Evaluation of Viola canescens Wall Ex. Roxb. for Anti-asthmatic and Antitussive Activities and Isolation of Bioactive Compound
Abdullah11*, Irfan Ullah1, Waqar Ahmad1, Muhammad Ibrar2and Bashir Ahmad33
1Department of Pharmacy, University of Malakand, Chakdara Dir Lower, Pakistan
2Department of Pharmacy, Bacha Khan University, Charsadda, Pakistan
3Department of Zoology, University of Malakand, Chakdara Dir Lower, Pakistan
Abstract
Folklorically, Viola canescens (VC) is used for the treatment of respiratory disorders, such as cough and asthma. The current study aimed to evaluate VC for anti-asthmatic and anti-tussive activities and isolate the bioactive compound. The plant was collected, extracted, and fractionated, with the isolation of compounds via column chromatography. Solvent extracts of VC were evaluated for anti-asthmatic and anti-tussive activities in animal models. The purified compound obtained from ethyl acetate fraction (EF) via column chromatography was identified by Mass and 1H-NMR spectroscopic techniques. The EF (at 200 mg/kg/day for 21 days) significantly increased latency to pre-convulsive dyspnea (PCD) as compared to control. Similarly, mucous viscosity of the sensitized group was reduced significantly by EF (at 200 mg/kg). In isolated guinea pig’s ileum preparation, the EF (at 25 μg/ml) exhibited maximum relaxant activity (48.83 ± 1.5% inhibition at 0.8 ml) against histamine-induced contractions (p<0.01). The citric acid-induced cough bouts in guinea pigs were significantly reduced by EF (58.13 ± 3.1% at 200 mg/kg). The EF also significantly inhibited the secretion of phenol red dye (43.02 ± 3.1% at 200 mg/kg). A flavonoid (quercetin) was isolated from the EF that may be probably responsible for anti-asthmatic and anti-tussive activities of the plant.
1. Introduction
The history of the use of medicinal plants for the treatment of different diseases is as old as man himself. During the past few decades, the use of herbal medicine has been revived due to multiple reasons [1]. Globally, respiratory diseases are the significant and one of the most common causes of morbidity and mortality. In Pakistan, acute respiratory infections represent 30-60% of outdoor patients in hospitals [2]. Common respiratory diseases include common cold, cough, bronchitis, asthma, and whooping cough. Worldwide, asthma affects approximately 262 million people, causing 4.5 million deaths, and the number of patients is expected to increase over time [3]. In Pakistan, the prevalence of asthma is increasing day by day with 5% annual increment, out of which 20-30% are children. It has been reported that 12% of Pakistan’s adult population is suffering from asthma [4].
Respiratory passages become over-responsive in asthma, accompanied by increased mucus production which results in episodic coughing, wheezing, and shortness of breath. Cough is also a respiratory disease caused by different etiological agents. It may coexist with asthma and reduce the quality of life significantly [5]. Cough affects about 40% of the world’s population. Drugs having anti-tussive activity are often used in asthma [6]. Herbal medicine is increasingly used in the treatment of asthma and cough due to cultural practices and beliefs, supposed few adverse effects, active marketing by manufacturers, and the relatively low cost [6, 7]. The current treatment of asthma involves only symptomatic relief by the administration of corticosteroids and anti-inflammatory drugs in combination with bronchodilators, such as 𝛽2-adrenergic agonists. Therefore, there is a dire need for better drugs with improved patient compliance that can modify the nature of disease [8, 9].
The emergence of COVID-19 pandemic caused widespread morbidity and mortality worldwide [10]. This situation is extremely alarming for asthmatic patients as COVID-19 aggravates asthma [11]. The Centre for Disease Control and Prevention (CDC) has warned that asthmatic patients are at a high risk of pneumonia and acute respiratory distress caused by COVID-19 pandemic [12]. In this scenario, new strategies for the treatment of asthma are direly needed.
Viola canescens (VC) Wall Ex Roxb. from family Violaceae is a herb that grows in the hilly areas of Khyber Pakhtunkhwa (KPK) in Pakistan [13, 14]. According to the folklore, it is used in the treatment of jaundice and cancer as antipyretic and carminative and also used in various nervous diseases [15, 16]. Furthermore, it is also used to relieve epilepsy, stomach acidity, rheumatism, eczema, respiratory disorders [17, 18], malaria, dysentery. It is also helpful in regulating menstruation, leucorrhoea, aphrodisiac, and headache [18]. VC has been shown to possess antioxidant, membrane stabilizing, hepatoprotective [19], and anti-malarial properties [20]. Secondary metabolites reported in the plant include saponins, phenols, alkaloids, flavonoids, tannins, and triterpenes [19]. No research has been conducted so far on anti-asthmatic and anti-tussive activities of the plant despite its ethnomedicinal usefulness in the treatment of these disorders. Therefore, solvent extracts of the plant were evaluated to test these properties and column chromatography was also carried out for isolation and purification of compound that may be probably responsible for these effects.
