Evaluation of Cost-Effective Therapy by Comparing Brands of the Same Formulation in Pakistan
Nayab Sajid1, Abdul Aziz2*, Samia Asif3, Saba Ashraf4, Azeem Ahmed Iqbal5, Gohar Ali2, Muhammed Amir2, and Junaid Ikram2
1Faculty of Pharmacy, University of Lahore, Lahore, Pakistan
2Department of Pharmacy, Abasyn University, Islamabad, Pakistan
3Departmeny of Biochemistry and Applied Chemistry, Government College University, Faisalabad, Pakistan
4Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore, Pakistan
5Punjab Pharmacy Council, Lahore, Pakistan
Abstract
In Pakistan, where millions face the burden of healthcare costs, the choice between branded and alternative drug formulations plays a crucial role in patient outcomes. Often, branded medications are prescribed over more cost-effective options, exacerbating financial strain for patients, especially in low- and middle-income settings. The current study is crucial to address healthcare affordability, highlighting significant cost disparities between prescribed branded medications and alternatives. It critically aimed to evaluate cost-effective therapies by comparing prescribed brands with other options for cardiovascular diseases (CVDs), diabetes, neurological disorders, and paediatrics. Furthermore, the study also identified the cost-effective therapies for CVDs, diabetes, neurological disorders, and pediatric conditions between branded medications with their generic and alternative counterparts in Pakistan. This would help to achieve cost-effective therapies. Additionally, it also shed light on the hurdles faced by the regulators to impose generic prescribing across Pakistan. It may motivate healthcare providers and policymakers about the benefits of generic prescribing to provide cost-effective treatment plan which may lead towards the overall patients’ satisfaction. Data collected from various regions of Pakistan across public and private healthcare sectors revealed significant cost disparities between branded and alternative medications. The analysis conducted in the study indicated a potential cost reduction of up to 66% for CVDs, 47% for neurological disorders, and 21% and 43% for diabetes and paediatrics, respectively, by opting for alternative brands. These findings underscore the urgent need for policy reforms, promoting generic prescriptions and leveraging pharmacists' expertise to enhance affordability and accessibility in the Pakistani healthcare system.
Introduction
As compared to their branded counterparts, generic medicines may substantially reduce out-of-pocket expenditure on drugs for patients with chronic diseases and low-income populations [1]. Generic substitution of brand prescriptions is an accepted practice in many parts of the world, and this is often done for economic reasons and equally therapeutic effectiveness of the medicines. Therapeutic value of medical therapies varies largely and an appropriate assessment may contribute to the economic treatment plan [2]. In Pakistan, however, generic substitution is not a universal acceptance practice, and many reasons contribute to these problems. Major factors include the non-availability of generic formulations and distrust of generic medicines by practitioners often due to perceived inferior quality and counterfeiting of drugs. These may also include lack of government interest in general public health, lack of stronghold and transparent policies of the regulatory authority over manufacturing industries and the central pillar in drugs manufacturing, transporting, stocking, and quality control units [3]. Furthermore, it also includes unethical practices between manufacturing companies and practitioners. However, implementing generic prescribing policy is an ongoing process in institutional settings, where drugs can be procured in bulk and dispensed from the institutional inventory with appropriate quality control measures [4].
To promote generic prescriptions in public sector hospitals, the Drug Regulatory Authority of Pakistan (DRAP) has proposed a generic prescription plan to the government, public institutions, and hospitals in recent years. This plan focuses on the adoption of generic prescription in Pakistan instead of branded prescription. However, many obstacles and problems must be cleared and solved before implementing such plans in Pakistan. No therapeutic equivalence studies have been conducted for the generic drugs to be equally accepted as their branded counterparts. This is because generic medicines are required to be the same as branded medicines in dosage, safety, effectiveness, strength, stability, and quality. as well as in their administration. This is the reason most of the practitioners rejected the ill-timed or before clarification notice of the DRAP.
Globally, noncommunicable diseases (NCDs) (CVDs, diabetes, and neurological diseases) have emerged as significant causes of death. These kill around 41 million people each year, accounting for 71% of all global fatalities [5]. More than 85% of these deaths happen in low- and middle-income countries (LMICs). With a population of 225 million people, Pakistan is the fifth most populated country in the world, and approximately half of its people suffer from one or more chronic diseases [6]. Furthermore, it is anticipated that between 2010 and 2025, nearly 3.87 million individuals would die in Pakistan due to NCDs. These include cardiovascular diseases (CVDs), cancer, and chronic respiratory disorders. According to a cited study, the economic cost linked with NCD fatalities would range between $152 million and $296 million between 2010 and 2025 [7]. Using generic drugs is a policy option that allows access to affordable medications and cost-effective therapy.
The current study provides an opportunity to address negative perceptions about generic drugs in the current healthcare system. In this regard, counselling by a qualified person may further improve the utilization of generic drugs, reducing the overall cost of therapy. Lowering the cost of treatment can reduce the patient's psychological pressure and stress level. Furthermore, the current study provides a clue to policymakers with relevant information that may aid in their decision-making process. The outcomes of this study would serve as a strategic tool in the area of generic cost savings.
1.1. Non-Communicative Diseases (NCDs)
1.1.1. Cardiovascular Diseases (CVDs).
CVDs are a significant hazard among NCDs), accounting for approximately 17.9 million deaths per year [8]. WHO defines CVDs as hypertension (HTN), coronary heart disease, cerebrovascular disease (stroke), peripheral vascular disease, heart failure, rheumatic heart disease, congenital heart disease, and cardiomyopathies [5]. According to the global burden of disease data, CVDs are among the top ten significant causes of death in Pakistan, with ischemic heart disease (IHD) accounting for 8% of all fatalities [5, 8]. WHO advises multi-drug therapy for the treatment and prevention of CVDs in people at ≥30% risk of having a stroke or heart attack within 10 years. These therapies include blood pressure (BP) lowering medications, antihyperlipidemic (HLD) medications, diabetic blood glucose control, and anti-platelet agents for secondary prevention of myocardial infarction. Despite promising clinical data supporting the usefulness of medicines in the prevention and management of CVDs, there is a cost gap among patients. Furthermore, long-term therapy is required for CVDs, diabetes, and neurological illnesses, which may result in significant healthcare costs.1.1.2. Diabetes.
