Kidney Stones: Pathophysiology, Cutting-Edge Treatments, and Emerging Concerns
Faiza Saifullah*, and Muhammad Asad Saeed
University of Central Punjab, Lahore, Pakistan
ABSTRACT
Kidney stone disease (KSD) is a frequently observed clinical condition globally. It poses multiple diagnostic and therapeutic challenges especially in the case of asymptomatic stones when using standard ultrasonic or X-ray procedures. While CT scan options are available for diagnosis, they raise concerns due to excessive radiation exposure. Etiology of KSD is vast and covers disparate types of stones out of which calcium oxalate stones are the most prevalent ones. KSD is influenced by enormous factors ranging from age, gender and obesity to serious metabolic and genetic disorders. Different treatment protocols are available including medications, lithotripsy, ureteroscopy, PCNL and open surgery. Their pros and cons are discussed comprehensively throughout the review. Surgery is only opted for cases when the stone is either extremely large or highly complicated. KSD is a painful condition and most of its treatment options are costly, resulting in a significant financial burden. Despite the availability of advanced treatment protocols, the cases of KSD continue to rise, which is concerning. This suggests that the changing climate and environmental factors which are significantly raising global temperature along with dehydration, may play a role in increasing the prevalence of the disease. The aim of this review is to provide a comprehensive overview of kidney stone disease, providing in-depth insights into stone types and their corresponding management strategies. Furthermore, this review also emphasizes the importance of lifestyle and dietary modifications, identifies constraints observed in the literature survey, and discusses the challenges facing healthcare providers, while also suggesting possible future research directions for emerging studies.
GRAPHICAL ABSTRACT
1. Introduction
A kidney stone is a solid mass that forms inside the kidneys, that not only impairs the quality of life, but also increases the risk of kidney failure and other renal complications [1].
1.1. Prevalence
Although various factors such as gender and climatic influence play a pivotal role in its occurrence, an increased incidence of kidney stones is observed in individuals over 30 years of age irrespective of gender [2].
1.2. Economic Impact
This accounts for a high financial burden on medical facilities for its treatment protocols [3]. According to a recent report, almost USD 5.3 billion was spent on its treatment in 2014, making it the most expensive of all renal ailments [4].
Kidney stones disease is a common condition worldwide and it is not only painful but also a major cause of chronic kidney disease or end-stage kidney disease [5–8]. Its global prevalence is almost 13% [2]. Even after complete recovery through appropriate medication, patients still suffer from the same consequence approximately after 5 years of initial treatment [9]. This represents a successive healthcare and financial burden [10].
1.3. Treatment Guidelines
Multiple guidelines are available for its diagnosis, treatment and follow-up procedures, most significant of which are the American Urology Association (AUA) and European Association of Urology (EAU) guidelines. The AUA guidelines use an alphabetical approach for grading [11], whereas EAU relies on words like strong and weak to emphasize the strength of recommendations [12].
Although guidelines serve as a very important tool for providing valuable information about a particular disease, they still do not guarantee desired outcomes. The major reason for this is the lack of timely upgradation of such guidelines [13].
1.4. Risk Factors
Kidney stones are produced by mineral crystallization which on further adherence forms a rigid mass. These stones vary widely in terms of size and location. They can be located in the ureter, kidney or bladder etc. Even after treatment, recurrence is tremendously observed in patients and assorted approaches are used for its avoidance. Dehydration is recognized as the major cause of stones development [14].
Some studies suggest that climate significantly influences the occurrence of kidney stones. Higher temperature favors the development of renal stones. In urban areas, temperature is constantly rising due to global warming and other effects, indicating that the prevalence of kidney stones will keep on increasing day by day if the situation persists [15].
A few literature outcomes also revealed an exceptional relationship between kidney stones and alcohol consumption. Heavy alcohol consumption was found to be reducing the risk of kidney stone development, somehow advanced studies are required in this area to identify the major contributing factor for this sequel [16].
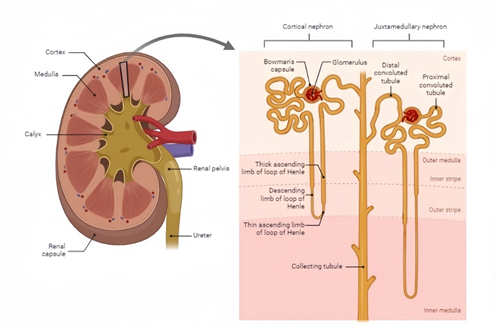
1.5. Anatomy Overview
Kidneys are bean-shaped organs and are estimated 11–14 cm in length, 6 cm in width and almost 4 cm in thickness. The left renal vein is thrice longer than the right one. Unlike the right one, the left renal vein before joining directly to the inferior vena cava receives several tributaries [17].
The nephron comprises the renal glomerulus, Bowman’s capsule, ascending and descending loop of Henle, distal convoluted tubule and collecting duct. The renal cortex is an outer layer, and it consists of a large number of nephrons. Nephron is further subdivided into two parts: the renal corpuscle and the renal tubule. The renal corpuscle constitutes the glomerulus and Bowman’s capsule, and the rest of the parts are included in the renal tubular portion.
The tips of renal pyramids are known as renal papillae, which directly project into the renal pelvis. It is a cavity responsible for collecting urine produced by nephrons. The renal pelvis further channels into the ureter which transfers the formed urine to the bladder where it is temporarily stored before excretion.
The deep anatomy of the kidney, as illustrated in Figure 1, also shows that the kidneys contain specialized cells that secrete essential hormones, helping to maintain hormonal balance.
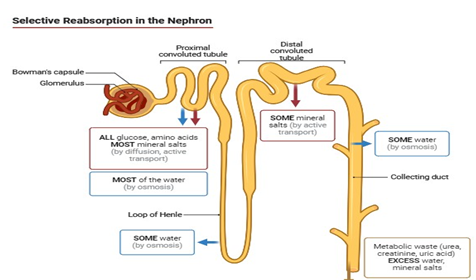
2. GENERAL PHYSIOLOGY
The kidneys are generally involved in osmoregulation and typically require 20-25% of cardiac output to function effectively and to maintain homeostasis [18]. Their most important function is filtering blood and producing urine. Water reabsorption is regulated by hormonal responses of aldosterone and antidiuretic hormone (ADH). The kidneys also help maintain acid-base balance by secreting drugs or ions, such as potassium and hydrogen into the tubular fluid from the blood. In this way, urine is formed and collected in the renal pelvis which is then transferred to the bladder via the ureters and is then expelled from the body through the urethra. The kidneys also play a significant role in regulating hormonal balance as in hypoxic conditions. Erythropoietin produced by kidneys in response to hypoxia facilitates red blood cell production by the stimulation of bone marrow. However, in response to low blood pressure, Renin is released which in turn activates RAAS, leading to elevated blood pressure through sodium reabsorption. RAAS system activates in response to low blood pressure to convert angiotensin 1 to angiotensin 2, it also releases aldosterone to maintain blood pressure homeostasis. Kidneys also play a crucial role in activating vitamin D, producing calcitriol which assists in regulating calcium and phosphate levels owing to better bone health. General physiology is depicted in Figure 2.