2. MATERIALS AND METHODS
2.1. Plant Collection and Extraction
VC was collected in March from Dir Lower, KPK, Pakistan. It was positively identified by taxonomists and voucher specimens submitted to the Herbarium with reference No H. UOM. BG. 277. It was dried under shade, ground, and the powder plant material (4.67 kg) was soaked in commercial-grade methanol for 3 weeks. It was filtered through filter paper and concentrated in rotary evaporator (Heidolph, Laborota 4000 efficient, Germany) to obtain Viola canescens methanolic extract (VCME). This was partitioned in separating funnel to get n-hexane (NHF), chloroform (CF), ethyl acetate (EF), and aqueous fractions (AQF)
2.2. Experimental Animals
Guinea pigs and BALB/c mice were picked up from the Veterinary Research Institute Peshawar and kept in the animal house; served with standard diet with 12/12 h light-dark cycle. Approval from the Research Ethics Committee, Department of Pharmacy, University of Malakand was also obtained (No. DREC/20160503-15).
2.3. Anti-asthmatic Activity
2.3.1. Histamine Induced Pre-convulsive Dyspnea (PCD). Guinea pigs (470-580 g) were randomly grouped into eighteen (n=5). Group I animals, non-sensitized, were orally treated with distilled water (2 ml/kg/day). Group II were ovalbumin (OVA)-sensitized animals, orally given distilled water (2 ml/kg) and group III-V animals were OVA-sensitized, treated with VCME p/o at 50, 100 and 200 mg/kg. While, group VI-VIII were OVA-sensitized animals, administered with NHF at 50, 100, and 200 mg/kg p/o. Similarly, group IX-XI animals were OVA-sensitized, treated with CF at 50, 100, and 200 mg/kg p/o. Group XII-XIV were OVA-sensitized, treated with EF at 50, 100, and 200 mg/kg; group XV-XVII were OVA-sensitized, treated with AQF at 50, 100, and 200 mg/kg. Group XVIII animals were orally administered salbutamol (0.5 mg/kg).
Guinea pig’s sensitization was conducted by treatment with OVA (100 mg/kg i.p) on the 1st day, followed by 50 mg/kg on the 2nd and the 20th day. On the 21st day, 1 h after the last dose, the animals were exposed to histamine dihydrochloride aerosol (0.2%) in a glass chamber until preconvulsive dyspnea (PCD) was observed. After the removal of guinea pigs from the chamber, they were then exposed to fresh air for recovery, followed by determination of the latency to PCD [21, 22].
2.3.2. Determination of WBC and Lymphocyte Count. Blood sample (1 ml) was taken from the abdominal aorta. The number of white blood cells (WBC) and lymphocytes was determined by automated blood analyzer (Hematology analyzer, BK-3200, Biobase China) [23].
2.3.3 Measurement of Mucus Viscosity. Tracheas (2 cm) were isolated from guinea pigs up to the point of thoracic bifurcation. It was then rinsed with normal saline (2 ml) for five minutes, followed by viscosity determination of the tracheal fluid [24]. Briefly, fluid from trachea (1.0 ml) was obtained by 1.0 ml syringe. The needle point of the syringe was kept downwards in a stand. The syringe plunger was carefully removed and the fluid was allowed to drop under gravity. The emptying time of tracheal fluid out of syringe was noted using a stopwatch. The flow rate was used as viscosity index and calculated as vol/sec (ml/sec) by formula [24].
2.3.4. Ex-vivo Anti-asthmatic Activity. After dissecting the abdomen of guinea pigs, ileum was removed and shifted to an organ bath containing Tyrode’s solution (15 ml), maintained at 37 ± 1°C temperature and continuously aerated. The dose-response curve for histamine was determined in Tyrode solution containing VC (25 μg/ml) and the response to drugs was determined on kymograph (Student kymograph, Pan Lab S.L Energia, Barcelona Spain). The tissue was equilibrated for 30 minutes and the solution was changed at 10 minutes interval. Histamine-induced (2.5 μg/ml) contractile responses of ileum in the presence and absence of the various fractions of VC were determined [25].
2.4. Anti-tussive Evaluation
Citric acid and phenol red expectoration models were used for the evaluation of anti-tussive activity.
2.4.1. Citric Acid-induced Cough. Guinea pigs were exposed to citric acid (7.5% aerosol) one day prior to experiment for five minutes and the number of cough bouts was noted. Animals exhibiting cough bouts of 13 ± 5 were erratically grouped into seventeen (n=5) and were orally administered various fractions of VC for one week. Group I animals were administered distilled water p/o (2 ml/kg/day), groups II-IV were orally treated with VCME 50, 100, and 200 mg/kg, and groups V-XVI were administered NHF, CF, EF, and AQF at 50, 100, and 200 mg/kg daily. While, group XVII administered codeine phosphate (25 mg, p.o). On the 7th day, 1 h after the administration of last dose, animals were re-exposed to 7.5% citric acid aerosol followed by counting the numbers of bouts of cough. The percentage inhibition of cough bouts was calculated by formula [26].
where, No is the number of cough bouts before treatment; Nt is the number of cough bouts after treatment.