Diabetes is a chronic metabolic disorder resulting from the unavailability of insulin to the cell. This may cause impaired production or resistance to produce insulin and lead towards glucose elevation in the blood. Diabetes may lead to other life-threatening disorders, such as nephropathy, neuropathy, and retinopathy.Older adults sometimes delay refilling their prescriptions due to high costs. The inability to refill a prescription could result in the individual not following their medication Regimen, which, in turn, can lead towards further health problems and even hospitalizations.According to Wood, high hospital admission rates have been reported due to medication non-compliance [9]. Among diabetic and heart disease patients, those who do not take their medication as prescribed have a higher mortality rate, 12.1% versus 6.7% [10]. Additionally, among those who have diabetes, hypertension, high cholesterol levels, and poor heart conditions, the rate of hospitalization is higher compared to those who take their medication as prescribed. The cost of medicines to treat chronic conditions has social and economic implications. Researchers have identified cost-saving approaches from various studies, estimates resulting from generic drugs and generic and therapeutic substitutions.
1.1.3. Pediatrics.
Pediatric disorders include protein-energy malnutrition and acute watery diarrhoea, malaria, pneumonia (severe), anaemia, asthma, and chicken pox. Moreover, these may also include diphtheria, leukaemia, measles, mumps, polio, tuberculosis, whooping cough, lyme disease, fever, down syndrome, dental caries, cystic fibrosis, chagas disease, candidiasis, cancer, bronchiolitis, and HIV/AIDS (paediatrics aids). These account for 75% of the admissions. Miscellaneous diseases account for only 25% of the cases.1.1.4. Neurological Disorder.
Neurological disorders are among the fifth leading causes of death globally and are also responsible for 5.53% of the total global deaths. Tension-type headaches (1505·9 million cases), migraine (958·8 million), headaches caused by the overuse of medication (58·5 million), and Alzheimer's disease (AD) including other dementias (46·0 million) were the most prevalent neurological disorders. Stroke is the leading cause of death, accounting for 67.3% of all neurological disorders, followed by AD and other dementias. Deaths caused by stroke among young adults have increased significantly in developing countries. Moreover, the number of disability-adjusted life years (DALYs) was seven times higher as compared to developed countries. WHO has estimated that 80% of all strokes would occur in developing countries. Dementia due to AD was more common, that is, 60% than vascular dementia which is 30% worldwide. Epilepsy affects approximately 70 million people worldwide and 90% of people in developing countries have epilepsy. Stroke is a serious health concern in Pakistan, with an annual incidence of 250/100,000 population. Epilepsy attacks 2.4 million people every year and cripples 5 million people for the rest of their lives. The prevalence of depression and anxiety in Pakistan is 34% and is more common among females. Depression is more prevalent in rural areas (66% in women and 25% in men) than in urban areas (25% in women and 10% in men). Minimal data indicates that the prevalence of AD is more frequent in the elderly population.2. METHODOLOGY
2.1. Settings
The medicines price and affordability data (prescription data) for four (4) key illness areas including CVDs, diabetes, neurological disorders, and paediatrics, were collected from January-May 2022. This survey covered five regions/cities: Islamabad (Federal Capital), Rawalpindi (Punjab province), Peshawar (KPK province), Mardan (KPK province), and Timergara (KPK province). Data was collected to avoid errors and improve understanding and presentation. Data on the pricing of medicines for all specified disorders was collected from public and private sector hospitals, as well as commercial retail pharmacies.
2.2. Sample Size Estimation
The study included 15 prescriptions per condition, proportional to their prevalence and representative of the healthcare settings in the selected regions. The latest studies addressing the similar issues were conducted with the sample size ranging between 40-100 prescriptions [11, 12].