3. KIDNEY STONES
3.1. Pathophysiology
Kidney stones are composed of amalgamated organic and inorganic crystals with proteins. Lithogenesis and crystallization can occur with many solutes in the urine but the most recurrent of all kidney stones are calcareous stones covering almost 80% of kidney stone cases [19–23].The pathophysiology of kidney stones is highly dependent on the type of stone, but renal water conservation is observed in almost all types of stones. In the case of calcium stones, elevated gut absorption and bone resorption are noticed, followed by leakage of calcium ions, renal leak, and bone loss induced by protein, hypocitraturia, aggravated luminal oxalate delivery, and urine excretion [24–26].In case of uric acid stones, urate titration to poorly soluble uric acid is observed [27]. Basic amino acid leakage occurs in cysteine stones, whereas in infectious stones, ammonium and bicarbonate production is enhanced from urea. The most prevalent pathophysiological factor for calcium stones is hypercalciuria [28]. Hyperoxaluria raises calcium oxalate urinary saturation but is less commonly observed than hypercalciuria [29, 30].
3.2. Causes
The literature indicates a strong connection between nutrient consumption, lifestyle factors, and the occurrence of kidney stones. High intake of carbohydrates and copper has been identified as a primary contributor to kidney stone formation [31]. Dehydration is also a well-documented cause of kidney stones.
Deficiency of Adenine phosphoribosyl transferase (APRT), Dent disease, nephrocalcinosis, hypomagnesemia, cystinuria, hypercalcinuria, and hyperoxaluria are rare but important precursors of kidney stone development [32]. This shows that genetic factors play a primary role in the development of kidney stones [33].
Some studies have also demonstrated a strong association between exposure to volatile organic compounds, such as styrene, propylene oxide, and the incidence of kidney stones. This association was quite robust among females and obese individuals [34].
Stone formation occurs only by the supersaturation of urine with some of the most common salts like calcium [35–37].
Dent’s disease is found as one of the major concerns in the development of kidney stones. It is a disease characterized by the functional defect in the proximal convoluted tubule, which then causes low-molecular-weight proteinuria, nephrolithiasis, and hypercalcinuria. It is an X-linked inherited disorder, which predominantly affects males [38]. In this disease, protein reabsorption is impaired, and its true prevalence is still unknown, which may account for the lack of complete patient history especially in affected areas of Pakistan [39]. This disease may occasionally require complete renal replacement in severe cases [40].There is no treatment available for this disease so symptomatic approaches are pursued for temporary relief of the condition. Usually, thiazides are often prescribed for this purpose as it helps in reducing calcium levels [38]. Lifestyle modifications and genetic counseling of such patients are mandatory [41, 42].
Hyperoxaluria is the main cause of the emergence of kidney stones [43]. It is a genetic condition and is often associated with the excessive production of oxalate by the liver, referred to as primary hyperoxaluria [44, 45]. In some cases, it may arise from non-genetic lifestyle factors, for instance a high intake of oxalate through diet or a reduction in the metabolic rate of oxalate. In this case, it is termed secondary hyperoxaluria [46].
Hyperoxaluria can lead to kidney injury and may also cause oxalate crystals to deposit in other organs due to a declining glomerular filtration rate. Primary hyperoxaluria is diagnosed in the advanced stages of chronic kidney disease in almost 50% of patients. After kidney transplantation, only 10% of patients are diagnosed with kidney stones after reoccurrence [47].
Out of all possible inducers of kidney stones, uric acid accounts for 5–40% of cases, with idiopathic hyperuricosuria being the primary reason. This condition is often associated with obesity, diabetes mellitus, or other metabolic disorders [48]. Hyperuricosuria is not only associated with kidney stones but also with deteriorating kidneys on various levels. It causes impaired autoregulation, microvascular damage, inflammation, and renal vasoconstriction [49]. Early identification is of prime importance for the prevention of renal graft damage [50].
Hypocitraturia is among the 30% of all potential kidney stone formers [51]. Hypocitraturia is prominent after renal transplantation and causes post-transplant nephrolithiasis [52]. Excessive diarrhea can decrease citrate absorption in the intestine [53]. Conditions like intestinal malabsorption and diarrhea reduce urinary magnesium levels while increasing overall citrate absorption, both of which are highly linked with the development of nephrolithiasis [54].
Kidney transplantation itself is a contributing factor to kidney stone formation, affecting approximately 1–2% of transplant recipients. Usually, kidney transplant patients are asymptomatic for kidney stones [55]. The basic precursors of kidney stone development are displayed in Figure 3.
3.3. Diagnosis
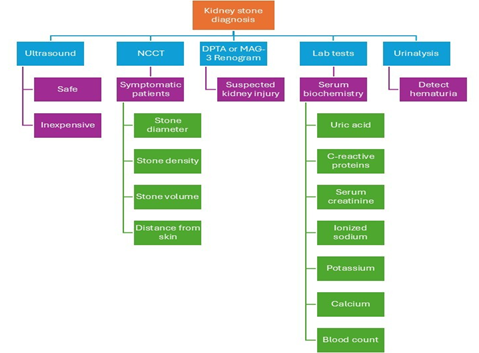
There are multiple diagnostic procedures available for kidney stones, as mentioned in Figure 4 [56–58]. According to EAU guidelines, the most valuable approach for the investigation of renal stones in asymptomatic patients is the use of ultrasound, as it is not only inexpensive but also safe and effective in the diagnosis of calculi. Non-contrast-enhanced computed tomography (NCCT) is prudent as an investigational tool for symptomatic patients. It can easily depict stone diameter, density, volume, and the distance of the stone from the skin accurately [59].According to the AUA guidelines, if a significant kidney injury is suspected, techniques such as a diethylene-triamine-penta-acetate (DTPA) or mercaptoacetyltriglycine (MAG-3) renogram — which are the major functional imaging modalities — can be used to guide treatment decisions.