2.4.2. Phenol Red Expectoration. Mice (20-30 g) were randomly grouped into seventeen (n= 5). The experiment was carried out for seven consecutive days [27]. Group I animals were administered with distilled water (2 ml/kg/day, p.o), groups II-IV were orally treated with VCME at 50, 100, and 200 mg/kg, and group V-XVI were administered NHF, CF, EF, and AQF at 50, 100, and 200 mg/kg daily. Group XVII was treated with sodium cromoglycate (50 mg, i.p).
On the 7th day, 1 h after the administration of last dose, ammonium chloride (5 mg/kg) was orally administered to all groups. After 30 minutes of ammonium chloride administration, phenol red (0.5 g/kg) was administered intraperitoneally to all groups. All the animals were euthanized by cervical dislocation and their trachea was cut down and placed in normal saline (2 ml) separately in test tubes. Sodium hydroxide (0.1 ml, 1 N) was added to stabilize the pH and the absorbance of dye secreted from trachea was measured at 460 nm by UV-visible spectrophotometer [28].
where, Cc is the concentration of dye secreted in control group and Ct is the concentration of dye secreted in test group.
2.5. Column Chromatography and Isolation of Compound
The column chromatography of EF was done using silica gel by employing slurry method. The column was eluted with pure n-hexane, followed by ethyl acetate: n-hexane, gradually increasing the polarity of the mixture and was finally eluted with 100% ethyl acetate. The eluates were concentrated separately in a rotary evaporator at 40°C, followed by TLC analysis [29, 30]. Fractions with same Rf were pooled for further chromatography. The 90% EF of VC was re-chromatographed and eluted with 5% ethyl acetate: hexane, and then collected in vials and dried. Chromatography continued until pure compound was obtained.
2.6. Statistical Analysis
Statistical analyses were performed by one-way-ANOVA following post-hoc Tukey test for multiple comparisons via SPSS version 16.
3. RESULTS
3.1. Percentage Yield
The percentage yield of VCME was 8.748% (408.56 g). VCME (70 g) was retained for biological activities, while 338 g was used for fractionation to get 22.6 g n-hexane (6.68%), 7.9 g CF (2.33%), 10.7 g EF (3.17%), and 272 g AQF (80.47%).
3.2. Anti-asthmatic Activity
3.2.1. Effect on Latency to PCD.Figure 1 shows that VC at concentrations of 50, 100, and 200 mg/kg/day significantly inhibited bronchoconstriction induced by histamine as observed from the latency to PCD, compared with the control group. VCME showed 8.06 ± 1.6%, 13.07 ± 2.6%, and 24 ± 2.2%, and CF showed 11.5 ± 2.6%, 19.42 ± 1.5%, and 31 ± 1.8% latency to PCD at 50, 100, and 200 mg/kg, respectively. While, EF exhibited 14.18 ± 1.9%, 22.86 ± 1.5%, and 37.4 ± 3.1% latency to PCD at 50, 100, and 200 mg/kg, respectively.
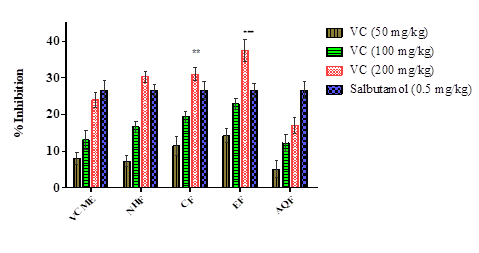
Figure 1.Effect of Viola canescens on Latency to PCD in Guinea Pigs
All values were taken as Mean ± SEM. Statistical analysis was performed by one-way ANOVA following post-hoc Tukey test, where *** = p < 0.001, ** = p < 0.01 as compared to control.VC, Viola canescens; VCME, Viola canescens methanolic extract; NHF, n-hexane fraction; CF, chloroform fraction; EF, ethyl acetate fraction; AQF, aqueous fraction.
3.2.2. Effect on WBC and Lymphocyte Counts. There was no significant change in lymphocyte and total number of WBC as shown in Table 1. Highest average WBC number was observed in the OVA group and lowest in the control group.
