Treatment of Children with Pneumonia and Underlying Causes of Recurrent Pneumonia at a Paediatric Hospital in Abbottabad, Pakistan
Fiaz Alam*, Salman Munawar, Anwar, Fahad khan, Khadifa Shakeel, and Laraib Ejaz
Department of Pharmacy, COMSATS University Islamabad, Abbottabad Campus, Abbottabad, Pakistan
Abstract
The current study aimed to examine the prescribed drugs, the underlying reasons of recurrent pneumonia in children, and the usage of over-the-counter (OTC) cough suppressants as a supplement to antibiotics for paediatric acute pneumonia. During the study period of one year, more than 420 cases were analyzed comprising 194 males (46.1%) and 226 females (53.8%). Eight drugs were prescribed from Essential Drug List (EDL), while 20 were not prescribed from EDL. The most common prescribed medication included ceftriaxone (inj) 280 times, followed by dexamethasone sodium phosphate 42 times. The most common OTC given was paracetamol 226 times followed by Ibuprofen 137 times. In 96.4% cases, nebulizer ventolin was used to control asthma. The current study identified immunodeficiency, aspiration, and structural abnormalities as significant factors for recurrent pneumonia. The analysis revealed frequent use of antibiotics and OTC medications for symptom management. Understanding these treatment patterns and the role of OTC cough medications as adjuncts to antibiotics may help optimize therapeutic strategies and improve clinical outcomes in pediatric pneumonia
1. Introduction
Pneumonia, a widespread and potentially life-threatening respiratory infection, presents a complex and multi-faceted challenge to global public health. It is a common respiratory infection characterized by the inflammation of lungs. It can affect individuals of all ages, however, it is particularly dangerous for young children, the elderly, and those with weakened immune systems [1]. Pneumonia is a significant public health concern worldwide, contributing to substantial morbidity and mortality, particularly in developing countries and among vulnerable populations. Understanding the epidemiology of pneumonia is crucial to implement effective prevention and control strategies [2].
Pneumonia can be caused by various infectious agents including bacteria, viruses, fungi, and parasites. Common pathogens responsible for pneumonia include Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae. Risk factors for developing pneumonia include age (very young or elderly), smoking, chronic lung diseases, weakened immune system, recent respiratory infections, and exposure to certain environmental pollutants [1, 3]. Age and general condition of patient may affect the symptoms of pneumonia. Fever, cough (which may create phlegm), chest pain, shortness of breath, exhaustion, and occasionally disorientation are typical symptoms of pneumonia, particularly in elderly persons [4]. A combination of clinical assessment, physical examination, and diagnostic testing is usually used to diagnose pneumonia. Chest X-rays, blood tests (including complete blood counts and blood cultures), sputum cultures, and sometimes CT scans or bronchoscopies are needed [5].
Antibiotics for bacterial pneumonia, antiviral drugs for viral pneumonia, and supportive care to reduce symptoms are frequently used in the treatment of pneumonia. Hospitalization may be required in extreme situations or when complications develop to provide close observation and intravenous antibiotics [6]. Typically, adults have lower incidence rates of pneumonia as compared to children. Pneumonia is more prevalent in young children (especially those under five years old) and the elderly population. While risk factors, such as age, chronic health conditions, and weakened immune systems are common across age groups, children may be more susceptible due to developing immune systems and increased exposure to respiratory pathogens in day-care or school settings [7]. Respiratory syncytial virus (RSV), influenza virus, Streptococcus pneumoniae, Haemophilus influenzae type b (Hib), and Mycoplasma pneumoniae are commonly associated with paediatric pneumonia [8]. Children with pneumonia may present with fever, cough, rapid or difficulty in breathing, nasal flaring, grunting, chest retractions, and in severe cases, cyanosis or lethargy [9].
Recurrent pneumonia refers to the occurrence of two or more episodes of pneumonia within a defined period, typically over the course of a year or several years. It is distinguished from a single episode of pneumonia by its recurrent nature, which may indicate underlying predisposing factors or conditions that increase the risk of repeated infections [10]. Chronic respiratory conditions, such as chronic obstructive pulmonary disease (COPD), bronchiectasis, cystic fibrosis, or interstitial lung diseases may predispose individuals to recurrent pneumonia [11]. Immune deficiencies, autoimmune diseases, or conditions that weaken the immune system (e.g., HIV/AIDS, immunosuppressive therapy) may increase susceptibility to recurrent infections [12]. Other factors include anatomical abnormalities, aspiration, gastroesophageal reflux disease (GERD), smoking, and environmental factors.
