
| Review | Open Access |
|---|
Impact of Drug Information Centers on Healthcare Outcomes: A Narrative Review of Pre- and Post-implementation in South Asian Countries |
 |
|---|
![]() Tharsika Kanthasamy1 , and Muhammad Ali2*
Tharsika Kanthasamy1 , and Muhammad Ali2*
1Department of Pharmacy, Faculty of Allied Health Sciences, University of Peradeniya, Sri Lanka
2Department of Pharmacy Practice and Pharmaceutics, Faculty of Pharmacy, Salim Habib University, Karachi, Pakistan
Drug Information Centers (DICs) play a vital role in the provision of accurate, reliable, and updated information on medications to healthcare professionals as well as the general public. These centers are now taking a step forward in the healthcare field. This narrative review aimed to analyze the evolution and impact of DICs on South Asian countries, such as India, Pakistan, Bangladesh, Sri Lanka, and Nepal. Furthermore, it also discussed the role of DICs in healthcare as well as the barriers in the establishment of such services in developing countries. The established DICs in these South Asian countries improves rational drug use and enhances patient safety even though there are significant challenges to establish and expand these centers in South Asia. The DICs established in India, Nepal, and Pakistan have significantly contributed in the enhancement of patient safety and rational use of medications. However, there are challenges in establishing DICs in Sri Lanka and Bangladesh. Innovative strategies, such as telemedicine services and collaboration with healthcare institutes, academics, and regulatory authorities would expand the services of DICs across South Asia.
1. INTRODUCTION
Drug Information Centers (DICs) are formalized units, established within healthcare systems that aim to provide reliable, accurate, and updated drug-related information in a timely manner to healthcare providers and the general public [1–5]. The services of DICs play a pivotal role in improving the rational medication usage, prevention of medication errors, as well as adverse drug events [1–5]. The functions of DICs underscore its need for establishment and expansion of such services in developing countries. Provision of drug information, support in education, academic, and research area, pharmacovigilance activities, as well as medication counseling have significant impact on overall healthcare improvement [1, 4–7].
Antimicrobial resistance (AMR) is an emerging challenge in low- and middle-income countries than high-income nations. By offering accurate information on proper antibiotic use and counseling patients, DICs actively contribute to combating AMR [4–6, 8]. The DICs extended their rules during COVID-19 pandemic, which proved to be a crucial forward step for the establishment and effectiveness of DICs in lower middle-income countries [9, 10]. The COVID-19 pandemic may act as a bridge to provide the public with objective, trustworthy information about COVID-19, its management, and its treatment strategy [9]. Additionally, the DICs disseminated educational materials regarding the COVID-19 pandemic [10]. Moreover, these centers serve as hubs for academic and research activities, providing opportunities for clinical pharmacy training and continuing professional development for healthcare professionals [11, 12].
However, developing countries often face unique challenges, such as a higher prevalence of self-medication practices and limited access to unbiased drug information [1, 4–6, 13, 14]. Traditional healthcare systems, such as Siddha, Unani, and Ayurveda also contribute to polypharmacy and the risk of unknown drug interactions [4, 5]. In countries, such as India, Pakistan, Nepal, Bangladesh, and Sri Lanka, these challenges underscore the critical need for establishing and maintaining well-functioning DICs to address these healthcare concerns effectively.
This narrative review aimed to compare healthcare outcomes before and after the implementation of DICs in South Asian countries, providing insights into their functions, contributions, and impact. Additionally, it sought to identify the barriers and facilitators affecting the successful operation of DICs in this region, offering a foundation for further improvements in healthcare systems.
- METHODOLOGY
Articles were searched using developed keywords, such as “drug information centers”, “drug information services (DISs)”, “medicine information”, “South Asia”, and “healthcare” via Google Scholar, Pubmed, and google search engine. A total of 58 articles containing full research articles (33), review articles (19), commentary articles (3), letters to editor (2), and reports (1) were screened and included. Table 1 shows the objectives of selected studies in this review.