Table 1.Effect of Viola canescens on WBC and Lymphocyte Counts of Guinea Pigs| Groups | Dose (Quantity/kg/day) |
WBC counts (cmm) |
Lymphocyte counts (%) |
|---|---|---|---|
| NHF | Control (2 ml DW) | 3100 | 44 |
| Sensitized (2 ml DW) | 4200 | 38 | |
| NHF (50 mg) | 3900 | 36 | |
| NHF (100 mg) | 3700 | 47 | |
| NHF (200 mg) | 3400 | 48 | |
| Salbutamol (0.5 mg) | 3500 | 41 | |
| CF | Control (2 ml DW) | 3100 | 44 |
| Sensitized (2 ml DW) | 4200 | 38 | |
| CF (50 mg) | 3800 | 34 | |
| CF (100 mg) | 3700 | 42 | |
| CF (200 mg) | 3300 | 40 | |
| Salbutamol (0.5 mg) | 3500 | 41 | |
| EF | Control (2 ml DW) | 3100 | 44 |
| Sensitized (2 ml DW) | 4200 | 38 | |
| EF (50 mg) | 3800 | 39 | |
| EF (100 mg) | 4000 | 43 | |
| EF (200 mg) | 3800 | 49 | |
| Salbutamol (0.5 mg) | 3500 | 41 | |
| AQF | Control (2 ml DW) | 3100 | 44 |
| Sensitized (2 ml DW) | 4200 | 38 | |
| AQF (50 mg) | 4200 | 37 | |
| AQF (100 mg) | 4000 | 42 | |
| AQF (200 mg) | 3800 | 36 | |
| Salbutamol (0.5 mg) | 3500 | 41 | |
| VCME | Control (2 ml DW) | 3100 | 44 |
| Sensitized (2 ml DW) | 4200 | 38 | |
| VCME (50 mg) | 4200 | 41 | |
| VCME (100 mg) | 3900 | 42 | |
| VCME (200 mg) | 3900 | 36 | |
| Salbutamol (0.5 mg) | 3500 | 41 |
3.2.3. Effect of VC on Mucus Viscosity. The viscosity of mucus in trachea was significantly reduced by various fractions of VC as compared to the sensitized untreated group (Table 2). The activity of CF and EF was significantly higher than other solvent extracts of VC.
Table 1.Effect of Viola canescens on Mucus Viscosity| Groups | Dose (Quantity/kg/day) |
Mucus viscosity (ml/sec) × 103 |
|---|---|---|
| NHF | Control (2 ml DW) | 18.80 |
| Sensitized (2 ml DW) | 13.91 | |
| NHF (50 mg) | 19.32 | |
| NHF (100 mg) | 19.91 | |
| NHF (200 mg) | 20.13 | |
| Salbutamol (0.5 mg) | 21.36 | |
| CF | Control (2 ml DW) | 18.80 |
| Sensitized (2 ml DW) | 13.91 | |
| CF (50 mg) | 19.68 | |
| CF (100 mg) | 20.14 | |
| CF (200 mg) | 20.83 | |
| Salbutamol (0.5 mg) | 21.36 | |
| EF | Control (2 ml DW) | 18.80 |
| Sensitized (2 ml DW) | 13.91 | |
| EF (50 mg) | 19.53 | |
| EF (100 mg) | 20.04 | |
| EF (200 mg) | 20.72 | |
| Salbutamol (0.5 mg) | 21.36 | |
| AQF | Control (2 ml DW) | 18.80 |
| Sensitized (2 ml DW) | 13.91 | |
| AQF (50 mg) | 18.84 | |
| AQF (100 mg) | 18.90 | |
| AQF (200 mg) | 19.49 | |
| Salbutamol (0.5 mg) | 21.36 | |
| VCME | Control (2 ml DW) | 18.80 |
| Sensitized (2 ml DW) | 13.91 | |
| VCME (50 mg) | 18.83 | |
| VCME (100 mg) | 19.11 | |
| VCME (200 mg) | 20.09 | |
| Salbutamol (0.5 mg) | 21.36 |
3.2.4. Ex-vivo Anti-asthmatic Activity. Histamine-induced contraction of isolated guinea pig ileum preparation was significantly inhibited by VC (25 μg/ml) (Figure 2), showing its H1 receptor antagonistic activity that is responsible for anti-asthmatic activity. VCME exhibited 37.5 ± 2.6% and EF showed 48.14 ± 1.5% inhibition of histamine-induced contraction of guinea pig ileum at 200 mg/kg as compared to control (p < 0.01).
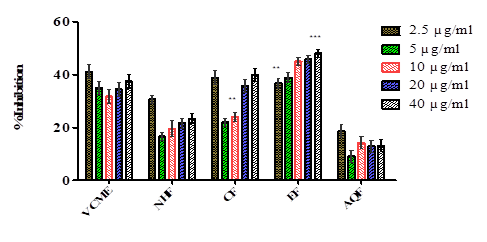
Figure 2.Percent Inhibition of V. canescens on Histamine-induced Contraction in Guinea Pig Ileum
All values were taken as Mean ± SEM. Statistical analysis was performed by one-way ANOVA following post-hoc Tukey test, where *** = p < 0.001, ** = p < 0.01 as compared to control.
3.3. Anti-tussive Activity
3.3.1. Effect of VC on Cough. Figure 3 shows that VC exhibited dose-dependent inhibition of cough induced by citric acid. VCME showed 24 ± 2.6%, 38.83 ± 2.4%, and 41.74 ± 2.6% inhibition, while EF exhibited 47.91 ± 1.7%, 51.15 ± 1.9%, and 58.13 ± 3.1% inhibition at 50, 100, and 200 mg/kg, respectively. While, codeine phosphate inhibited 65.69 ± 2.3% of citric acid-induced cough at 25 mg/kg.