In Pakistan, pneumonia remains a critical health issue, particularly among children under the age of 5. It contributes to a notable percentage of childhood mortality in the country. Contributing factors include limited healthcare access, malnutrition, and suboptimal vaccination rates. National initiatives, such as the Expanded Program on Immunization (EPI), aim to combat pneumonia in Pakistan, however, challenges persist.
This study aimed to investigate deeper into the nuances of pneumonia, encompassing its various types, causes, and management strategies. Moreover, it also explored the available medications for the treatment of pneumonia. For this purpose, it statistically analysed the prescribed medicines and underlying causes of recurrent pneumonia in children as well as over-the-counter (OTC) medications to reduce cough as an adjunct to antibiotics for acute pneumonia in children.
2. METHODS
Prescriptions from various patients served as the study's source material. Data on all prescribed drugs, the underlying causes of recurrent pneumonia in children, and OTC cough suppressants used in conjunction with antibiotics for paediatric acute pneumonia were examined.
2.1. Design
A study period of one year was carried out from September 2023 to August 2024 among the children admitted with the diagnosis of pneumonia in Women and Children Hospital Abbottabad, KP Pakistan. The total sample size included was 420. The prescriptions of children with pneumonia were collected from time to time during the study period irrespective of pneumonia etiology. The reports of patient history were also observed. Children who had chronic respiratory conditions including tuberculosis and chronic suppurative lung disease, as well as comorbid conditions, such as congenital heart disease, listed on the patient history form were not included.
Data Collection Tools
The data collection tools are described as follows:
- Total patients
- Children (males, females)%
- Average age of patients to which drugs were prescribed
- Duration of study
- Duration of therapy
- Percentage of prescribed medicines including the most frequently prescribed medicines
- Approximate daily cases
- OTC prescribed to reduce cough
- Percent of OTC prescribed
- The usage of nebulizer / % of nebulizer used in patients
- Other diseases with pneumonia
- Comparison with Essential Drug List (EDL)
- Data analysis
- Statistics
Medical cases were collected from Women and Children Hospital Abbottabad that is a unit of DHQ Abbottabad. It is a secondary hospital focused on the population of Abbottabad city. The cases were collected from wards by visiting the hospital. Data was collected by trained final year students and supervisor. A data collection form including information on patient’s demographics, clinical features, medications utilized, dosage forms, and evaluation of drug charts using WHO prescription indicators was employed to document the observed data. Data collection included age, sex, disease, previous medication, duration of therapy, and the number of times the disease occurred, current medication, duration of medication and OTC medication [13]. Data included the percentage of prescriptions in which an antibiotic and an injection were prescribed; and the percentage of drugs prescribed from an EDL in Pakistan published by WHO [14]. (https://www.dra.gov.pk/publications/national-essential-medicine-lists/).
2.2. Ethical Considerations
After providing parents or other caregivers with detailed explanations about the goal of study and methods, each participant gave their informed written consent before data was collected. The study was authorized by the Ethical Review Committee of Department of Pharmacy, COMSATS University Islamabad, Abbottabad campus (reference No. PHM.Eth/CF-M04/19-0134).
2.3. Inclusion and Exclusion Criteria
The study included all paediatric ward patients admitted to the in-patient department with a diagnosis of pneumonia as well as those who were prescribed at least one medication. Children with comorbid diseases, such as congenital heart disease, and chronic respiratory conditions, such as tuberculosis and chronic suppurative lung disease, that were noted on the patient history form were excluded. The current study excluded all adult patients, emergency room patients, outpatients, and patients with other respiratory conditions who exhibited symptoms comparable to those of paediatric pneumonia and who were unwilling to participate.
2.4. Statistical Analysis
The study employed observational and perspectives methods for data collection and outcome observations, respectively. Microsoft Excel software was utilized for the statistical analysis of collected data and results were presented in percentage format.
3. RESULTS AND DISCUSSION
The current study offered valuable insights into the management of recurrent pneumonia in paediatric populations by analysing prescribed medications, identifying underlying causes, and evaluating the use of OTC medications and nebulizers as adjunct therapies. The findings are based on a comprehensive review of over 420 recurrent pneumonia paediatric cases over a one-year period, providing a robust dataset for analysis.