2.3. Data Source
2.3.1. Healthcare Establishments.
A total of 60 prescriptions were collected which fulfilled the inclusion criteira, 15 for each disease were collected from 10 hospitals. Price data was collected from 20 retail pharmacies in different regions. This included a total of 42 medicines, 10 for CVDs, 14 for diabetes, 09 for neurological disorders, and 09 for paediatrics diseases. Afterwards, for each drug/medicine, 3 alternatives were the competitors and were available at lower prices than the prescribed medicines. A total of 120 alternative medicines were studied for price evaluation as shown in the Table 1. A total of 33 prescriptions were rejected for the exclusion criteria, mentioned below in detail.Table 1. Prescriptions for Cardiovascular, Diabetic, Pediatric and Neurological Disorders were Reviewed for the Drug Class, Generic Name, and Total Number Of Times the Drug is Prescribed
|
Cardiovascular |
||
|
Class of drugs |
Generics |
Total Drugs |
|
NSAIDs |
Aspirin (R8) |
8 |
|
Calcium Channel Blockers |
Amlodipine+ Valsartan (R3) |
3 |
|
PPIs |
Omeprazole(R8) |
8 |
|
Loop diuretics |
Furosemide + Spironolactone (R7) |
7 |
|
Beta-blockers |
Metoprolol tartrate(R3) nebivolol Bisprolol fumarate (R3) |
7 |
|
Anti-platelets |
Aspirin+ clopidogrel (R2) |
2 |
|
Statins |
Atorvastatin (R3) |
3 |
|
Nitrates |
Glyceryl trinitrate (R3) |
3 |
|
Alpha and beta-blockers |
Carvedilol |
1 |
|
Angiotensin Receptor blockers |
Losartan potassium candesartan |
2 |
|
H2 blockers |
Famotidine |
1 |
|
Anti-diabetics |
||
|
Anti-diabetics |
Glimepiride (R5), Sitagliptin (R8), Metformin (R3), Gliclazide (R2) |
17 |
|
Anti-hypertensive |
Losartan (R2), Ramipril (R2), Bisoprolol (R2) |
6 |
|
Multivitamins |
Calcium Vit D, E, K (R2), Vit B12 (mecobalamin) (R2) |
4 |
|
Anti-depressant |
Duloxetine(R2), Escitalopram(R2) |
4 |
|
Antacids |
Aluminum Hydroxide (R2), Aluminum-mag Hydroxide-Simethicone (R2) |
4 |
|
Anticonvulsants |
Pregabalin (R2) |
2 |
|
PPIs |
Esomeprazole (R2), Omeprazole (R2), Pantoprazole (R2) |
6 |
|
Anti-antihistamines |
Cetirizine(R2), Fexofenadine(R2) |
4 |
|
Bronchodilators |
Mynophylline(R2) |
2 |
|
NSAIDs |
Nimesulide(R1), Meloxicam(R2), Aspirin (R2) |
5 |
|
Calcium channel blockers |
Amlodipine (R2) |
2 |
|
Antibiotics |
Azithromycin (R2) |
2 |
|
Antipyretics |
Paracetamol (R2) |
2 |
|
Anti-emetics |
Domperidone (R2) |
2 |
|
Anti-platelet agents |
Clopidogrel (R2) |
2 |
|
Lipid-lowering drugs |
Atorvastatin (R2) |
2 |
|
Analgesics |
Tramadol (R2) |
2 |
|
Paediatrics |
||
|
Antibiotics |
Co-amoxillin (R2), Cefpodoxime proxitel Cefixime (R3) |
6 |
|
NSAID |
Ibuprofen |
1 |
|
Corticosteroids |
Triamcinolone, Acetonide |
1 |
|
Histamine H2-receptor antagonists |
Famotidine (R3) |
2 |
|
Antipyretic |
Paracetamol (R4) |
1 |
|
Anthelmintics |
Mebendazole |
1 |
|
Antihistamines |
Levocitirizine, Cetrizine (R4) |
5 |
|
Leukotrienes receptor antagonists |
Montelukast (R3) |
3 |
|
Bronchodilators |
Ipratropium (R2) |
2 |
|
Anticonvulsants |
Sodium valproate |
1 |
|
Supplements |
Cholecalciferol (R3), Polysaccharide iron complex, Multivitamin, Zinc enriched yeast, Lactobacillus rhamnosus |
8 |
|
Neurology |
||
|
SSRIs |
Fluoxetine(R2) Esctalopram (R2) |
4 |
|
Anti-convulsants |
Pregabalin(R3) |
3 |
|
NSAIDs |
Naproxen(R6) Aceclofenac (R2) Ketoprofen(R2) Diclofenac sod (R2) Glucosamine(R2) |
14 |
|
Supplements |
Digestive enzymes (R1), Methocobalamine+vitamins (R3), Cacium+vit D(R2), Cholecaferol Alfacalcidol calcium, Multivitamins |
9 |
|
Anti-diabetics |
Sitagliptin + Metformin |
1 |
|
Calcium channel blockers |
Amlodipine (R2) |
2 |
|
SNRIs |
Duloxetine (R2) |
2 |
|
Anti-depressants |
Amitriptyline (R2) Nortriptyline (R2) |
4 |
|
Beta-blockers |
Propranolol |
1 |
|
Atypical antipsychotics |
Olanzapine+fluoxetine |
1 |
|
Antipyretics |
Paracetamol + Orphenadrine (R2) |
2 |
|
Laxatives |
Lactulose |
1 |
|
Analgesics |
Thiocolchicosides (R2) |
2 |
|
Bisphosphonates |
Ibandronate sodium |
1 |
|
Anti-bacterial |
Enoxacin sesquihydrate |
1 |
2.3.2 Inclusion and Exclusion Criteria.
2.3.2.1. Inclusion Criteria. The prescription for CVDs, diabetes, neurological disorder, and paediatric conditions was selected from region-specific registered healthcare establishments working under Punjab Healthcare Commission.
2.3.2.2. Exclusion Criteria. The prescriptions with multiple conditions, for instance incomplete prescriptions or prescriptions from unauthorized practitioners or healthcare establishments.
2.4. Data Analysis
To represent the data, following softwares and methods were used:
- SPSS (Descriptive statistics including mean, percentage, and etc.)