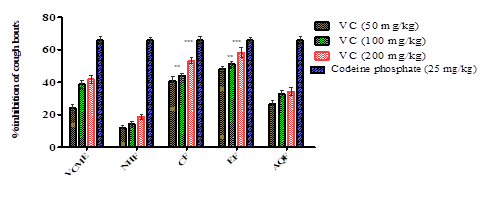
Figure 3.Effect on Citric Acid-induced Cough Bouts
All values were taken as Mean ± SEM. Statistical analysis was performed by one-way ANOVA following post-hoc Tukey test, where *** = p < 0.001, ** = p < 0.01 as compared to control.
3.3.2. Effect of VC on Phenol Red Dye Secretion in Mice. VC exhibited dose-dependant inhibition of phenol red dye secretion in mice as compared to control (Figure 4). VCME demonstrated 8.23 ± 2.6%, 10.23 ± 2.1%, and 19.52 ± 1.3% inhibition of phenol red secretion at 50, 100, and 200 mg/kg, respectively. EF exhibited 14.5 ± 1.9%, 27.3 ± 1.4%, and 43.02 ± 3.1% inhibition of dye at 50, 100, and 200 mg/kg, respectively. While, sodium cromoglycate inhibited 32.14 ± 2.3% of phenol red dye secretion into tracheal fluid at 50 mg/kg.
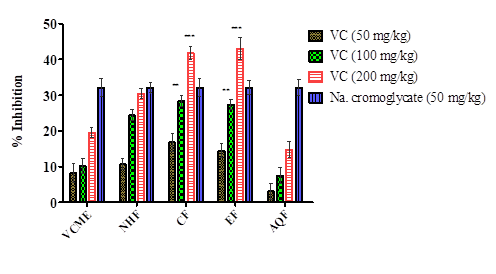
Figure 4.Percent Inhibition of Phenol Red Dye Secretion in Mice
3.4. Compound Isolation
The isolated compound was obtained as yellow amorphous powder, soluble in acetone with melting point 316°C, molecular weight 302, and molecular formula C15H10O7.
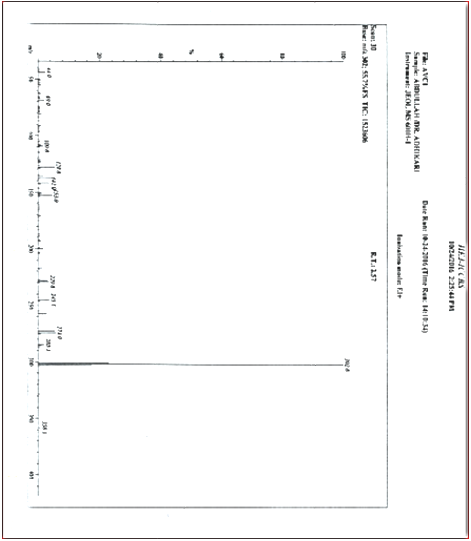
3.4.1. Mass Spectra of Isolated Compound. The molecular ion peak in the EI-MS spectrum of the compound was at m/z 302.0 and the other peaks were visible at m/z 128, 142, 153, 229, 245, and 274 (Supplementary data).
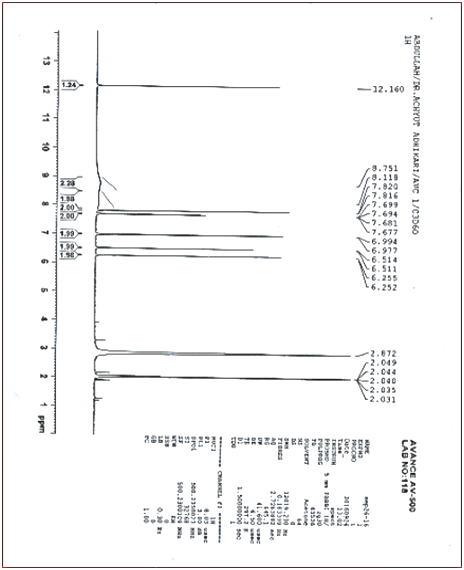
3.4.2. Proton NMR Spectrum of Compound. The P-NMR data of isolated compound matched with the previously reported one. Proton NMR spectrum of the compound (in acetone-d6 at 400 MHz) exhibited chemical shift values δ 6.85 (1H, d, J = 8.0 Hz, H-5'), 7.55 (1H, dd, J = 8.0, 2.0 Hz, H-6'), 6.37 (1H, J = 2.0 Hz, H-8), 7.67 (1H, d, J = 2.0 Hz, H-26.12 (1H, d, J = 2.0 Hz, H-6), 12.16 (s, H5/OH) (Supplementary data).
3.4.2. Proton NMR Spectrum of Compound. The P-NMR data of isolated compound matched with the previously reported one. Proton NMR spectrum of the compound (in acetone-d6 at 400 MHz) exhibited chemical shift values δ 6.85 (1H, d, J = 8.0 Hz, H-5'), 7.55 (1H, dd, J = 8.0, 2.0 Hz, H-6'), 6.37 (1H, J = 2.0 Hz, H-8), 7.67 (1H, d, J = 2.0 Hz, H-26.12 (1H, d, J = 2.0 Hz, H-6), 12.16 (s, H5/OH) (Supplementary data).