The gender distribution in this study revealed a slight predominance of female children (54%) as compared to male children (46%) as shown in table 1. This distribution is consistent with the existing literature that often reports a higher incidence of respiratory infections among female children. Understanding this distribution is crucial for tailoring prevention and intervention strategies appropriately
Table 1.Gender Distribution of Paediatric Patients with Recurrent Pneumonia
| Total number of patients | 420 |
| Total number of male patients | 194 |
| Total number of female patients | 226 |
| Percentage of male patients | 46.1% |
| Percentage of female patients | 53.8% |
The average age calculated for both male and female patients was 4.5 years. The analysis of prescribed medications highlighted the common use of antibiotics and bronchodilators to manage pneumonia in children. Antibiotics are the cornerstone of bacterial pneumonia treatment, while bronchodilators are frequently used to alleviate respiratory symptoms [15]. Data revealed that ceftriaxone is the first-choice drug used for the management of pneumonia followed by vancomycin and ampicillin in both cases of previous and current medications. The previous medications prescribed for patients contained ibuprofen and paracetamol most of the time. On subsequent visits (recurrent) as indicated in Figure 2, dexamethasone and hydrocortisone were prescribed. The study’s data underlined the necessity of antibiotics for bacterial infections, however, also raised considerations about antibiotic stewardship to prevent resistance. The medications used previously and the current cases of pneumonia are listed in Figure 1 and 2.
It is essential to recognize the shift in treatment strategies over time, driven by factors, such as antibiotic resistance, efficacy, and safety concerns based on the general trends in pneumonia treatment.
Figure 1 explains that the pneumonia treatments often relied on narrow-spectrum antibiotics, such as penicillin and cephalosporins, that is, ampicillin and ceftriaxone. These medications were effective against specific pathogens, however, may now have reduced efficacy due to increasing antibiotic resistance. Penicillins and cephalosporins were commonly used in outpatient settings for the treatment of mild to moderate pneumonia cases. However, their overuse led to the rise of resistant strains, reducing their current effectiveness [16]. These are followed by vancomycin that is specific for MRSA (Methicillin-resistant Staphylococcus aureus) and must not be used unless indicated. Whereas, macrolides like azithromycin are frequently used for atypical pneumonia caused by organisms, such as Mycoplasma pneumoniae and Chlamydia pneumoniae [17]. No fluoroquinolone has been prescribed that is the first line for pneumonia. The rest of medications prescribed are for adjunct therapy. Aminophylline, meropenem, salbutamol, calpol, and clafron were used in varied numbers, as indicated in Figure 1.
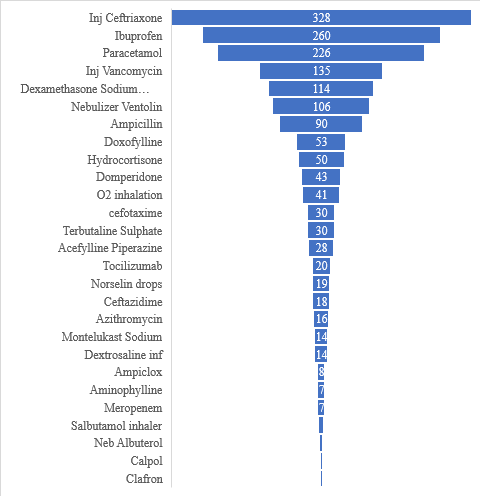
Figure 1.Frequency of Previous Medications used to Treat Pneumonia
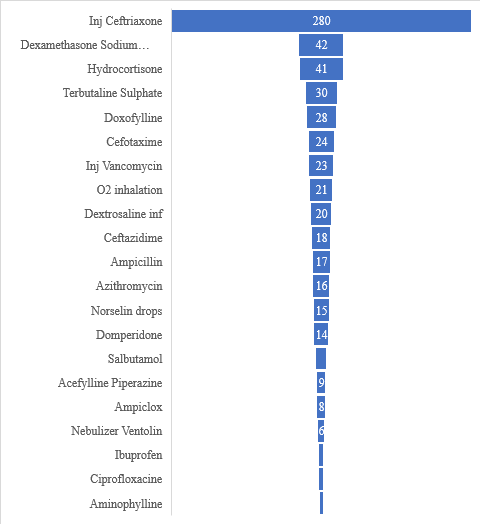
Figure 2.Frequency of Current Medications used to Treat Pneumonia
Figure 2 explains that there is not much change in the prescribing trends of antibiotics for the treatment of pneumonia. There is a slight decrease in the use of ceftriaxone, however, still it is the most prescribed antibiotic. Although, there was no prescription of vancomycin which shows slight improvement in the prescribing trend [18]. Apart from that, no fluoroquinolone was prescribed which is the first line of medication for pneumonia. Total 8 drugs were prescribed from EDL, while 20 were not prescribed from EDL.
