crises [21]. This approach not only highlights9the flexibility of modern pharmacology in addressing unforeseen challenges but also emphasizes the9importance of comprehensive drug databases and9computational methods in identifying9promising repurposing candidates.
Despite the promising outlook of repurposing valdecoxib,9transitioning from concept to clinical applications9entails navigating technological and regulatory hurdles. Successful9drug repositioning initiatives9require a collaborative approach, incorporating insights from various scientific disciplines and simplifying regulatory processes to ensure the9seamless integration of repurposed9drugs into clinical practice [22].
Research indicates that valdecoxib significantly9enhances glucose uptake9in skeletal muscle cells and also enhances the9signaling of insulin, offering a potential pharmacotherapeutic option for managing insulin resistance and type 2 diabetes [23]. Its documented9efficacy in pain management for9conditions such as osteoarthritis, rheumatoid arthritis,9primary dysmenorrhea, and postoperative pain, coupled9with a lower incidence of gastrointestinal complications, highlights its potential for broader9pain management applications [24].
The repurposing of old drugs for new therapeutic uses in fields like oncology is gaining momentum. Advances have revealed many old drugs to show activity9at novel antioncogenic pharmacological targets,9suggesting their potential beyond their initial indications [25].
Furthermore, valdecoxib has been shown9to prevent endoplasmic reticulum stress-induced cell death in experimental glaucoma by blocking the9PERK-ATF4-CHOP pathway, indicating its therapeutic potential9in neurodegenerative diseases,9especially in managing retinal ischemia-reperfusion injury [26].
Addressing technological and regulatory9challenges in drug repurposing is essential to fully realize the potential of valdecoxib's repurposing. Innovative9approaches are recommended9to efficiently navigate these barriers [27].
2. CONCLUSION
To conclude, the repurposing of valdecoxib9represents the broader potential of re-evaluating existing pharmaceuticals for9new therapeutic uses. This strategy offers a9cost-effective pathway to drug development and holds the promise9of meeting unmet medical needs across various health conditions. As the field progresses, it's crucial to support these9efforts with solid scientific evidence9and adaptable regulatory frameworks to navigate9the dynamic landscape of drug repurposing.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding details
This research did not receive grant from any funding source or agency.
Bibliography
- U.S. Food and Drug Administration. Drug recalls. FDA Web site. https://www.fda.gov/drugs/drug-safety-and-availability/drug-recalls. Accessed April 13, 2024.
- U.S. Food and Drug Administration. Recalls, corrections and removals (devices). FDA Web site. https://www.fda.gov/medical-devices/postmarket-requirements-devices/recalls-corrections-and-removals-devices. Accessed April 13, 20024.
- Chavez ML, DeKorte CJ. Valdecoxib: a review. Clin Ther. 2003;25(3):817–851. https://doi.org/10.1016/s0149-2918(03)80110-8
- U.S. Food and Drug Administration. BEXTRA® valdecoxib tablets serious skin reactions. FDA Web site. https://www.accessdata.fda.gov/drugsatfda_docs/label/2004/21341lbl.pdf. Accessed April 13, 2024.
- U.S. Food and Drug Administration. Postmarket drug safety information for patients and providers. FDA Web site. https://www.fda.gov/drugs/drug-safety-and-availability/postmarket-drug-safety-information-patients-and-providers. Accessed April 13, 2024.
- Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. New Eng J Med. 2000;343(21):1520–1528. https://doi.org/10.1056/NEJM200011233432103
- Com. Valdecoxib interactions. Drugs Web site. https://www.drugs.com/drug-interactions/valdecoxib.html. Assessed April 13, 2024.
- National Library of Medicine Web site. https://pubchem.ncbi.nlm.nih.gov/compound/Valdecoxib. Accessed April 13, 2024.