4. DISCUSSION
Respiratory diseases are increasing due to uncontrolled pollution that has attracted the attention of scientists recently [31, 32]. The current study showed that the solvent extracts of VC inhibit histamine-induced bronchoconstriction in guinea pigs and prevent chemical-induced cough. It has already been determined in the published researches that VC extracts have a wide margin of safety up to 2 g/kg body weight [19].
Ovalbumin-induced sensitization of guinea pigs is a widely accepted model of asthma [33, 34]. The EF exhibited an increased latency to PCD which denotes the inhibition of bronchospasm caused by histamine which is in corroboration with the previous studies [22]. Histamine and other spasmogens activate the release and utilization of calcium that increase the contraction of smooth muscle of respiratory passage [35]. VC has shown antispasmodic activity by ameliorating the responses to histamine and relaxing guinea pig ileum. This activity is probably mediated by flavonoids (quercetin) present in VC to inhibit calcium entry into the smooth muscles [36]. VC contains flavonoids which are already known as bronchodilators [37]. Among several anti-asthmatic effects, flavonoids block histamine release from mast cells and thus, hinder histamine-induced bronchoconstriction [38, 39]. Quercetin was isolated from the ethyl acetate fraction of VC for the first time which is known to exhibit bronchodilator effect [40, 41]. Several medicinal plants with similar phytochemicals to VC have exhibited anti-asthmatic activity [34, 42].
Agents that decrease the viscosity of tracheal fluid are beneficial in asthma as mucus plugging of bronchial passages occur in this disease. It was determined that the viscosity of tracheal fluid was reduced by VC extracts, particularly the EF. Moreover, VC has high concentration of flavonoids and polyphenols which have antisecretory potential [19, 43]. The antioxidant potential of VC is also one of the contributing factors to anti-asthmatic activity [44, 45].
In the current study, citric acid-induced cough model was employed, which was significantly inhibited by VC in a dose-dependent fashion. It was reported that cough induced by chemicals is analogous to the physiological events occurring in human beings [46]. Cough reflex involves central or peripheral mechanism. Anti-tussive activity in the current study shows that VC decreased the number of cough bouts and the amount of phenol red dye secreted by the trachea. As the viscosity of mucus and its secretion is reduced, consequently decreasing the resistance to airflow and thus, irritation, which may result in cough, is also reduced. Additionally, the inhibition of cough bouts also involves central pathway as codeine acts centrally [47]. This shows that VC inhibits cough by peripheral and central mechanisms.
4.1. Conclusion
VC exhibits anti-asthmatic and anti-tussive activities by peripheral and central mechanism. Moreover, the viscosity of mucus and its secretion is reduced that decreases air way resistance, and hence irritation, which might result in cough is responsible for antitussive activity. Since this plant is enriched with polyphenols and flavonoids, the isolated compound quercetin (a flavonoid) may be responsible for anti-asthmatic and anti-tussive effects. Furthermore, clinical studies on the plant, its fractions, and isolated compound are needed that may lead towards the development of plant-based anti-asthmatic and anti-tussive drugs.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
All the data is contained in this article and its supplementary file.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Šantić Ž, Pravdić N, Bevanda M, Galić K. The historical use of medicinal plants in traditional and scientific medicine. Psychiatr Danub. 2017;29(4):69–74
- Alamgeer, Younis W, Asif H, et al. Traditional medicinal plants used for respiratory disorders in Pakistan: a review of the ethno-medicinal and pharmacological evidence. Chin Med. 2018;13(48):1–29. https://doi.org/10.1186/s13020-018-0204-y
- Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life‑years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Oncol. 2018;392(10159):1859–1922. https://doi.org/10.1016/S0140-6736(18)32335-3
- Younis W, Asif H, Sharif A, Riaz H, Bukhari IA, Assiri AM. Traditional medicinal plants used for respiratory disorders in Pakistan: a review of the ethno-medicinal and pharmacological evidence. Chin Med. 2018;13(1):1–29. https://doi.org/10.1186/s13020-018-0204-y