The identification of underlying causes is critical to prevent recurrent pneumonia. The expert panel as well as physicians and pharmacists analysed the causes of recurrent pneumonia. Based on the clinical features and the results of investigations, underlying illness could be identified in children. This study identified immunodeficiency (20% of total cases), aspiration (30% of total cases), asthma (20.5%), recurrent pulmonary oedema (5%), drug toxicity (1%), structural abnormalities (9% of total cases), and granulomatous disease as significant factors. Immunodeficiency may lead towards increased susceptibility to infections, while aspiration and structural abnormalities could contribute to recurrent respiratory issues. Addressing these underlying causes through targeted interventions, such as immunoglobulin replacement therapy for immunodeficient patients or surgical correction of structural anomalies, is essential for reducing recurrence rates [19]. According to reports, 7.7% to 9% of children with community-acquired pneumonia experience at least two episodes of pneumonia in a single year or three episodes overall with intracortical radiographic clearance of density [20].
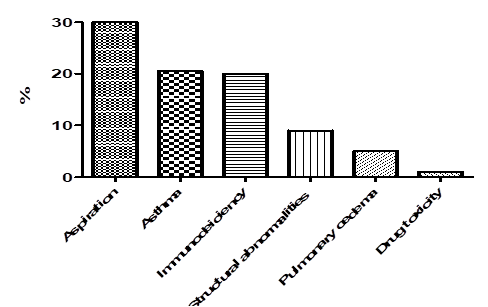
Figure 3.Percentage of Underlying Causes of Recurrent Pneumonia in Children
OTC medications are commonly used as adjuncts to antibiotics in order to manage symptoms, such as cough in children with acute pneumonia [21]. The current study found a notable percentage of cases involving OTC medications, reflecting their widespread use in symptomatic relief. Paracetamol (226) and ibuprofen (137) were the most used OTC drugs. However, the efficacy and safety of these medications need careful consideration, especially in young children. Healthcare providers should ensure that parents and caregivers are well-informed about appropriate OTC medication use and potential side effects [22]. Table 2 shows the OTC drugs used to manage pneumonia.
Table 1.Frequency of OTC Drugs used to manage Pneumonia
| Groups | Dose (Quantity/kg/day) |
|---|---|
| Paracetamol | 226 |
| Ibuprofen | 137 |
| Acefyl | 40 |
| Acefylline Piperazine | 28 |
| Muconyl | 20 |
| Broxol-DM | 16 |
| Provas | 16 |
| Mucinex | 13 |
| Ferosoft | 9 |
| Coldrex | 9 |
| Actified-DM | 5 |
| Cap Vit A | 5 |
| Chlorphinramine | 1 |
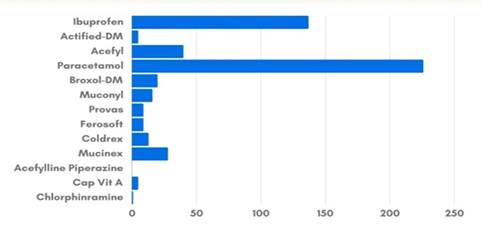
Figure 4.Frequency of OTC Drugs used to manage Pneumonia
The current study also examined the use of nebulizers, which are often prescribed to deliver bronchodilators and other medications directly to the lungs. The percentage of patients using nebulizers indicates their role in managing acute respiratory distress. Nebulizer therapy may be particularly beneficial for children with severe symptoms or those struggling with inhaler techniques. However, proper education on nebulizer uses and maintenance is crucial to maximize therapeutic benefits and minimize risks, such as infections [23].

Figure 5.Figure shows the Percentages of Nebulizer Albuterol and Ventolin used.