- The costs comparison of the brand and alternate
- The cost comparison was represented graphically by the charts
- R language code for sample size estimation using the pwr package
2.4.1. Consent Forms.
This study was conducted after the approval of ethical committee by submitting prior approvals from the healthcare establishments. Afterwards, the consent of agreements was submitted by the prescriber and patients to the relevant department.3. RESULTS AND DISCUSSION
3.1. Cardiovascular Diseases (CVDs)
Table 2. Price Comparison of Prescribed Brands with Available Alternate in Prescription-1 for CVS
|
Sr. no. |
Prescribed brands |
Generics |
Price |
Alternate Brands#1 |
Price |
Alternate Brands#2 |
Price |
Alternate Brands#3 |
Price |
Dosage forms |
|
1 |
Loprin |
Aspirin |
51 |
Apiscot |
26 |
Angipro |
28 |
Glorin |
30 |
Tablets |
|
2 |
Extor |
Amlodipine+ Valsartan |
330 |
Avsar |
290 |
Amodip-V |
230 |
Biforge |
145 |
Tablets |
|
3 |
Capzol |
Omeprazole |
250 |
Cipro |
250 |
Benzim |
240 |
Noran |
250 |
Capsule |
|
4 |
Spiromide |
Furosemide+ Spironolactone |
215 |
Spidar |
120 |
Spirotech |
110 |
Spirofer |
140 |
Tablets |
|
5 |
Merol |
Metoprolol Tartrate |
75 |
Betaloc |
40 |
Carsel |
65 |
Bulmet |
30 |
Tablets |
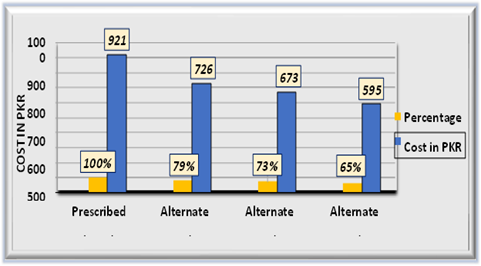
Figure 1. Cost Comparison of Prescription-1 for Cardiovascular Complications
Table 2 shows the cost comparison of the prescribed brands for patients having CVDs with the available alternative brands in the market. The tabular and graphic data shows a significant difference in prescription cost. The prescribed brand's cost is selected as the standard (100%) for their alternative drugs. The cost in percentage shows that the procurement of the prescribed brands would cost 921 PKR (100% (standard)). If the alternate brand #1 is selected, which would cost 726 PKR (79% of the 921 PKR), it means that 21% (193 PKR) can be saved. Similarly, alternate brands#2 may save 27% (248 PKR) and alternate brands#3 would save 35% (322 PKR) in a single prescription filling. The same method was repeated with the rest of the data as well.
Table 3. Price Comparison of Prescribed Brands with available Alternate in Prescription-2 for CVDs
|
Sr. no. |
Prescribed brands |
Generics |
Price |
Alternate Brands#1 |
Price |
Alternate Brands#2 |
Price |
Alternate Brands#3 |
Price |
Dosage forms |
|
1 |
Lowplat plus |
Aspirin+ Clopidogrel |
150 |
Ascard plus |
150 |
Clopido plus |
120 |
Abiclot plus |
130 |
Tablets |
|
2 |
Lochol |
Atorvastatin |
210 |
Atorscot |
180 |
Colezaf |
130 |
Atorex |
150 |
Tablets |
|
3 |
Cardnit |
Glyceryl Trinitrate |
210 |
Webser |
150 |
Glyrate-SR |
160 |
Glycon-N |
100 |
Tablets |
|
4 |
Spiromide |
Furosemide+ Spironolactone |
215 |
Spidar |
120 |
Spirofer |
140 |
Spirotech |
110 |
Tablets |
|
5 |
Capzol |
Omeprazole |
250 |
Cipro |
250 |
Noran |
250 |
Benzim |
240 |
Capsule |
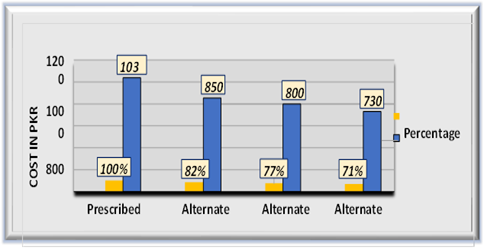
Figure 2. Cost Comparison of Prescription-2 for Cardiovascular Complications
Table 3 shows the cost comparison of the prescribed brands for patients with CVDs with the available alternative brands in the market. The tabular and graphic data showed a significant difference in prescription cost. The prescribed brands cost 1035 PKR. If the alternate brand #1 is selected, which would cost 850 PKR (82% of the 1035 PKR), it means that 18% (186 PKR) can be saved. Similarly, alternative brand #2 can save 23% (238 PKR) and alternate brands#3 would save 29% (300 PKR) in a single prescription filling.
3.2. Neurological Disorders
Table 4. Price Comparison of Prescribed Brands with Available Alternate in Prescription-1 for Neurological Disorders
|
Sr. no. |
Prescribed Brands |
Generics |
Price |
Alternate Brands#1 |
Price |
Alternate Brands#2 |
Price |
Alternate Brands#3 |
Price |
Dosage forms |
|
1 |
Plux 20mg |
Flouxetine |
275 |
Depset |
65 |
Fluxac |
100 |
Xeal |
83 |
Tablets |
|
2 |
Zeegap 50mg |
Pregabalin |
285 |
Aropen |
150 |
Gablin |
194 |
Breglin |
200 |
Capsules |
|
3 |
Co purpal 500\20 |
Naproxen + esomeprazole |
735 |
Alidase |
122 |
Alnapro |
180 |
Calgesic |
99 |
Tablets |
|
4 |
Oscal D |
Alfacalcidol calcium |
580 |
Bone care c |
340 |
Cal-K |
300 |
Kalsob |
533 |
Tablets |
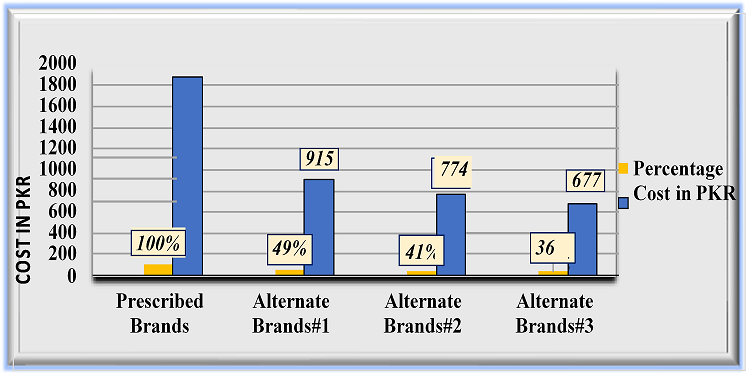
Figure 3. Cost Comparison of Prescription-1 for Cardiovascular Complications
Table 5 presents the prescribed medicines for neurology, their respective alternatives, and their prices. Figure 1 evaluates the total cost differences. The prescribed brands cost 1875 PKR. If thealternate brand #1 is selected, which would cost 915 PKR (49% of the 1875 PKR), 51% (956 PKR) can be saved. For that, alternative brand #2 can save 59% (1106 PKR) and alternative brand #3 would save 64% (1200 PKR) in a single prescription filling.