Other than imaging, numerous laboratory screening tests are also suggested as diagnostic parameters, including serum biochemistry and coagulation tests. According to EAU guidelines, uric acid, C-reactive proteins, serum creatinine, ionized sodium, potassium, calcium, and blood count should also be evaluated [60].
Ultrasound is the most common diagnostic tool for kidney stones. After that, stones are examined by X-ray crystallography. Infrared may also serve as a potential analytical tool in the future. Urinalysis is performed to detect the presence of blood, as hematuria eventually confirms the diagnosis [61–64].
Analyzing the basic chemistry and composition of kidney stones can provide valuable insights into the disease’s etiology and help identify possible underlying illness. This can be achieved by using machine learning algorithms [65–67].
Machine learning algorithms are useful in classifying chronic kidney disease using deep neural networks [68]. Examples include support vector machine, adaptive boost, multilayer perceptron, random forest classifier, and decision tree [57]. These algorithms also help in predicting stone recurrence by analyzing urine data within a 24-hour timeframe [69]. Machine learning also predicts CKD state in an effective manner [70].Deep learning approaches are also utilized along with machine learning for the classification of CKD. Convolutional neural networks (CNNs) are used to categorize kidneys according to CT scan images such as tumor, cyst, normal, or stone. These approaches also facilitate the prediction of possible renal failure.
3.4. Types of Kidney Stones
Table 1.Summary of Types of Kidney Stones| Type of kidney stone | Causes | Treatment | Symptoms |
|---|---|---|---|
| Calcium oxalate stones |
• Metabolic disorders • Idiopathic |
• Thiazide diuretics • Potassium citrate • Diet low in calcium and sodium • If increase in uric acid is observed allopurinol is recommended |
• Renal Colic • Hematuria • Nausea • Vomiting • Frequent Urination |
| Uric acid and urate stones |
• Diabetes • Ageing • Hypertension |
• Urine alkalinization with potassium citrate • Allopurinol |
• Painful urination • Hematuria • Foul-smelling urine |
| Cysteine stones |
• Cystinuria • Low urinary pH • Dehydration • UTIs |
• Potassium citrate • Urine alkalinization • High fluid intake • Protein and sodium intake should be reduced • Thiol containing medications (Captopril) |
• Persistent pain in lower abdomen or back • Frequent and painful urination • Hematuria |
| Calcium phosphate stones |
• Hyperthyroidism • Renal acidosis • UTIs |
• Reduce sodium intake • Increase calcium intake • Thiazide diuretics • Phosphorous binding agents |
• Hematuria • Nausea and vomiting |
| Struvite stones |
• Pre-existing infections • Cystinuria |
• Surgical treatment • Anti-microbials |
• Painful urination • Recurrent Urinary Tract infections • Fever and chills • Severe back pain |
| Infectious stones |
• Urea-splitting microorganisms |
• Antimicrobials • Urease inhibitors |
• Recurrent Urinary tract infections • Painful urination • Nausea and vomiting • Fever and chills |
3.5. Symptoms
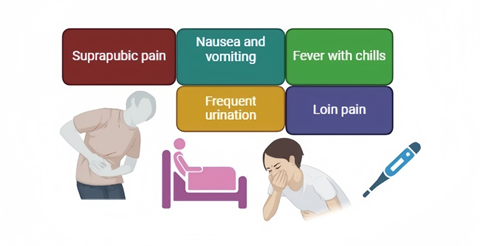
Symptoms of kidney stones can vary from person to person, as elucidated in Figure 5. Common symptoms include high fever and vomiting, frequent urination, suprapubic pain, and terminal hematuria. Patients may also experience intense loin pain, or they may be completely asymptomatic. Ordinary symptoms include frequent urination and severe back pain, this pain is usually described by patients as colicky, but fluctuates in intensity. In severe cases, urine may accumulate with blood with pain. If an infection is present, a patient may encounter fever with chills. Rare symptoms include urine with a bad smell and cloudy appearance, vague pain or severe stomach pain that doesn’t easily go away, burning sensation during urination, sharp pain below the ribs, hematuria, dizziness, and frequent urinary tract infections.
3.6. Treatment
Immediate pain-relieving medications are recommended as renal colic pain is almost unbearable. NSAIDs are prescribed although opioids can be suggested but NSAIDs are a better option as they proffer fewer side effects. However, NSAIDs are generally not advised in kidney transplant patients due to their ability to induce nephrotoxicity [62]. Treatment pathway is described in Figure 6.
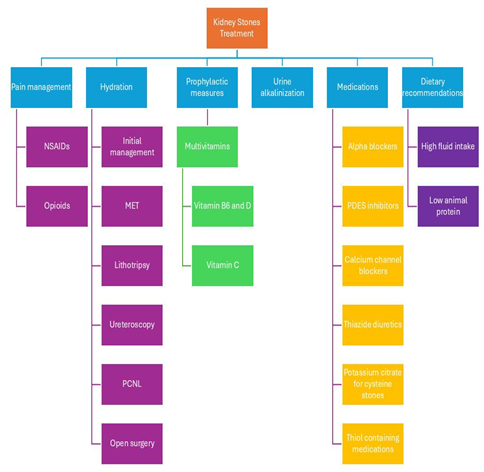
The first line approach for the initial management of kidney stones involves hydration and pain management using pain-killers. The second line approach includes medication expulsive therapy, as discussed in the successive sections, followed by Lithotripsy, Ureteroscopy, PCNL and ultimately open surgery if no recovery is observed.
Intake of multivitamins is considered an effective prophylactic measure for preventing kidney stones. The coadministration of vitamin B6 and vitamin D has been shown to reduce the prevalence of kidney stones. The use of vitamin C is first found to be effective in avoiding kidney stones but its prolonged consumption aggravates stone formation [71].
Multiple drugs of various pharmacological classes offer significant potential. Such drugs may include α-blockers which are highly recommended for stones having size >5 mm according to EAU. In contrast, AUA suggests α-blockers for all stones up to 10 mm in size. Furthermore, phosphodiesterase type 5 (PDE5) inhibitors and calcium channel blockers are also recommended. α-blockers are highly advised in kidney transplant patients [72]. Thiazide diuretics play a positive role in treating kidney stones due to their vasodilating property, but they offer some undesirable metabolic side effects like compromised glucose tolerance [73].