Table 1. Objectives of the Concerned Studies
| S.no | Literature Review | Objectives |
|---|---|---|
| 1 | A reflective commentary on drug information services (DISs) in Nepal | To draw attention towards the recent scenario of DISs in Nepal, to discuss the challenges in establishing and running DICs, and to analyze the ways of strengthening DICs |
| 2 | An overview on DICs | To identify various concepts of DICs in different countries and to understand the differences in their functioning |
| 3 | Overview of status and challenges of DISs in India | This analyzes the status and challenges of DISs in India |
| 4 | Status of DICs and DISs in India | To highlight the current status of DICs and requirements to develop its services further |
| 5 | Perspectives on DISs in Nepal | This study discussed the need of DICs in Nepal, the problems in the effective running of DICs, and the current status of DICs in Nepal |
| 6 | The impact of DICs to improve medication safety in Saudi Arabia | To assess the use of DICs by healthcare professionals in Saudi Arabia |
| 7 | The functions of DICs and the challenges associated with establishing DICs in India | To understand the roles of DICs and the actions to be taken in establishing a DIC in India |
| 8 | The evolution of DICs and specialists | To discuss the evolution of DICs and role of drug information specialists |
| 9 | The functions of DICs at the Manipal Teaching Hospital | To discuss the various functions carried out by the DICs at Manipal Teaching Hospital |
| 10 | Assessment of DISs and their utilization in a tertiary care teaching hospital | To assess the usage of DISs and create awareness for the utilization of DICs |
| 11 | Perspectives on DICs in developing countries and challenges in developing DICs in those countries | To analyze the role of DICs in developing countries, requirements for setting up a DIC, and challenges while establishing a DIC in developing countries |
| 12 | Assessment of new DICs in Ethiopia | To analyze the use and status of DICs located at university teaching hospitals in Ethiopia |
| 13 | DICs - need of the hour | To discuss about DICs in India, requirements for setting up a DIC, and challenges in running a DIC in India |
| 14 | European DICs | To discuss about European DICs |
| 15 | Perceptions of physicians and patients on DISs in a tertiary care hospital | To implement DISs, to provide information on drugs, and to promote awareness on DICs |
| 16 | Hospital-based DISs in developing countries | To analyze the advantages of DICs based in teaching hospitals |
| 17 | The need for drug and poison information centers in Pakistan | To ascertain the need of drug and poison information centers in Karachi |
| 18 | Perspectives on hospital pharmacy practice in Bangladesh | To sum up the current status of pharmacy practices and identify the pharmacist’s roles |
| 19 | Self-medication practices and factors among undergraduates | To determine the factors associated with self-medication practices and create awareness on self-medication practices |
| 20 | Knowledge of prescribed medication information among non-English proficient patients in Sri Lanka | To evaluate the knowledge on prescribed medications and explore factors in determining the knowledge |
| 21 | Evaluation of performance of DICs in a tertiary care hospital in South India | To evaluate the performance of DICs in the provision of drug information |
| 22 | Prevalence of self-medication practices in India | To systematically review the prevalence of self-medication and its associated factors |
| 23 | Self-medication and non-prescription practices in Nepal | To obtain data on self-prescribing and analyze the factors influencing self-medication |
| 24 | The state of primary healthcare in South Asia | To investigate the strengths and deficiencies of different primary healthcare approaches in the South Asian region and provide a comparative analysis between countries |
| 25 | A systematic review on factors and consequences of polypharmacy practices in South Asia | To sum up the factors and consequences of polypharmacy practices |
| 26 | Systematic review and analysis on factors associated with polypharmacy | To analyze the prevalence and factors associated with polypharmacy practices |
| 27 | Assessment of a drug and poison information center in Pakistan | To evaluate the use of drug and poison information center services |
| 28 | Pharmacovigilance practices in South Asian countries | To examine the current pharmacovigilance activity and make recommendations for safe monitoring of medicines |
| 29 | Scoping review on the need for drug information in Asia and Africa | To quantify and map the English language concerns in written medication information |
| 30 | Self-medication practices in Pakistan and the need for proper monitoring | To emphasize the need for proper monitoring on self-medication practices in Pakistan |
| 31 | Assessment on the role of DICs towards safety of drug usage | To analyze the services provided by the DICs at Manipal Teaching Hospital |
| 32 | A cross sectional study on patient knowledge on prescribed drugs and package inserts | To assess the knowledge and awareness towards package inserts |
| 33 | Evaluation of patient information leaflets on topical medications | To evaluate the quality of patient information leaflets drugs available in the market and to analyze the design, content, and readability |
| 34 | Analysis on package inserts available in Pakistan | To assess the information written on pharmaceutical package inserts of products marketed in Pakistan |
| 35 | Evaluation of errors found in patient information leaflets available with medicines in Pakistan | To assess and evaluate the errors found in leaflets available with medicines in Pakistan |