Table 5. Price Comparison of Prescribed Brands with Available Alternate in Prescription-2 for Neurological Disorders
|
Sr. no. |
Prescribed Brands |
Generics |
Price |
Alternate Brands#1 |
Price |
Alternate Brands#2 |
Price |
Alternate Brands#3 |
Price |
Dosage form |
|
1 |
Sitamt 500\50 |
Sitagliptin+ metformin |
412 |
Tagipmet |
392 |
Sitagliptin |
395 |
Qosmet |
190 |
Tablets |
|
2 |
Norvasc 10mg |
Amlodipine |
804 |
Lodopin |
92 |
Onato |
135 |
Amodip |
150 |
Tablets |
|
3 |
Zenbac30m g |
Duloxetine |
375 |
C-Yalta |
261 |
DePree |
180 |
Dulan |
280 |
Capsules |
|
4 |
Xymec |
Digestive enzymes |
475 |
Zymosaf |
147 |
H |
31 |
Novozyme |
45 |
Tablets |
|
5 |
Acenac sr 100mg |
Aceclofenac |
375 |
Alkeris |
54 |
Aceclo |
35 |
Acemed |
60 |
Capsules |
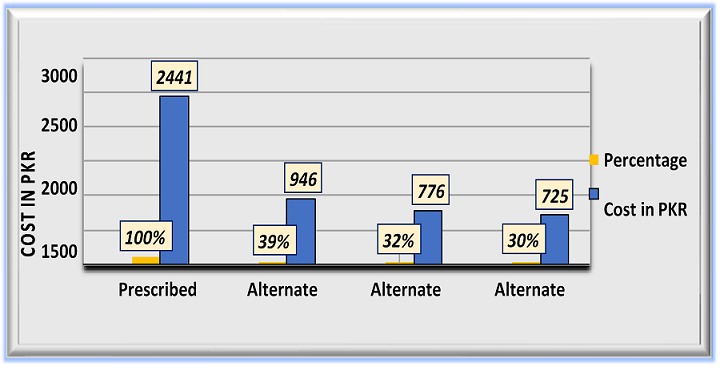
Figure 4. Cost Comparison of Prescription-2 for Neurological Disorders
Table 6 presents the prescribed medicines for neurology, their respective alternatives, and their prices. Figure 2 evaluates the total cost differences. The prescribed brands cost 2441 PKR. If the alternate brand #1 is selected, which would cost 946 PKR (39% of the 2441 PKR), 61% can be saved (1489 PKR). Alternate brand #2 can save 68% (1659 PKR), and alternate brand #3 would save 70% (1708 PKR) in a single prescription filling.
3.3. Diabetes
Table 6. Price Comparison of Prescribed Brands with Available Alternate in Prescription-1 for Diabetes
|
Sr. no. |
Prescribed brands |
Generics |
Price |
Alternate brands#1 |
Price |
Alternate brands#2 |
Price |
Alternate brands#3 |
Price |
Dosage forms |
|
1 |
Orinase(2mg) |
Glimepiride |
240 |
DAZEMEP |
200 |
A-GLIM |
100 |
AMARIT |
56 |
|
|
2 |
Neoglip (5omg) |
Sitagliptin Phosphate USP+ Metformin HCL |
414 |
Sitaform |
325 |
Alosita-Met |
308 |
Qosmet tablet |
190 |
Tablets |
|
3 |
Tansin |
Losartan (50mg) |
188 |
NOKTAN |
160 |
NORMOPRESS |
150 |
CORIK |
99 |
Tablets |
|
4 |
Daily cal |
Calcium, Vitamin D, E, K2, |
599 |
Osteoflex |
480 |
Calavant-d Tab |
450 |
Cac1000 Plus |
395 |
Tablets |
|
5 |
Duzalta (30mg) |
Duloxetine HCl USP |
369 |
DULOXET |
266 |
DURON |
160 |
DUDEP |
100 |
Tablets |
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
DIABIN |
Metformin(HCl) |
91 |
GLUMIN |
56 |
metformin |
48 |
GLYFORM |
43 |
Tablets |
|
7 |
Gelcid Syrup |
Antacid |
80 |
ALUMICO |
45 |
BICOLON |
20 |
ALMASIM |
18 |
Syrup |
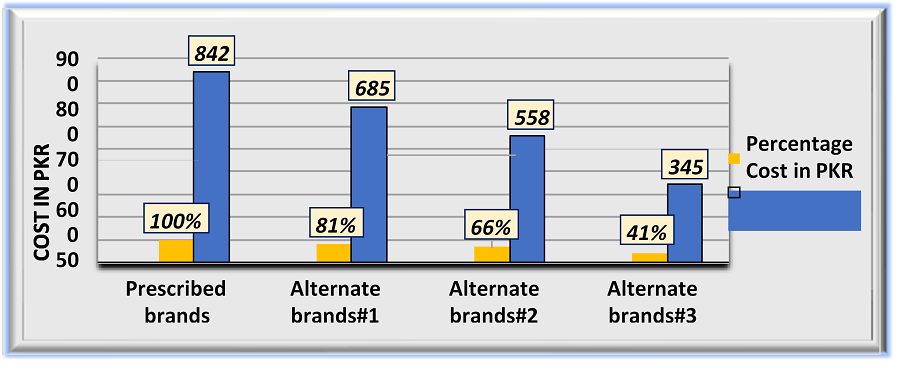
Figure 5. Cost Comparison of Prescription-1 for Diabetes
Table 7 shows the prescribed medicines for diabetes, their respective alternatives, and prices. Figure 1 evaluates the total cost differences. The prescribed brands cost 842 PKR. If the alternate brand #1 is selected, which would cost 685 PKR (81% of the 842 PKR), 19% (159 PKR) can be saved. Alternate brand #2 can save 44% (370 PKR), and alternate brand #3 would save 59% (496 PKR) in a single prescription filling.