Urine alkalinization is another key approach implemented [74]. This approach is characterized by using sodium bicarbonate and alkaline citrate for making urine alkaline which helps in dissolving uric acid stones. Although this treatment of oral chemolysis has been in practice for years, no clinical trials have been conducted to validate it. Potassium citrate can also be used for cysteine stones. Urine pH should be regularly monitored for those patients who are receiving this therapy which will help in dose adjustments. Uric acid stones are highly linked with other diseases like diabetes, hypertension, aging etc. Chemolysis can be performed using potassium citrate for the dissolution of kidney stones. This treatment was not only found successful in treating kidney stones, but it also proved to be effective in avoiding reoccurrence [75]. Xanthine oxidase inhibitors are commonly used to prevent uric acid stone formation [76].
In the case of cysteine stones, high fluid intake is good for resolving the issue. Thiol-containing medications are good alternatives especially for those patients who cannot rely on high fluid intake due to multiple medical reasons. Captopril is used for this purpose, but its efficacy is still unknown. During this treatment, a low animal-protein diet is suggested [77].
Lithotripsy is another option with fewer complications as compared to PCNL and ureteroscopy [78, 79]. The efficacy of this procedure depends on the composition, size, and location of the stone. To prevent unnecessary deflection of shock waves, ultrasound gels are used. A suitable analgesic should be utilized as this method is accompanied by severe pain-induced movements. If stones are highly infected, antibiotics are also recommended. According to the majority of guidelines, stent placement is not usually recommended. Despite being effective, this method cannot be used in pregnant patients and in patients with uncontrolled UTIs, skeletal malformations, bleeding disorders, arterial aneurysm close to the stone, anatomical obstructions or patients who are highly obese. Lithotripsy is a non-invasive treatment with fewer complications in comparison to other methods [80].
Ureteroscopy is complicated but has better outcomes as compared to lithotripsy [81]. Stent placement is not recommended in this procedure either because of the complications associated with it or its expensive nature. AUA recommends it in extreme cases with high evidence; otherwise, it is usually discouraged. If stent placement is necessary, then α-blockers should be prescribed to avoid discomfort associated with a stent. The holmium: yttrium–aluminum–garnet (Ho:YAG) laser is suggested to be used in ureteroscopy by EAU. Prophylactic use of antibiotics should also be ensured prior to operation. Ureteroscopy cannot be used for ureteral stones. It is highly recommended in cases when antithrombotic therapy cannot be discontinued. It is recommended in pregnant women or obese patients especially among those having bleeding diathesis [82]. An endoscopic procedure is preferred if kidney stones are smaller in size in the transplanted kidney [83]. Urinary tract infections are the major complications that occur with this technique [74].
Percutaneous Nephrolithotomy (PCNL) is recommended as a first-line approach for renal calculi [84]. Before the procedure, a CT scan or other imaging approach should be utilized to get a better picture of the condition. Flexible nephroscopy should be used for the removal of unnecessary fragments from areas where a rigid nephroscope has no access. Electrolyte derangement should be avoided by the use of normal saline. Cultures should be taken directly from the pelvis to avoid sepsis [85, 86]. PCNL is not suggested for pregnant patients, patients with malignant renal tumors, patients using anti-coagulant therapy, or those with untreated UTIs. Percutaneous therapy has a risk for the development of hemorrhage or sepsis [87]. The principle of PCNL is the use of endoscopic instruments for the extraction, crushing, and pulverization of kidney stones. The main advantage that this technique offers is the reduction in the rate of lumbotomies, which was the major reason for some serious complications in young patients [78, 88, 89]. Thus, PCNL plays an important role in the management and treatment of kidney stones [90]. PCNL is highly recommended for stones having size >2 cm [91–93]. Horseshoe kidneys are at risk of developing urolithiasis, and PCNL is the suggested treatment to address this issue as non-invasive approaches are usually desired in such cases [94, 95].
If a patient has stones and other anatomical defects that require reconstruction, then open surgery and laparoscopy are highly effective. This approach is reserved only for complex cases or when other treatments fail to give effective results. It has higher SFR in comparison to other techniques [96, 97]. Treatment and management approaches are exemplified in Table 2.
Table 2.Treatment Options for Kidney Stone Disease| Treatment options | Indication | Contraindication | Justification of Contraindication |
|---|---|---|---|
| NSAIDs and Opioids |
Symptomatic relief | NSAIDs are not recommended for kidney transplant patients due to their potential for nephrotoxicity |
NSAIDs inhibit cyclooxygenase (COX) enzymes, which are required for prostaglandin production for regulating blood flow to the kidneys as a result patient may experience a decline in graft function and impaired renal blood flow. |
| Notreatment just increasd fluid intake |
For stones <4mm | It is not suggested for large, extremely complex stones |
Larger and complex stones may be life-threatening, so they require immediate treatment. |
| α-blockers | For stones >5mm For kidney transplant patients | It is not proposed for patients with exceptionally low blood pressure | Alpha- blockers relaxes the blood vessels which may lower the blood pressure to alarming level, leading to orthostatic hypertension. |
| Phosphodiesterase type-5 inhibitors or calcium channel blockers |
<10mm | Not appropriate for patients on nitrates therapy | Combination of these two will drop the blood pressure level to dangerous level |
| Thiazide diuretics | Hypercalcinuria | May cause glucose tolerance | Thiazide diuretics may impair insulin secretion which could be problematic in diabetic patients |
| Urine alkalinization | Recommended for urate or cysteine stones | It is not encouraged for calcium phosphate stones |
Calcium phosphate stones require alkaline environment to grow that is why urine alkalinization may aggravate calcium phosphate stones |
| Lithotripsy | Suggested to most of the kidney stones | It is not suitable for highly infectious stones |
In infectious stones lithotripsy may cause bacteria to enter blood stream or urinary tract, which will result in extreme sepsis |
| Ureteroscopy | Good for patients using anti-thrombotic therapy Suggested for pregnant or obese patientsPatients with bleeding diathesis | It is not advised for ureteral stones | In very complex cases of ureteral stones, ureteroscopy may cause sepsis |
| PCNL | 1st line approach for renal calculi For stones >2cmFor horseshoe kidneys |
It is not suggested in pregnancy It is not recommended for patients with malignant renal tumors It is not appropriate for the patients using anti-coagulants or those patients with untreated UTIs | In pregnancy, PCNL is generally not recommended as it uses radiation which can be harmful for developing fetus In tumor patients, PCNL can cause tumor seeding so it is generally not recommended |
| Open surgery and Laparoscopy | Suggested for highly complex stones when other treatment options collapse | For minor and small stones | Combination of these two will drop the blood pressure level to dangerous level |
4. RECENT ADVANCES AND FUTURE CONCERNS
Although for professional medical experts’ kidney-ureter-bladder (KUB) X-ray images are relatively easy, certain poses can be difficult to classify accurately by humans, highlighting the need for AI assistance. To address this challenge, researchers have developed a transfer learning (TL) model which is VGG16 empowered. In this model, AI efficiently accesses and classifies KUB X-ray images as normal or kidney stones. This model’s accuracy was found to be 97.41%. This model, despite having high precision, was unable to ensure fairness and description of the decision-making process. To address this issue a new explainable artificial intelligence (XAI) technique was established. It is a recent technique and shows a greater potential for detection and diagnosis of kidney stones which may prove to be beneficial in for medical professionals. A new novel approach using conventional neural network has been developed for an accurate diagnosis of kidney stones. This approach is used in collaboration with computed tomography images. This approach is based on efficient optimization of conventional neural network by utilizing dwarf mongoose optimization (FDMO) algorithm which helps by providing an efficient model for kidney stones detection. This model helps in ensuring patient care by reducing physician-induced errors or uncertainties. Now with emerging AI technologies, AI chatbots are available for designing dietary plans for kidney-compromised patients. Bard AI is the best available AI chatbot for estimating oxalate concentrations in food items.