- Patadia MO, Murrill LL, Corey J. Asthma: symptoms and presentation. Otolaryngol Clin North Am. 2014;47(1):23–32. https://doi.org/10.1016/j.otc.2013.10.001
- Razzaq S, Nafees AA, Rabbani U, et al. Epidemiology of asthma and associated factors in an urban Pakistani population: adult asthma study‑Karachi. BMC Pulm Med. 2018;18:1–13. https://doi.org/10.1186/s12890-018-0753-y
- Welz AN, Emberger‑Klein A, Menrad K. Why people use herbal medicine: insights from a focus‑group study in Germany. BMC Complement Altern Med. 2018;18:1–9. https://doi.org/10.1186/s12906-018-2160-6
- Chung KF, Caramori G, Adcock IM. Inhaled corticosteroids as combination therapy with β‑adrenergic agonists in airways disease: present and future. Eur J Clin Pharmacol. 2018;18:1–9. https://doi.org/10.1007/s00228-009-0682-z
- Shahid SK. Newer glucocorticosteroids and corticosteroid resistance reversal in asthma. Pharm Pat Anal. 2013;2(3):373–385. https://doi.org/10.4155/ppa.13.14
- Van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS‑CoV‑2 as compared with SARS‑CoV‑1. N Engl J Med. 2020;382(16):1564–1567. https://doi.org/10.4155/ppa.13.14
- Sears MR. Epidemiology of asthma exacerbations. J Allergy Clin Immunol. 2008;122(4):662–668. https://doi.org/10.1016/j.jaci.2008.08.003
- Bousquet J, Jutel M, Akdis CA, et al. ARIA‐EAACI statement on asthma and COVID‐19 (June 2, 2020). Allergy. 2021;76(3):689–697. https://doi.org/10.1111/all.14471
- Abbasi AM, Khan MA, Shah MH, Shah MM, Pervez A, Ahmad M. Ethnobotanical appraisal and cultural values of medicinally important wild edible vegetables of Lesser Himalayas‑Pakistan. J Ethnobiol Ethnomed. https://doi.org/10.1186/1746-4269-9-66
- Masood M, Arshad M, Asif S, Chaudhari SK. Viola canescens: herbal wealth to be conserved. J Bot. 2014;2014:1–6. https://doi.org/10.1155/2014/345451
- Gilani SA, Qureshi RA, Gilani SJ. Indigenous uses of some important ethnomedicinal herbs of Ayubia National Park, Abbottabad, Pakistan. Ethnobot Leaflets. 2006;2006(1):e32.
- Jan G, Khan MA, Gul F. Ethnomedicinal plants used against jaundice in Dir Kohistan valleys (NWFP), Pakistan. Ethnobot Leaflets. 2009;2009(8):e7.
- Ahmed E, Arshad M, Saboor A, et al. Ethnobotanical appraisal and medicinal use of plants in Patriata, New Murree, evidence from Pakistan. J Ethnobiol Ethnomed. 2013;9(1):1–10. https://doi.org/10.1186/1746-4269-9-13
- Hamayun M, Khan SA, Sohn EY, Lee IJ. Folk medicinal knowledge and conservation status of some economically valued medicinal plants of District Swat, Pakistan. Lyonia. 2006;11(2):101–113.
- Khan MA, Ahmad W, Ahmad M, Nisar M. Hepatoprotective effect of the solvent extracts of Viola canescens Wall. ex. Roxb. against CCl₄ induced toxicity through antioxidant and membrane stabilizing activity. BMC Complement Altern Med. 2017;17(1):1–11. https://doi.org/10.1186/s12906-016-1537-7
- Verma G, Dua VK, Agarwal DD, Atul PK. Anti‑malarial activity of Holarrhena antidysenterica and Viola canescens, plants traditionally used against malaria in the Garhwal region of north‑west Himalaya. Malar J. 2011;10:1–5 https://doi.org/10.1186/1475-2875-10-20
- Ge Y, Liu J, Su D. In vivo evaluation of the anti‑asthmatic, antitussive and expectorant activities of extract and fractions from Elaeagnus pungens leaf. J Ethnopharmacol. 2009;126(3):538–542. https://doi.org/10.1016/j.jep.2009.08.042
- Salami EO, Ozolua RI, Okpo SO, Eze GI, Uwaya DO. Studies on the anti‑asthmatic and antitussive properties of aqueous leaf extract of Bryophyllum pinnatum in rodent species. Asian Pac J Trop Med. 2013;6(6):421–425. https://doi.org/10.1016/S1995-7645(13)60067-X
- Ozolua R, Okolie N, Ebeigbe A, Karikari N. Effects of sub‑chronic oral cyanide on endothelial function in rabbit aortic rings. Hum Exp Toxicol. 2007;26(2):105–110. https://doi.org/10.1177/0960327107071865
- Leonard R. Simple technique for measuring serum or plasma viscosity with disposable apparatus. Br Med J. 1981;283(6300):e1154. https://doi.org/10.1136/bmj.283.6300
- Pandit P, Singh A, Bafna A, Kadam P, Patil M. Evaluation of antiasthmatic activity of Curculigo orchioides Gaertn. rhizomes. Ind J Pharm Sci. 2008;70(4):e440. https://doi.org/10.4103/0250-474X.44590
- Nadig P, Laxmi S. Study of anti‑tussive activity of Ocimum sanctum Linn in guinea pigs. Ind J Physiol Pharmacol. 2005;49(2):243–245.