Table 7. Price Comparison of Prescribed Brands with Available Alternate in Prescription-2 for Diabetes
|
Sr. no. |
Prescribed Brands |
Generics |
Price |
Alternate brands#1 |
Price |
Alternate brands#2 |
Price |
Alternate brand#3 |
Price |
Dosage forms |
|
1 |
Inosita |
Sitagliptin |
740 |
SITA MET |
395 |
GLYZIAMET |
350 |
GLIPTIN PLUS |
210 |
Tablets |
|
2 |
Gilap |
Glimepiride |
420 |
DAZEMEP |
200 |
A-GLIM |
100 |
AMARIT |
56 |
Tablets |
|
3 |
Zoblin |
Pregabalin |
570 |
ZEEGAP |
345 |
NERGAB |
325 |
BREGLIN |
200 |
Tablets |
|
4 |
NEXUM |
Esomeprazole Magnesium |
400 |
X-PRAZOLE |
300 |
KONCEPT |
285 |
Esoral |
119 |
Tablets |
|
5 |
ZANLAN |
Cetirizine (10mg) |
65 |
ZINE |
33 |
Rex (10mg) |
29 |
ASKOGIX |
16 |
Tablets |
|
6 |
Hydrelin |
Mynophyline plus Compound syrup |
69 |
COLDREX-E |
29 |
BROXOL |
20 |
ROFLIN |
17 |
syrup |
|
7 |
Nise |
Nimesulide (100mg) |
140 |
MESULID |
100 |
NEMSIS |
90 |
NIROX |
45 |
|
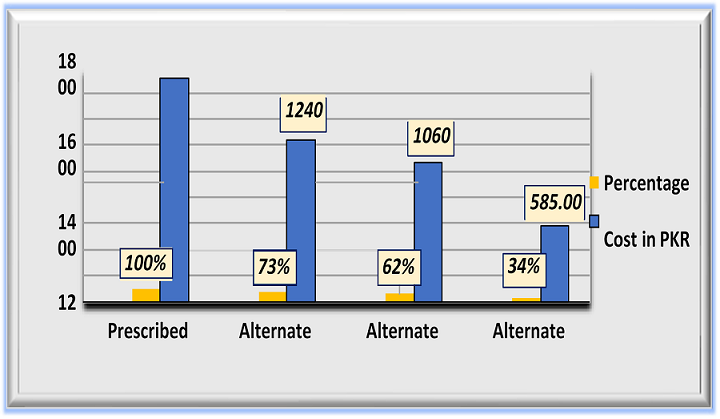
Figure 6. Cost Comparison of Prescription-2 for Diabetes
Table 8 shows the prescribed medicines for diabetes, their respective alternatives, and prices. Figure 2 evaluates the total cost differences. The prescribed brands cost 1710 PKR. If the alternate brand #1 is selected, which would cost 1240 PKR (73% of the 1710 PKR), 27% (461 PKR) can be saved. Alternate brand #2 can save 38% (649 PKR), and alternate brand #3 would save 66% (1128 PKR) in a single prescription filling.
3.4. Paediatrics
Table 8. Price Comparisonof Prescribed Brands with Available Alternate in Prescription-1 for Paediatrics
|
Sr. no. |
Prescribed brands |
Generics |
Price |
Alternate brands#1 |
Price |
Alternate brands#2 |
Price |
Alternate brands#3 |
Price |
Dosage Forms |
|
1 |
Amclav |
Co - Amoxicillin |
100 |
Loment |
80 |
Cla |
55 |
Amoxilite plus |
50 |
Syrup |
|
2 |
Panadol |
paracetamol |
100 |
Calpol |
76 |
Disprol |
50 |
Febrol DS |
40 |
Syrup |
|
3 |
Vermox 30 ml |
mebendazole |
50 |
Nemazole |
42 |
Panamox 30ml |
27 |
anthex 30ml |
22 |
Syrup |
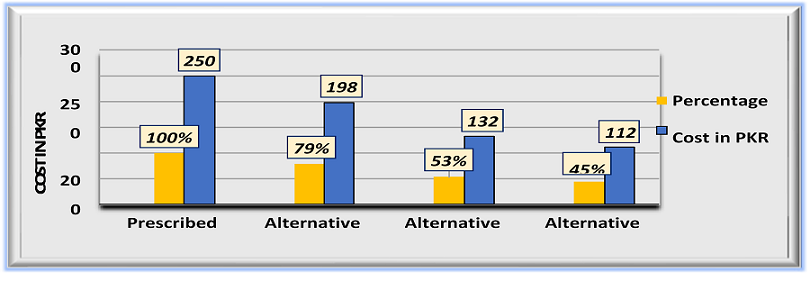
Figure 7. Cost Comparison of Prescription-1 for Paediatrics
Table 9 presents the prescribed medicines for paediatrics, their respective alternatives, and prices. Figure 1 evaluates the total cost differences. The prescribed brands cost 250 PKR. If the alternate brand #1 is selected, which would cost 198 PKR (79% of the 250 PKR), 21% (52 PKR) can be saved. Alternative brand #2 can save 47% (117 PKR), and alternative brand #3 would save 55% (137 PKR) in a single prescription filling.