5. DISCUSSION
Kidney stone disease is a major health challenge in today’s world, and several future concerns need to be adequately addressed [1]. Since obesity greatly increases the risk of kidney stones, controlling obesity could serve as an effective preventive strategy. Modifying lifestyle and dietary habits also help prevent and manage kidney stones [14]. Although diagnostic technology and treatment options have advanced significantly in this modern era, a proper approach is needed to address preventive measures in a comprehensive manner which can be ensured by increasing public awareness regarding appropriate lifestyle modifications and dietary recommendations. Efficient research should focus on developing personalized prevention and treatment strategies for each patient by addressing genetic and metabolic issues of each patient individually. With evolving environmental factors, new stone types are emerging thus requiring a thorough research dive for evaluating their composition, prevention and treatment protocols. Future efforts should be on the development of antibiotic-resistant infections which are found as the main reason for complications. Addressing this issue requires a multifaced approach, including better education on lifestyle modifications, advancements in medical research and improved access to healthcare providers, researchers and public health officials will be effective in the management and reduction on the impact of kidney stones and overall global health. Kidney stones treatments are highly expensive so sufficient importance should be given to manage the financial concerns associated with it [4]. Additionally, the risk of chronic kidney disease due to kidney stones should also be effectively disserted. Challenges and costs associated with the emerging technologies should be handled. Moreover, research on genetic findings also present a main challenge as they are not easy to carry out. With evolving treatment practices risks for complications may arise and strategies should also be developed to ensure patient compliance.
5.1. Conclusion
Kidney stone disease is a common urological condition. Its diagnostic and treatment modalities are well-established but still, there remains significant room for research and development. Kidney stone disease due to genetic factors is the least explored area. Moreover, challenges in regard to high expenditures on its treatment protocols are also not effectively handled. AI-based algorithms are serving as promising diagnostic tools by using numerous neural networks but access to healthcare facilities is still a matter of concern. Furthermore, with climate change and evolution new types of kidney stones are also discovered which requires researchers to shift their focus to this side and ensure a promising healthy future for upcoming generations.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
All the data evaluated in this review article is available publicly in published articles and is properly cited in the reference section.
FUNDING DETAILS
No funding was received for this work.
REFERENCES
- Assad A, Raizenne BL, El Yamani MEM, et al. The impact of kidney stone disease on quality of life in high‐risk stone formers. BJU Int. 2024;133(5):570–578. https://doi.org/10.1111/bju.16294
- Sorokin I, Mamoulakis C, Miyazawa K, Rodgers A, Talati J, Lotan Y. Epidemiology of stone disease across the world. World J Urol. 2017;35:1301–1320. https://doi.org/10.1007/s00345-017-2008-6
- Devi AT, Nagaraj R, Prasad A, Lakkappa DB, Zameer F, Nagalingaswamy NPM. Nephrolithiasis: insights into biomimics, pathogenesis, and pharmacology. Clin Complement Med Pharmacol. 2023;3(2):e100077. https://doi.org/10.1016/j.ccmp.2022.100077
- Raheem OA, Khandwala YS, Sur RL, Ghani KR, Denstedt JD. Burden of urolithiasis: trends in prevalence, treatments, and costs. Eur Urol Focus. 2017;3(1):18–26. https://doi.org/10.1016/j.euf.2017.04.001
- Sigurjonsdottir VK, Runolfsdottir HL, Indridason OS, Palsson R, Edvardsson VO. Impact of nephrolithiasis on kidney function. BMC Nephrol. 2015;16:1–7. https://doi.org/10.1186/s12882-015-0126-1
- Shoag J, Halpern J, Goldfarb DS, Eisner BH. Risk of chronic and end-stage kidney disease in patients with nephrolithiasis. J Urol. 2014;192(5):1440–1445. https://doi.org/10.1016/j.juro.2014.05.117
- Khan SR. Nephrocalcinosis in animal models with and without stones. Urol Res. 2010;38:429–438. https://doi.org/10.1007/s00240-010-0303-4
- Gambaro G, Croppi E, Bushinsky D, et al. The risk of chronic kidney disease associated with urolithiasis and its urological treatments: a review. J Urol. 2017;198(2):268–273. https://doi.org/10.1016/j.juro.2016.12.135
- Uribarri J, Oh MS, Carroll HJ. The first kidney stone. Ann Intern Med. 1989;111(12):1006–1009. https://doi.org/10.7326/0003-4819-111-12-1006
- Hyams ES, Matlaga BR. Economic impact of urinary stones. Transl Androl Urol. 2014;3(3):278–283. https://doi.org/10.3978/j.issn.2223-4683.2014.07.02
- Faraday M, Hubbard H, Kosiak B, Dmochowski R. Staying at the cutting edge: a review and analysis of evidence reporting and grading; the recommendations of the American Urological Association. BJU Int. 2009;104(3):294–297. https://doi.org/10.1111/j.1464-410X.2009.08729.x
- Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:e924. https://doi.org/10.1136/bmj.39489.470347.AD
- Hughes T, Ho HC, Pietropaolo A, Somani BK. Guideline of guidelines for kidney and bladder stones. Turk J Urol. 2020;46(Suppl 1):S104–S112. https://doi.org/10.5152/tud.2020.20315
- Jebir RM, Mustafa YF. Kidney stones: natural remedies and lifestyle modifications to alleviate their burden. Int Urol Nephrol. 2024;56:1025–1033. https://doi.org/10.1007/s11255-023-03764-1
- Maline GE, Goldfarb DS. Climate change and kidney stones. Curr Opin Nephrol Hypertens. 2024;33(1):89–96. https://doi.org/10.1097/MNH.0000000000000931
- Wei B, Tan W, He S, Yang S, Gu C, Wang S. Association between drinking status and risk of kidney stones among United States adults: NHANES 2007–2018. BMC Public Health. 2024;24:e820. https://doi.org/10.1186/s12889-024-18307-1
- Windisch O, Benamran D, Vaessen C. Surgical anatomy of kidneys and adrenals. In: John H, Wiklund P, eds. Robotic Urology. Springer, Cham; 2024:191–101. https://doi.org/10.1007/978-3-031-49428-4_5
- Clark‐Price SC, Fischer JR. Physiology, pathophysiology, and anesthetic management of patients with renal disease. In: Lamont L, Grimm K, Robertson S, Love L, Schroeder C, eds. Veterinary Anesthesia and Analgesia: The Sixth Edition of Lumb and Jones. Wiley; 2024:922–943. https://doi.org/10.1002/9781119830306.ch43
- Herring LC. Observations on the analysis of ten thousand urinary calculi. J Urol. 1962;88(4):545–562. https://doi.org/10.1016/S0022-5347(17)64842-0
- Daudon M, Hennequin C, Lacour B, et al. Sex- and age-related composition of 10,617 calculi analyzed by infrared spectroscopy. Urol Res. 1995;23:319–326. https://doi.org/10.1007/BF00300021
- Mandel NS, Mandel GS. Urinary tract stone disease in the United States veteran population. I. Geographical frequency of occurrence. J Urol. 1989;142(6):1513–1515. https://doi.org/10.1016/S0022-5347(17)39144-9
- Mandel NS, Mandel GS. Urinary tract stone disease in the United States veteran population. II. Geographical analysis of variations in composition. J Urol. 1989;142(6):1516–1521. https://doi.org/10.1016/S0022-5347(17)39145-0
- Pak CY, Poindexter JR, Adams-Huet B, Pearle MS. Predictive value of kidney stone composition in the detection of metabolic abnormalities. Am J Med. 2003;115(1):26–32. https://doi.org/10.1016/S0002-9343(03)00201-8
- Pak CY, Kaplan R, Bone H, Townsend J, Waters O. A simple test for the diagnosis of absorptive, resorptive, and renal hypercalciurias. N Engl J Med. 1975;292(10):497–500. https://doi.org/10.1056/NEJM197503062921002
- Pacifici R, Rothstein M, Rifas L, et al. Increased monocyte interleukin-1 activity and decreased vertebral bone density in patients with fasting idiopathic hypercalciuria. J Clin Endocrinol Metab. 1990;71(1):138–145. https://doi.org/10.1210/jcem-71-1-138
- Pietschmann F, Breslau NA, Pak CY. Reduced vertebral bone density in hypercalciuric nephrolithiasis. J Bone Miner Res. 1992;7(12):1383–1388. https://doi.org/10.1002/jbmr.5650071205
- Moe O, Abate N, Sakhaee K. Normouricosuric uric acid urolithiasis: a systemic disease with defective renal acidification. Endocrinol Metab Clin North Am. 2002;31:895–914. https://doi.org/10.1016/S0889-8529(02)00032-4
- Malluche HH, Tschoepe W, Ritz E, Meyer-Sabellek W, Massary S. Abnormal bone histology in idiopathic hypercalciuria. J Clin Endocrinol Metab. 1980;50(4):654–658. https://doi.org/10.1210/jcem-50-4-654
- Hamm LL, Hering-Smith KS. Pathophysiology of hypocitraturic nephrolithiasis. Endocrinol Metab Clin. 2002;31(4):885–893. https://doi.org/10.1016/S0889-8529(02)00031-2
- Pak C, Adams-Huet B, Poindexter J, Pearle M, Peterson R, Moe O. Stone disease rapid communication: Relative effect of urinary calcium and oxalate on saturation of calcium oxalate. Kidney Int. 2004;66:2032–2037.
- Cheraghian B, Meysam A, Hashemi SJ, et al. Kidney stones and dietary intake in adults: a population-based study in southwest Iran. BMC Public Health. 2024;24:e955. https://doi.org/10.1186/s12889-024-18393-1
- Edvardsson VO, Goldfarb DS, Lieske JC, et al. Hereditary causes of kidney stones and chronic kidney disease. Pediatr Nephrol. 2013;28:1923–1942. https://doi.org/10.1007/s00467-012-2329-z
- Beara-Lasic L, Edvardsson VO, Palsson R, Lieske JC, Goldfarb DS, Milliner DS. Genetic causes of kidney stones and kidney failure. Clin Rev Bone Miner Metab. 2012;10:2–18. https://doi.org/10.1007/s12018-011-9113-7
- Wu M, Liu M, Zhang Y, et al. Serum HDL partially mediates the association between exposure to volatile organic compounds and kidney stones: A nationally representative cross-sectional study from NHANES. Sci Total Environ. 2024;907:e167915. https://doi.org/10.1016/j.scitotenv.2023.167915
- Tamborino F, Cicchetti R, Mascitti M, et al. Pathophysiology and main molecular mechanisms of urinary stone formation and recurrence. Int J Mol Sci. 2024;25(5):e3075. https://doi.org/10.3390/ijms25053075
- Dong C, Zhou J, Su X, et al. Understanding formation processes of calcareous nephrolithiasis in renal interstitium and tubule lumen. J Cell Mol Med. 2024;28(7):e18235. https://doi.org/10.1111/jcmm.18235
- Coe FL, Parks JH, Asplin JR. The pathogenesis and treatment of kidney stones. N Engl J Med. 1992;327(16):1141–1152. https://doi.org/10.1056/NEJM199210153271607