| 36 | A retrospective study on the quality of information available in product information insert | To evaluate the completeness and appropriateness of information against references |
| 37 | Evaluation of information on drug-drug interactions in the medicine package leaflets | To evaluate the extent and nature of information on drug interactions presented in the package leaflets |
| 38 | Antimicrobial resistance surveillance in South East Asian and South Asian countries | To explore the state of AMR and highlight the opportunities and progress in tackling AMR |
| 39 | Evaluation on sources of drug information and impact of DICs on Indian community | To discuss the role of DICs and rational use of medications |
| 40 | Assessment and evaluation of DISs provided in a teaching hospital in India | To evaluate the types of queries on drugs and quality of services provided by the DICs |
| 41 | Assessment of DISs in Kanchipuram Tertiary Care Hospital | To assess DISs in hospitals over eight months |
| 42 | Evaluation of quality of services provided by the DICs in a tertiary care hospital | To assess the quality of services provided by the DICs over three years |
| 43 | Review on DISs in a teaching hospital, India | To review the activities carried out by DICs |
| 44 | Establishment of a drug information unit and pharmacovigilance cell in a provincial hospital of Nepal | To brief about the establishment of a drug information unit and pharmacovigilance cell |
| 45 | Evaluation of utilization of drug information resources by healthcare providers | To study the drug information resources used by medical practitioners and the need for a drug information unit |
| 46 | Evaluation of promotional materials in a hospital in Nepal | To analyze whether the promotional materials met World Health Organization’s (WHO) ethical criteria for medicinal drug promotion |
| 47 | Analysis of potential drug–drug interactions in hospital settings in Pakistan | To investigate the frequency of potential drug–drug interactions and analyze the management of frequently identified interactions |
| 48 | Assessment of the current state of pharmacovigilance system in Pakistan | To evaluate the functions of pharmacovigilance system |
| 49 | Retrospective analysis on potential drug–drug interactions among elderly patients hospitalized in Sri Lanka | To study how hospitalization affects potential drug-drug interactions |
| 50 | DISs and their role in rational drug therapy | To discuss the clinical impacts of DICs and their future |
| 51 | Novel role of DICs during the COVID-19 pandemic | To explore the additional roles of DICs with respect to drug information provision during pandemic times |
| 52 | Satisfactory outcomes of DICs and their services | To evaluate the outcomes and user satisfaction levels of pharmacist-led tele-health services |
| 53 | Dissemination of awareness and educational materials on COVID-19 pandemic by a regional DIC | To describe the distribution and acceptance of COVID-19 educational materials by DICs of Brazilian public university |
| 54 | Perspectives on the roles of Sri Lankan pharmacists | To highlight the need to strengthen the pharmacist’s role in Sri Lanka |
| 55 | The impact of DISs on drug safety, clinical outcomes, and patient care in UK | To analyze the impact of medicine information centers on patient care and patient safety |
| 56 | Impact on drug queries at DICs after the awareness programs on DISs in a public hospital, Malaysia | To analyze the DISs provided by a public hospital, Malaysia |
| 57 | Use of a pilot DIC | To assess the use of pilot DICs established in Uganda |
| 58 | Quality evaluation and survey on the need for DICs | To analyze the services provided by DICs in Egypt and evaluate the effectiveness of DICs |
3. HISTORICAL DEVELOPMENT OF DRUG INFORMATION CENTER (DIC)
The first DIC was established at the University of Kentucky in 1962 in the United States [3, 4, 5, 15] and earlier, in 1960, in the United Kingdom [3]. In Latin America, Brazil established its first DIC in 2001, followed by Costa Rica in 2003 [3]. Similarly, Singapore inaugurated its DIC in 1980 [3].
In South Asia, the progress of DICs varies across countries. In India, the DICs were inaugurated in 1997 in Jagadguru Sri Shivarathreeshwara, Mysore, Trivandrum Medical Faculty, and Karnataka State Pharmacy Council [4, 5]. Later, the Karnataka State Pharmacy Council collaborated with WHO’s India office and established five DICs in Haryana, Goa, Assam, Rajastan, and Chhattisgarth in 2007 [8, 13]. Now, there are about nine independent DICs and over 15 hospital-attached DICs in India which are working successfully [4, 5]. Nepal established its first DIC at Tribhuvan University Teaching Hospital in 1994 [1, 4, 16]. Subsequently, in 1996, the Drug Information Network of Nepal was developed to provide high-quality drug information [1, 12], leading to the establishment of several additional DICs that collaborated within this network. These included the College of Medical Sciences, KIST Teaching Hospital, B. P Koirata Institute of Health, and Resource for Primary Healthcare [1, 4, 16]. In 2003, the first DIC in private sector was inaugurated in Manipal Teaching Hospital, Pokhara [12]. Pakistan’s first DIC was founded in 1995 at Aga Khan University Hospital, although there is no official data on the total number of DICs currently available in the country [15].
In contrast, Bangladesh lacks structured DICs entirely [17, 18]. Similarly, in Sri Lanka, the Department of Pharmacology at the Colombo Medical Faculty initiated a Drug Information Service in January 1999 [19]. However, there are no regulated or structured DICs within government hospitals in Sri Lanka, and the Ministry of Healthcare and Nutrition emphasizes the government to fund a national medicines information center [20]. This highlights the varying levels of development and implementation of DICs across South Asia.