Table 9. Price comparison of prescribed brands with available alternate in prescription-2 for paediatrics
|
Sr. no. |
Prescribed brands |
Generics |
price |
Alternate brands#1 |
Price |
Alternate brands#2 |
Price |
Alternate brands#3 |
Price |
Dosage forms |
|
1 |
Sunny-D ampule |
cholecalciferol |
736 |
D- tres ampule |
150 |
D- all |
148 |
choltec |
126.00 |
injection |
|
2 |
Monaka 4mg |
Montelukast |
475 |
Montika |
278 |
Floaid |
249 |
Mytika |
222 |
sachet |
|
3 |
Atiza |
levocetirizine |
65 |
Citramacl |
40 |
Histasun |
35 |
Welcet |
30 |
syrup |
|
4 |
Ferricure |
Polysaccharide iron complex |
200 |
Elezo |
150 |
Ben-10 |
135 |
Amrotose |
75 |
syrup |
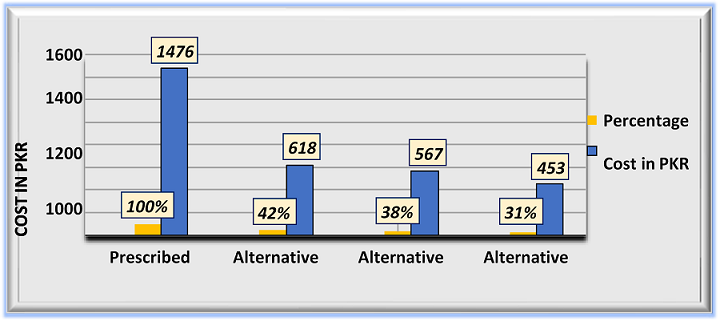
Figure 8. Cost Comparison of Prescription-2 for Paediatrics
Table 10 presents the prescribed medicines for pediatrics, their respective alternatives, and prices. Figure 2 evaluates the total cost differences. The prescribed brands cost 1476 PKR. If the alternate brand #1 is selected, which would cost 618 PKR (42% of the 1476 PKR), 48% (708 PKR) can be saved. For that, alternative brand #2 can save 62% (915 PKR), and alternate brand #3 would save 69% (1018 PKR) in a single prescription filling.
The data collected for the current study was analyzed. The results on average showed about 55% possible reduction in the cost of prescription filling through alternate brands of medicines. The resulting data evaluated for each disease is presented in the tables below.
Table 10. Cost Comparison of Alternate Brands for Diseases
|
Cardiovascular Diseases (CVDs) |
||||
|
S. no. |
Prescribed Cost & (%) |
Alternative one cost & (%) |
Alternative two cost & (%) |
Alternative three cost & (%) |
|
P1 |
921 PKR (100%) |
726 PKR (79%) |
673 PKR (73%) |
595 PKR (65%) |
|
P2 |
1035 PKR (100%) |
850 PKR (82%) |
800 PKR (77%) |
730 PKR (71%) |
|
Diabetes |
||||
|
P1 |
842 PKR (100%) |
685 PKR (81%) |
558 PKR (66%) |
345 PKR (41%) |
|
P2 |
1710 PKR (100%) |
1240 PKR (72%) |
1060 PKR (62%) |
585 PKR (34%) |
|
Pediatrics |
||||
|
P1 |
250 PKR (100%) |
198 PKR (79%) |
132 PKR (52%) |
112 PKR (44%) |
|
P2 |
1476 PKR (100%) |
618 PKR (41%) |
567 PKR (38%) |
453 PKR (30%) |
|
Neurological Disorder |
||||
|
P1 |
1875 PKR (100%) |
677 PKR (36%) |
774 PKR (41%) |
915 PKR (49%) |
|
P2 |
2441 PKR (100%) |
946 PKR (39%) |
776 PKR (32%) |
725 PKR (30%) |
The current study demonstrated that the prescribed brands are more expensive as compared to the available alternate brands. It is common practice for practitioners to prescribe expensive brands even when less costly or cheaper brands are available. There are too many variations in the prices of different brands with the same formulations. Unlike many developed countries, there is no generic prescription in Pakistan to reduce the cost. For many patients, it is impossible to afford these expensive brands and they opt to skip or leave the therapy due to the high cost. Similar concerns and questions are seen arising in the society regarding particular brand prescription. The current study was conducted to find answers to questions raised on the healthcare system of Pakistan. Furthermore, it also aimed to convey these concerns to responsible authorities and to the general public in order to understand the benefits of the generic prescription.
Manufacturing companies and distributors mainly promote their brands and increase their sales production by convincing practitioners to prescribe their medicines instead of any other medicines that may be less expensive. The practitioners still prescribe costly brands and there are mixed reasons for their practice. One factor is the drug's safety, efficacy, and potency ensured by the expensive brands, which the cheaper brands may not clarify. Other factors include the brands' availability and personal benefits, contributing to the costly prescription [13]. Incentives provided by pharmaceutical industries or distributors directly or indirectly to the prescribers ultimately lead towards unjustified brand choice, costing the patients considerable resources [14]. A study has compared brand writing versus generic prescription in diabetic and hypertensive patients. After months of treatment with branded and generic drugs for two groups, no significant differences were observed in clinical parameters [15]. In some cases, the use of well-known brands might be advantageous. For instance, in the case of inhalers, the quality of container could affect the dosage [16].