- Devuyst O, Thakker RV. Dent's disease. Orphanet J Rare Dis. 2010;5:e28. https://doi.org/10.1186/1750-1172-5-28
- Shrimpton AE, Hoopes RR Jr, Knohl SJ, et al. OCRL1 mutations in Dent 2 patients suggest a mechanism for phenotypic variability. Nephron Physiol. 2009;112(2):27–36. https://doi.org/10.1159/000213506
- Tosetto E, Graziotto R, Artifoni L, et al. Dent’s disease and prevalence of renal stones in dialysis patients in Northeastern Italy. J Hum Genet. 2006;51:25–30. https://doi.org/10.1007/s10038-005-0317-x
- Diéguez L, Pilco M, Butori S, et al. Dent’s disease: a cause of monogenic kidney stones and nephrocalcinosis. J Pers Med. 2024;14(6):e623. https://doi.org/10.3390/jpm14060623
- Wang X, Wang Q. Current dietary and medical prevention of renal calcium oxalate stones. Int J Gen Med. 2024;17:1635–1649. https://doi.org/10.2147/IJGM.S459155
- Michael M, Harvey E, Milliner DS, et al. Diagnosis and management of primary hyperoxalurias: best practices. Pediatr Nephrol. 2024;39:3143–3155. https://doi.org/10.1007/s00467-024-06328-2
- Cochat P, Rumsby G. Primary hyperoxaluria. N Engl J Med. 2013;369(7):649–658. https://doi.org/10.1056/NEJMra1301564
- Bacchetta J, Wood KD. Primary hyperoxaluria type 1: time for prime time? Clin Kidney J. 2022;15:i1–i3. https://doi.org/10.1093/ckj/sfab233
- Demoulin N, Aydin S, Gillion V, Morelle J, Jadoul M. Pathophysiology and management of hyperoxaluria and oxalate nephropathy: a review. Am J Kidney Dis. 2022;79(5):717–727. https://doi.org/10.1053/j.ajkd.2021.07.018
- Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8:467–475. https://doi.org/10.1038/nrneph.2012.113
- Abou-Elela A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: a narrative review. J Adv Res. 2017;8(5):513–527. https://doi.org/10.1016/j.jare.2017.04.005
- Isaka Y, Takabatake Y, Takahashi A, Saitoh T, Yoshimori T. Hyperuricemia-induced inflammasome and kidney diseases. Nephrol Dial Transplant. 2016;31(6):890–896. https://doi.org/10.1093/ndt/gfv024
- Cheungpasitporn W, Thongprayoon C, Mao MA, et al. Incidence of kidney stones in kidney transplant recipients: a systematic review and meta-analysis. World J Transplant. 2016;6(4):790–797. https://doi.org/10.5500/wjt.v6.i4.790
- Levy FL, Adams-Huet B, Pak CY. Ambulatory evaluation of nephrolithiasis: an update of a 1980 protocol. Am J Med. 1995;98(1):50–59. https://doi.org/10.1016/S0002-9343(99)80080-1
- Bolen E, Stern K, Humphreys M, et al. Urine metabolic risk factors and outcomes of patients with kidney transplant nephrolithiasis. Clin Kidney J. 2022;15(3):500–506. https://doi.org/10.1093/ckj/sfab208
- Bunnapradist S, Neri L, Wong W, et al. Incidence and risk factors for diarrhea following kidney transplantation and association with graft loss and mortality. Am J Kidney Dis. 2008;51(3):478–486. https://doi.org/10.1053/j.ajkd.2007.11.013
- Rudman D, Dedonis JL, Fountain MT, et al. Hypocitraturia in patients with gastrointestinal malabsorption. N Engl J Med. 1980;303(12):657–661. https://doi.org/10.1056/NEJM198009183031201
- Kanbay M, Copur S, Bakir CN, Hatipoglu A, Sinha S, Haarhaus M. Management of de novo nephrolithiasis after kidney transplantation: A comprehensive review from the European Renal Association CKD-MBD working group. Clin Kidney J. 2024;17(2):sfae023. https://doi.org/10.1093/ckj/sfae023
- Srivastav S, Guleria K, Sharma S. Predictive machine learning approaches for chronic kidney disease. IEEE. 2023:1–5. https://doi.org/10.1109/INCET57972.2023.10170425
- Wu Y, Mo Q, Xie Y, et al. A retrospective study using machine learning to develop predictive model to identify urinary infection stones in vivo. Urolithiasis. 2023;51:e84. https://doi.org/10.1007/s00240-023-01457-z
- Doyle P, Gong W, Hsi R, Kavoussi N. PD34-06 machine learning prediction of symptomatic kidney stone recurrence using 24-hour urine data and electronic health record-derived features. J Urol. 2023;209(Suppl 4):e922. https://doi.org/10.1097/JU.0000000000003327.06
- Worster A, Preyra I, Weaver B, Haines T. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med. 2002;40(3):280–286. https://doi.org/10.1067/mem.2002.126170
- Akram M, Jahrreiss V, Skolarikos A, et al. Urological guidelines for kidney stones: Overview and comprehensive update. J Clin Med. 2024;13(4):e1114. https://doi.org/10.3390/jcm13041114
- Frassetto L, Kohlstadt I. Treatment and prevention of kidney stones: an update. Am Fam Physician. 2011;84(11):1234–1242.
- Türk C, Petřík A, Sarica K, et al. EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol. 2016;69(3):468–474. https://doi.org/10.1016/j.eururo.2015.07.040
- Wright P, English P, Hungin A, Marsden S. Managing acute renal colic across the primary-secondary care interface: a pathway of care based on evidence and consensus. BMJ. 2002;325:e1408. https://doi.org/10.1136/bmj.325.7377.1408
- Pearle MS, Goldfarb DS, Assimos DG, et al. Medical management of kidney stones: AUA guideline. J Urol. 2014;192(2):316–324. https://doi.org/10.1016/j.juro.2014.05.006
- Doyle P, Gong W, Hsi R, Kavoussi N. Machine learning models to predict kidney stone recurrence using 24-hour urine testing and electronic health record-derived features. Res Sq. 2023:rs.3.rs-3107998. https://doi.org/10.21203/rs.3.rs-3107998/v1
- Srikanth V. Chronic kidney disease prediction using machine learning algorithms. Int J Techno Eng. 2023;15(1):106–122.