- Engler H, Szelenyi I. Tracheal phenol red secretion, a new method for screening mucosecretolytic compounds. J Pharmacol Methods. 1984;11(3):151–157. https://doi.org/10.1016/0160-5402(84)90033-0
- Lin B‑q, Li P‑b, Wang Y‑g, Peng W, Wu Z, Su W‑w, Ji H. The expectorant activity of naringenin. Pulm Pharmacol Ther. 2008;21(2):259–263. https://doi.org/10.1016/j.pupt.2007.05.001
- Abdullah, Khan MA, Ahmad W, et al. Antioxidant, antinociceptive, anti‑inflammatory, and hepatoprotective activities of pentacyclic triterpenes isolated from Ziziphus oxyphylla Edgew. Drug Chem Toxicol. 2022;45(4):1796–1807. https://doi.org/10.1080/01480545.2021.1880427
- Mujwah AA, Mohammed MA, Ahmed MH. First isolation of a flavonoid from Juniperus procera using ethyl acetate extract. Arab J Chem. 2010;3(2):85–88. https://doi.org/10.1016/j.arabjc.2010.02.003
- Fang Z, Huang C, Zhang J, et al. Traffic‑related air pollution induces non‑allergic eosinophilic airway inflammation and cough hypersensitivity in guinea‑pigs. Clin Exp Allergy. 2019;49(3):366–377. https://doi.org/10.1111/cea.13308
- Zhang Y, Liu Y, Xue Y, Yang L, Song G, Zhao L. Correlational study on atmospheric concentrations of fine particulate matter and children cough variant asthma. Eur Rev Med Pharmacol Sci. 2016;20(12):2650–2654.
- Bramley AM, Langlands JM, Jones AK, et al. Effects of IZP‑94005 (contignasterol) on antigen‑induced bronchial responsiveness in ovalbumin‑sensitized guinea‑pigs. Br J Pharmacol. 1995;115(8):e1433. https://doi.org/10.1111/j.1476-5381.1995.tb16634.x
- Ozolua R, Umuso D, Uwaya D, Modugu A, Oghuvwu S, Olomu J. Evaluation of the anti‑asthmatic and antitussive effects of aqueous leaf extract of Ocimum gratissimum in rodents. Med Arom Plants. 2016;5(1000235):e2167‑0412.1000235. https://doi.org/10.4172/2167-0412.1000235
- Panula P, Chazot PL, Cowart M, et al. International union of basic and clinical pharmacology. XCVIII. Histamine receptors. Pharmacol Rev. 2015;67(3):601–655. https://doi.org/10.1124/pr.114.010249
- Van Den Broucke C, Lemli J. Spasmolytic activity of the flavonoids from Thymus vulgaris. Pharm Weekbl. 1983;5:9–14. https://doi.org/10.3390/biom10060860
- Khan Au, Khan M, Subhan F, Gilani AH. Antispasmodic, bronchodilator and blood pressure lowering properties of Hypericum oblongifolium–possible mechanism of action. Phytother Res. 2010;24(7):1027–1032. https://doi.org/10.1002/ptr.3067
- Delarcina S, Lima‑Landman M, Souccar C, et al. Inhibition of histamine‑induced bronchospasm in guinea pigs treated with Cecropia glaziovi Sneth and correlation with the in vitro activity in tracheal muscles. Phytomedicine. 2007;14(5):328–332. https://doi.org/10.1016/j.phymed.2006.12.022
- Tanaka T, Takahashi R. Flavonoids and asthma. Nutrients. 2013;5(6):2128–2143. https://doi.org/10.3390/nu5062128
- Joskova M, Franova S, Sadlonova V. Acute bronchodilator effect of quercetin in experimental allergic asthma. Bratisl Lek Listy. 2011;112(1):9–12.
- Townsend EA, Emala CW. Quercetin acutely relaxes airway smooth muscle and potentiates β‑agonist‑induced relaxation via dual phosphodiesterase inhibition of PLCβ and PDE4. Am J Physiol Lung Cell Mol Physiol. 2013;305(5):L396–L403. https://doi.org/10.1152/ajplung.00125.2013
- Nagore D, Ghosh V, Patil M. Evaluation of antiasthmatic activity of Cassia sophera Linn. Pharmacognosy Mag. 2009;5(19s):109–118.
- Lago JHG, Toledo‑Arruda AC, Mernak M, et al. Structure‑activity association of flavonoids in lung diseases. Molecules. 2014;19(3):3570–3595. https://doi.org/10.3390/molecules19033570
- Riccioni G, Barbara M, Bucciarelli T, di Ilio C, D’Orazio N. Antioxidant vitamin supplementation in asthma. Ann Clin Lab Sci. 2007;37(1):96–101.
- Shaheen SO, Sterne JA, Thompson RL, et al. Dietary antioxidants and asthma in adults: population‑based case–control study. Am J Respir Crit Care Med. 2001;164(10):1823–1828. https://doi.org/10.1164/ajrccm.164.10.2104061
- Canning BJ. The cough reflex in animals: relevance to human cough research. Lung. 2008;186(Suppl 1):23–28. https://doi.org/10.1007/s00408-007-9054-6
- Bush AJFP. Pathophysiological mechanisms of asthma. Front Pediatr. 2019;7:e68. https://doi.org/10.3389/fped.2019.00068
SUPPLEMENTARY DATA
Mass Spectrum of Isolated Compound
11H-NMR Spectrum of Isolated Compound