Variations in prices of different brands result from the manufacturing cost, quality control measures, ensuring safety, efficacy, use of correct formulations, and dosage form by the manufacturer. Other factors include external pressure, competition, manufacturing company's location, and marketing costs [17], as these factors may differ for industries. The healthcare system of Pakistan has many gaps as compared to developed countries. Besides, the budget for health, one reason that may reduce the expenses of the therapy and selecting the affordable drug for a patient is the induction of pharmacists into the healthcare system of Pakistan. This is because in Pakistan, pharmacists are not consulted to take advantage from their knowledge pertaining to drugs and cost-effective therapies. Once a pharmacist is induced into the healthcare system, the implementation of the generic prescription would become easier. This is because the pharmacist would help in policymaking about generic prescription. Moreover, he/she would also have strong support. The health regulatory authority must develop policies regarding generic prescriptions and limit the cost of medicines that may be affordable for poor patients. Overall, a high level of satisfaction was reported in multiple studies where patients switched to generic medicine from brand prescribed medicines [18].
3.5. Conclusion
The current study concluded that the cost of prescribed brands available for CVDs, diabetes, and neurological disorders is high in comparison to the alternate brands available in the market. There are several contributing factors to the increased cost of these prescribed brands. These include lack of qualified individuals in most retail and community pharmacies, unavailability of alternative drugs, attraction of promotional activities for prescribers, pharmaceutical pressure, and lack of policy implementation regarding the filling of prescriptions.
3.6. Recommendations
- The availability of a qualified individual for the intervention of the prescribed brand and to provide cost-effective therapy.
- The prescription should be generic drug-oriented instead of brand orientation.
- DRAP should actively play its role to minimize the price gap.
- Drug testing laboratories should be appropriately equipped and be functional to ensure the quality of all the available brands.
- To increase the number of qualified pharmacists in the existing healthcare system and discourage irrational prescribing patterns.
- Policies regarding the promotion of pharmaceutical products should be made and implemented for the community's better social and mental health.
- The government should minimize shifting charges on the raw material to reduce the overall cost of therapy.
- Industrial production of raw material should be encouraged at government level through attractive packages.
- While prescribing the medicines, practitioners should consider the patient's socio-economic status.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding details
This research did not receive grant from any funding source or agency.
Bibliography
- Hassali MA, Shafie AA, Jamshed S, Ibrahim MI, Awaisu A. Consumers' views on generic medicines: a review of the literature. Int J Pharm Pract. 2009;17(2):79–88. https://doi.org/10.1211/ijpp.17.02.0002
- Girardin FR, Cohen K, Schwenkglenks M, Durand-Zaleski I. Pharmacoeconomics in the era of health technology assessment and outcomes research to prioritize resource use, innovation and investment. Front Pharmacol. 2023;14:e1210002. https://doi.org/10.3389/fphar.2023.1210002
- Atif M, Azeem M, Sarwar MR. Potential problems and recommendations regarding substitution of generic antiepileptic drugs: a systematic review of literature. Springerplus. 2016;5:1–8. https://doi.org/10.1186/s40064-016-1824-2
- World Health Organization. Progress in Essential Drugs and Medicines Policy: 1998–1999. World Health Organization; 2000.
- World Health Organization. Cardiovascular diseases (CVDs). WHO Web site. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds). Accessed May 20, 2024.
- Rattani SA. Case Study Describing Access to Palliative Care in Pakistan [doctoral thesis]. Pakistan: Aga Khan University; 2020.
- Jafar TH, Haaland BA, Rahman A, et al. Non-communicable diseases and injuries in Pakistan: strategic priorities. Lancet. 2013;381(9885):2281–2290. https://doi.org/10.1016/S0140-6736(13)60646-7
- Lozano R, Naghavi M, Foreman K, Lim S. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. https://doi.org/10.1016/S0140-6736(12)61728-0
- Wood L. A review on adherence management in patients on oral cancer therapies. Eur J Oncol Nurs. 2012;16(4):432–438. https://doi.org/10.1016/j.ejon.2011.10.002
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. https://doi.org/10.1016/S1474-4422(18)30499-X
- Premnath K, Arunprasath K, Sanjeevi R, Elilvanan R, Ramesh M. Natural/synthetic fiber reinforced hybrid composites on their mechanical behaviors–a review. Interactions. 2024;245(1):e111. https://doi.org/10.1007/s10751-024-01924-y
- Reichert T. The prevalence of sexual imagery in ads targeted to young adults. J Consum Aff. 2003;37(2):403–412. https://doi.org/10.1111/j.1745-6606.2003.tb00460.x
- Reichert S, Simon T, Halm EA. Physicians' attitudes about prescribing and knowledge of the costs of common medications. Arch Intern Med. 2000;160(18):2799–2803. https://doi.org/10.1001/archinte.160.18.2799
- Zarei E, Ghaffari A, Nikoobar A, Bastami S, Hamdghaddari H. Interaction between physicians and the pharmaceutical industry: a scoping review for developing a policy brief. Front Public Health. 2023;10:e1072708. https://doi.org/10.3389/fpubh.2022.1072708
- Premanath M, Kulkarni P. Generic drugs or branded generics, which one you prefer to prescribe? APIK J Intern Med. 2024;12(3):195–196. https://doi.org/10.4103/ajim.ajim_119_23
- Chrystyn H, Price D. Not all asthma inhalers are the same: factors to consider when prescribing an inhaler. Prim Care Respir J. 2009;18(4):243–249. https://doi.org/10.4104/pcrj.2009.00029
- Yu LX. Pharmaceutical quality by design: product and process development, understanding, and control. Pharm Res. 2008;25:781–791. https://doi.org/10.1007/s11095-007-9511-1
- Valles JA, Barreiro M, Cereza G, et al. Acceptance of generic prescribing in general practice: effect of patient education and reference prices. Gac Sanit. 2002;16(6):505–510. https://doi.org/10.1016/s0213-9111(02)71972-9