- Nussmeier NA, Whelton AA, Brown MT, et al. Complications of the COX-2 inhibitors parecoxib and valdecoxib after cardiac surgery. New Eng J Med. 2005;352(11):1081–1091. https://doi.org/10.1056/NEJMoa050330
- Bensen W. Efficacy and safety of valdecoxib in treating the signs and symptoms of rheumatoid arthritis: A randomized, controlled comparison with placebo and naproxen. Rheumatology. 2002;41(9):1008–1016. https://doi.org/10.1093/rheumatology/41.9.1008
- Atukorala I, Hunter DJ. Valdecoxib: the rise and fall of a COX-2 inhibitor. Expert Opin Pharmacother. 2013;14(8):1077–1086. https://doi.org/10.1517/14656566.2013.783568
- Obeid S, Libby P, Husni E, et al. Cardiorenal risk of celecoxib compared with naproxen or ibuprofen in arthritis patients: insights from the PRECISION trial. Eur Heart J Cardiovasc Pharmacother. 2022;8(6):611–621. https://doi.org/10.1093/ehjcvp/pvac015
- Sakai N, Kamimura K, Terai S. Repurposable drugs for immunotherapy and strategies to find candidate drugs. Pharmaceutics. 2023;15(9):e2190. https://doi.org/10.3390/pharmaceutics15092190
- Wang X, Wang T, Chen X, et al. Efficacy and safety of oral anticoagulants in older adult patients with atrial fibrillation: pairwise and network meta-analyses. J Am Med Dir Assoc. 2023;24(8):1233–1239. https://doi.org/10.1016/j.jamda.2023.05.010
- Gilligan MM, Gartung A, Sulciner ML, et al. Aspirin-triggered proresolving mediators stimulate resolution in cancer. Proc Natl Acad Sci U S A. 2019;116(13):6292–6297. https://doi.org/10.1073/pnas.1804000116
- North GL. Celecoxib as adjunctive therapy for treatment of colorectal cancer. Ann Pharmacother. 2001;35(12):1638–1643. https://doi.org/10.1345/aph.10133
- Gupta V, Panwar S, Pande RK, Arora R. Drug-related stevens–johnson syndrome and toxic epidermal necrolysis: a review. Ind J Critical Care Med. 2021;25(5):575–579. https://doi.org/d10.5005/jp-journals-10071-23826
- Ziemer M, Wiesend CL, Vetter R, et al. Cutaneous adverse reactions to valdecoxib distinct from stevens-Johnson syndrome and toxic epidermal necrolysis. Arch Dermatol. 2007;143(6):711–716.https://doi.org/10.1001/archderm.143.6.711
- El-Malah AA, Gineinah MM, Deb PK, et al. Selective COX-2 inhibitors: road from success to controversy and the quest for repurposing. Pharmaceuticals. 2022;15(7):e827. https://doi.org/10.3390/ph15070827
- Mude L, Jupudi S, Swaroop AK, Tallapaneni V, Karri VVSR. Molecular insights in repurposing selective COX-2 inhibitor celecoxib against matrix metalloproteinases in potentiating delayed wound healing: a molecular docking and MMPB/SA based analysis of molecular dynamic simulations. J Biomol Struct Dynam. 2023;42(5):2437–2448. https://doi.org/10.1080/07391102.2023.2209666
- Zhou Y, Hou Y, Shen J, Huang Y, Martin W, Cheng F. Network-based drug repurposing for novel coronavirus 2019-nCoV/SARS-CoV-2. Cell Discov. 2020;6:e14. https://doi.org/10.1038/s41421-020-0153-3
- EMBL-EBI. Exploring ChEMBL data with the new ChEMBL interface. EBI Web site. https://www.ebi.ac.uk/training/events/exploring-chembl-data-new-chembl-interface-0/. Updated March 11, 2020. Accessed April 13,
- Kim TJ, Lee HJ, Pyun DH, Abd El-Aty AM, Jeong JH, Jung TW. Valdecoxib improves lipid-induced skeletal muscle insulin resistance via simultaneous suppression of inflammation and endoplasmic reticulum stress. Biochem Pharmacol. 2021;188:e114557. https://doi.or/10.1016/j.bcp.2021.114557
- Fenton C, Keating GM, Wagstaff AJ. Valdecoxib. Drugs. 2004;64:1231–1261. https://doi.org/10.2165/00003495-200464110-00006
- Shah RR, Stonier PD. Repurposing old drugs in oncology: opportunities with clinical and regulatory challenges ahead. J Clin Pharm Ther. 2019;44(1):6–22. https://doi.org/10.1111/jcpt.12759
- Gao Z, Li M, Yao F, et al. Valdecoxib protects against cell apoptosis induced by endoplasmic reticulum stress via the inhibition of PERK-ATF4-CHOP pathway in experimental glaucoma. Int J Mol Sci. 2022;32(21):e12983. https://doi.org/10.3390/ijms232112983
- Pushpakom S, Iorio F, Eyers P, et al. Drug repurposing: progress, challenges and recommendations. Nat Rev Drug Discov. 2018;18:41–58. https://doi.org/10.1038/nrd.2018.168