The findings have several implications for clinical practice. Firstly, the study emphasized the importance of a comprehensive diagnostic approach to identify and address the underlying causes of recurrent pneumonia. Secondly, it highlighted the need for judicious use of antibiotics and the potential role of adjunct therapies including OTC medications and nebulizers. Lastly, the study underscored the importance of educating caregivers pertaining to the appropriate use of these therapies in order to ensure safety and efficacy [24].
With the rise of antibiotic resistance, treatment has shifted towards broad-spectrum antibiotics. Fluoroquinolones (for instance, levofloxacin, moxifloxacin), newer macrolides (e.g., azithromycin), and third-generation cephalosporins (e.g., ceftriaxone, cefotaxime) are now used more frequently.
Newer medications aim to cover a broader range of pathogens including drug-resistant strains of Streptococcus pneumoniae and Haemophilus influenza. Carbapenems (for instance, meropenem) and piperacillin-tazobactam are now reserved for severe or hospital-acquired pneumonia (HAP) where multidrug-resistant organisms are suspected [25].
Previous medications were more focused on narrow-spectrum antibiotics, which are now less effective due to resistance. Current medications are broad-spectrum, targeting resistant and atypical pathogens as well as reflecting changes in microbial patterns and treatment guidelines. The shift is towards medications that cover multidrug-resistant organisms, especially in hospital settings or severe pneumonia cases.
3.1. Conclusion
The current prospective observational study provided significant insights into the management of recurrent pneumonia in children by analysing prescribed medications, identifying underlying causes, and evaluating the use of OTC medications and nebulizers. The key findings included a balanced gender distribution with a slight female predominance. The study underscored the necessity of a comprehensive diagnostic approach to address these underlying causes effectively. Furthermore, it also highlighted the widespread use of OTC medications and nebulizers as adjunct therapies, emphasizing the need for careful consideration of their efficacy and safety in paediatric patients. In conclusion, healthcare providers may considerably improve clinical outcomes and lower the recurrence of pneumonia in children by addressing underlying causes and making the most of prescribed and adjunct therapies. This would lessen the overall burden of pneumonia on paediatric populations.
3.2. Future Research Implications
Longitudinal studies should be focused in future to track long-term outcomes of children with recurrent pneumonia, considering both pharmacological and non-pharmacological interventions. Additionally, exploring the impact of educational interventions for caregivers on the management of paediatric pneumonia could provide further insights into improving care and reducing recurrence rates.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
Data will be provided by corresponding author on reasonable request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Yadav KK, Awasthi S. Childhood pneumonia: what’s unchanged, and what’s new?. Ind J Pediatr. 2023;90(7):693–699. https://doi.org/10.1007/s12098-023-04628-3
- Ablakimova N, Smagulova GA, Rachina S, et al. Bibliometric analysis of global research output on antimicrobial resistance among pneumonia pathogens (2013–2023). Antibiotics. 2023;12(9):e1411. https://doi.org/10.3390/antibiotics12091411
- Choo ELW, Janhavi A, Koo JR, Yim SH, Dickens BL, Lim JT. Association between ambient air pollutants and upper respiratory tract infection and pneumonia disease burden in Thailand from 2000 to 2022: a high frequency ecological analysis. BMC Infect Dis. 2023;23(1):e379. https://doi.org/10.1186/s12879-023-08185-0
- Dinka IR, Seyoum D, Debelo S, et al. Time to recovery and its predictors among under-five children admitted with severe pneumonia in East Wallaga Zone public hospitals, western Ethiopia, 2023; a retrospective cohort study. BMC Pediatr. 2024;24(1):e459. https://doi.org/10.1186/s12887-024-04937-2
- Akhtamovna KN. Modern diagnostics and treatment methods of pneumonia in children. J Healthc Life Sci Res. 2023;2(12):155–160.