- Kaur C, Kumar MS, Anjum A, Binda M, Mallu MR, Al Ansari MS. Chronic kidney disease prediction using machine learning. J Adv Inf Technol. 2023;14(2):384–391. https://doi.org/10.12720/jait.14.2.384-391
- Gulhane M, Kumar S, Choudhary S, et al. Integrative approach for efficient detection of kidney stones based on improved deep neural network architecture. SLAS Technol. 2024;29(4):e100159. https://doi.org/10.1016/j.slast.2024.100159
- Shee K, Chan C, Liu A, et al. PD34-05 A novel machine-learning algorithm to predict stone recurrence with 24-hour urine data. J Urol. 2023;209(Suppl 4):e921. https://doi.org/10.1097/JU.0000000000003327.05
- Anil D, Naimudden S, Reddy AS, Lavanya A. Prediction of chronic kidney disease using various machine learning algorithms. IEEE. 2023:156–161. https://doi.org/10.1109/ICIDCA56705.2023.10100255
- Zeng H, Liu Z, He Y, et al. Multivitamins co-intake can reduce the prevalence of kidney stones: a large-scale cross-sectional study. Int Urol Nephrol. 2024;56:2991–3001. https://doi.org/10.1007/s11255-024-04021-9
- Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones: Systematic review and meta-analysis. BMJ. 2016;355:i6112. https://doi.org/10.1136/bmj.i6112
- Bargagli M, Anderegg MA, Fuster DG. Effects of thiazides and new findings on kidney stones and dysglycemic side effects. Acta Physiol. 2024;240(7):e14155. https://doi.org/10.1111/apha.14155
- Emiliani E, Subiela JD, Regis F, Angerri O, Palou J. Over 30-year experience on the management of graft stones after renal transplantation. Eur Urol Focus. 2018;4(2):169–174. https://doi.org/10.1016/j.euf.2018.06.007
- Normand M, Haymann J-P, Daudon M. Medical treatment of uric acid kidney stones. Can Urol Assoc J. 2024;18(11):E339–345. https://doi.org/10.5489/cuaj.8774
- Lam JS, Greene TD, Gupta M. Treatment of proximal ureteral calculi: Holmium:YAG laser ureterolithotripsy versus extracorporeal shock wave lithotripsy. J Urol. 2002;167(5):1972–1976. https://doi.org/10.1016/S0022-5347(05)65065-3
- Sharma NKH. A comprehensive review on kidney stones, its treatment and recent advancement. Int J Med Sci Dental Res. 2024;7(1):16–23.
- Lingeman JE, Coury TA, Newman DM, et al. Comparison of results and morbidity of percutaneous nephrostolithotomy and extracorporeal shock wave lithotripsy. J Urol. 1987;138(3):485–490. https://doi.org/10.1016/S0022-5347(17)43236-8
- Pearle MS, Lingeman JE, Leveillee R, et al. Prospective, randomized trial comparing shock wave lithotripsy and ureteroscopy for lower pole caliceal calculi 1 cm or less. J Urol. 2005;173(6):2005–2009. https://doi.org/10.1097/01.ju.0000158458.51706.56
- Torricelli FCM, Danilovic A, Vicentini FC, Marchini GS, Srougi M, Mazzucchi E. Extracorporeal shock wave lithotripsy in the treatment of renal and ureteral stones. Rev Assoc Med Bras. 2015;61(1):65–71. https://doi.org/10.1590/1806-9282.61.01.065
- Dasgupta R, Cameron S, Aucott L, et al. Shockwave lithotripsy versus ureteroscopic treatment as therapeutic interventions for stones of the ureter (TISU): a multicentre randomised controlled non-inferiority trial. Eur Urol. 2021;80(1):46–54. https://doi.org/10.1016/j.eururo.2021.02.044
- Schlomer BJ. Urologic treatment of nephrolithiasis. Curr Opin Pediatr. 2020;32(2):288–294. https://doi.org/10.1097/MOP.0000000000000849
- Swearingen R, Roberts WW, Wolf JS. Ureteroscopy for nephrolithiasis in transplanted kidneys. Can J Urol. 2015;22(2):7727–7731.
- Jones P, Elmussareh M, Aboumarzouk OM, Mucksavage P, Somani BK. Role of minimally invasive (micro and ultra-mini) PCNL for adult urinary stone disease in the modern era: evidence from a systematic review. Curr Urol Rep. 2018;19:e27. https://doi.org/10.1007/s11934-018-0764-5
- Whitehurst L, Jones P, Somani BK. Mortality from kidney stone disease (KSD) as reported in the literature over the last two decades: a systematic review. World J Urol. 2019;37:759–776. https://doi.org/10.1007/s00345-018-2424-2
- Liu M, Chen J, Gao M, et al. Preoperative midstream urine cultures vs renal pelvic urine culture or stone culture in predicting systemic inflammatory response syndrome and urosepsis after percutaneous nephrolithotomy: a systematic review and meta-analysis. J Endourol. 2021;35(10):1467–1478. https://doi.org/10.1089/end.2020.1140
- Sharbaugh A, Morgan Nikonow T, Kunkel G, Semins MJ. Contemporary best practice in the management of staghorn calculi. Ther Adv Urol. 2019;11:1–9. https://doi.org/10.1177/1756287219847099
- Le Duc A. Les complications immédiates de la chirurgie percutanée du rein [Immediate complications of percutaneous surgery of the kidney]. Prog Urol. 1991;1(1):31–35.
- Benchekroun A, Iken A, Karmouni T, et al. La néphrolithotomie percutanée. À propos de 211 cas. Ann Urol. 2001;35(6):315–318. https://doi.org/10.1016/S0003-4401(01)00051-1
- Mbodji MM, Jalloh M, Ndoye M, et al. Treatment of kidney stones by percutaneous nephrolithotomy: evaluation of the results of the first series of our experience in the Urology Department of the Idrissa Pouye General Hospital in Dakar. Open J Urol. 2024;14(2):104–114. https://doi.org/10.4236/oju.2024.142011
- Wyatt J, Kolettis PN, Burns JR. Treatment outcomes for percutaneous nephrolithotomy in renal allografts. J Endourol. 2009;23(11):1821–1824. https://doi.org/10.1089/end.2008.0115
- Krambeck AE, LeRoy AJ, Patterson DE, Gettman MT. Percutaneous nephrolithotomy success in the transplant kidney. J Urol. 2008;180(6):2545–2549. https://doi.org/10.1016/j.juro.2008.08.032
- Reddy P, Hulbert J, Lange P, et al. Percutaneous removal of renal and ureteral calculi: experience with 400 cases. J Urol. 1985;134(4):662–665. https://doi.org/10.1016/S0022-5347(17)47372-1
- Singh AG, Jairath A, Balaji SS, et al. Changing trends in the endourological management of urolithiasis in anomalous kidneys. BJU Int. 2019;123(2):318–327. https://doi.org/10.1111/bju.14575
- Spinos T, Tatanis V, Seitz C, Liatsikos E, Kallidonis P. Percutaneous nephrolithotomy (PCNL) versus other treatments for stone management in horseshoe kidneys: a systematic review. Arab J Urol. 2024;22(4):243–252. https://doi.org/10.1080/20905998.2024.2312699
- Boissier R, Rodriguez-Faba O, Zakri RH, et al. Evaluation of the effectiveness of interventions on nephrolithiasis in transplanted kidney. Eur Urol Focus. 2023;9(3):491–499. https://doi.org/10.1016/j.euf.2022.11.019
- Wong KA, Olsburgh J. Management of stones in renal transplant. Curr Opin Urol. 2013;23(2):175–179. https://doi.org/10.1097/MOU.0b013e32835d3097