- Postma DF, Van Werkhoven CH, Van Elden LJ, et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N Engl J Med. 2015;372(14):1312–1323. https://doi.org/10.1056/NEJMoa1406330
- Sidabutar E, Bustan N, Birawida AB. Analysis of risk factor for pneumonia in children less than five years in Makassar. J Educ Health Promot. 2024;13(1):e16. https://doi.org/10.4103/jehp.jehp_727_23
- Ruuskanen O, Järvinen A. Editorial commentary: what is the real role of respiratory viruses in severe community-acquired pneumonia?. Clin Infect Dis. 2014;59(1):71–73. https://doi.org/10.1093/cid/ciu242
- Cotter JM, Hall M, Neuman MI, et al. Antibiotic route and outcomes for children hospitalized with pneumonia. J Hosp Med. 2024;19(8):693–701. https://doi.org/10.1002/jhm.13382
- Mei M, Dai D, Guo Z, et al. Underlying causes and outcomes of recurrent pneumonia in hospitalized children. Pediatr Pulmonol. 2023;58(6):1674–1682. https://doi.org/10.1002/ppul.26374
- Restrepo MI, Sibila O, Anzueto A. Pneumonia in patients with chronic obstructive pulmonary disease. Tuberc Respir Dis. 2018;81(3):187–197. https://doi.org/10.4046/trd.2018.0030
- Gupta S, Pattanaik D, Krishnaswamy G. Common variable immune deficiency and associated complications. Chest. 2019;156(3):579–593. https://doi.org/10.1016/j.chest.2019.05.009
- Tsegaw H, Yimam M, Nureye D, Woldeselassie W, Hambisa S. Predictors of treatment outcomes among pediatric patients hospitalized with pneumonia in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Adv Pharm Pharm Sci. 2021;2021(1):e6690622. https://doi.org/10.1155/2021/6690622
- Mishore KM, Girma Y, Tola A, Mekuria AN, Ayele Y. Evaluation of medication use pattern among patients presenting to the emergency department of Hiwot Fana Specialized University Hospital, using WHO prescribing indicators. Front Pharmacol. 2020;11:e509. https://doi.org/10.3389/fphar.2020.00509
- Zhang Zs, Li H, Hu Y, et al. The efficacy and safety of inhaled antibiotics for pneumonia: a systematic review and meta-analysis. Pulm Pharmacol Ther. 2024;86:e102315. https://doi.org/10.1016/j.pupt.2024.102315
- Heffelfinger JD, Dowell SF, Jorgensen JH, et al. Management of community-acquired pneumonia in the era of pneumococcal resistance: a report from the Drug-Resistant Streptococcus pneumoniae Therapeutic Working Group. Arch Intern Med. 2000;160(10):1399–1408. https://doi.org/10.1001/archinte.160.10.1399
- Vigo E. Community-acquired infections: focus on unusual epidemics and update on S. pneumonia. Clin Microbiol Infect. 2004;10(3):87–178.
- Sileshi A, Tenna A, Feyissa M, Shibeshi W. Evaluation of ceftriaxone utilization in medical and emergency wards of Tikur Anbessa Specialized Hospital: a prospective cross-sectional study. BMC Pharmacol Toxicol. 2016;17:1–10. https://doi.org/10.1186/s40360-016-0057-x
- Quinti I, Soresina A, Guerra A, et al. Effectiveness of immunoglobulin replacement therapy on clinical outcome in patients with primary antibody deficiencies: results from a multicenter prospective cohort study. J Clin Immunol. 2011;31:315–322. https://doi.org/10.1007/s10875-011-9511-0
- Montella S, Santamaria F. Recurrent pneumonia in children: a reasoned diagnostic approach and a single centre experience. Int J Mol Sci. 2017;18(2):e296. https://doi.org/10.3390/ijms18020296
- Clark G, Fitzgerald DA, Rubin BK. Cough medicines for children-time for a reality check. Paediatr Respir Rev. 2023;48:30–38. https://doi.org/10.1016/j.prrv.2023.08.003
- Berbakov ME, Hoffins EL, Stone JA, et al. Adapting a community pharmacy intervention to improve medication safety. J Am Pharm Assoc. 2024;64(1):159–168. https://doi.org/10.1016/j.japh.2023.11.009
- Shen K, Hong J, El Beleidy A, et al. International expert opinion on the use of nebulization for pediatric asthma therapy during the COVID-19 pandemic. J Thorac Dis. 2021;13(7):e3934. https://doi.org/10.21037/jtd-21-841
- Thi TVL, Pham EC, Dang-Nguyen DT. Evaluation of children's antibiotics use for outpatient pneumonia treatment in Vietnam. Braz J Infect Dis. 2024;28(4):e103839. https://doi.org/10.1016/j.bjid.2024.103839
- Raj K, Attavar PC. Multidrug resistance in microorganisms causing ventilator-associated pneumonia: a literature review. Int J Res Publ Rev. 2024;5(1):15965–15974.