4. ROLE OF DRUG INFORMATION CENTERS (DICS) IN HEALTHCARE
The role of DICs in healthcare is indispensable, offering services that elevate the pharmacy profession and enhance healthcare outcomes. Their functions are diverse and impactful, as outlined below:
4.1. Key Functions of DICs in Healthcare
DICs deliver reliable, accurate, and up-to-date medication information. They address queries related to drug interactions, availability, substitutes for specific medications, and drug identification [1–3, 8, 11, 13, 14, 21, 22].
DICs provide targeted counseling for illiterate patients, patients prescribed medical devices or special dosage forms (e.g., suppositories, pessaries), patients on high-risk medications (e.g., antiepileptics, antibiotics), and pediatric and geriatric patients, and those with poor medication compliance [6]. By offering proper counseling, DICs help minimize adverse drug reactions (ADRs) and other unwanted side effects, such as AMR [1–3, 6, 11, 13, 14, 21].
DIC monitors and assesses medication safety alerts communicated by drug manufacturers, drug distributors, and medical regulatory authorities [6].
DICs work closely with drug and therapeutic committees to evaluate new drugs for hospital formularies and to identify safety concerns or newly reported side effects [3, 6, 14]. They also collaborate with pharmaceutical manufacturers to obtain information on the quality, dosage forms, and formulations of new drugs [3].
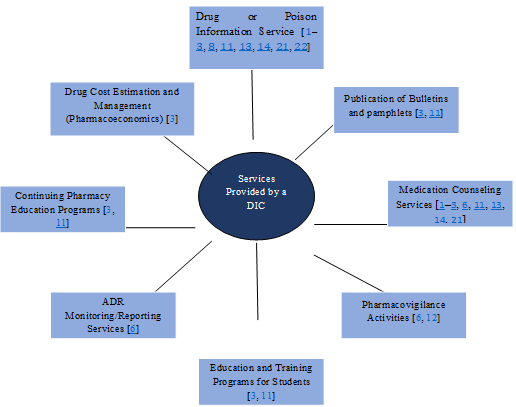
Figure 1. Roles of DIC
DICs support the education of undergraduate and postgraduate students, fostering an interest in pharmacology and guiding them in addressing drug-related queries and counseling patients [3, 11]. Furthermore, they play a key role in research areas, such as pharmacoepidemiology, Pharmacoeconomics, and the rational use of medications [3]. Additionally, DICs publish drug bulletins, case reports, and reviews, benefitting academic institutions and the general public [3, 11]. They also organize Continuing Professional Development (CPD) and education programs for healthcare providers [3, 11].
Most of the DIC members participate in ward rounds and identify drug-related queries arising during the rounds [6]. The DICs coordinate and support various medication programs, such as AMR awareness campaigns, vaccination programs, and preventive missions for infection controls and pandemic situations [1, 8, 10, 23].
The DICs actively participate in ADR monitoring and reporting, ensuring patient safety by identifying and mitigating drug-related risks [6].
The functions and roles of DICs benefit the patients and society by reducing medication and healthcare-related costs [24]. Furthermore, DICs also keep a check on inappropriate usage of medication, reducing medication errors and patient mortality rates by promoting good clinical care practices. This also leads towards an increase in the quality of patient care, improving medication adherence and patient compliance, as well as promoting safe and effective use of medication [1–3, 8, 10, 11, 13, 14, 21, 23, 24].
5. PRE-IMPLEMENTATION SCENARIO OF DRUG INFORMATION CENTERS (DICS) IN SOUTH ASIA
In South Asia, countries such as Nepal, India, Pakistan, Bangladesh, and Sri Lanka have historically faced challenges in accessing reliable and updated drug information [1, 5, 8, 15]. These challenges usually arise due to limited access to current medical literature, insufficient funding for drug information services, poor documentation and lack of quality assurance programs, as well as the continuous introduction of new drug formulations [1, 5, 8].
Additionally, widespread self-medication, polypharmacy, and misuse of over-the-counter drugs, exacerbated by high illiteracy rates and poverty [8, 25], have contributed to improper medication practices and elevated health risks in the region [26–31].
A scoping review [32] highlighted significant deficiencies in the availability and accessibility of drug information across South Asia. Patient information leaflets in countries, such as India, Pakistan, Sri Lanka, and Bangladesh were found to be lengthy, filled with complex medical terminology, and often not written in local languages [33]. Critical drug information, such as drug-drug interactions and proper usage instructions, was frequently missing [34–37]. In many cases, medicine information was available only in English, limiting accessibility for patients who could not read or understand English [25, 31, 34, 38]. A study conducted in Nepal concluded that the information available in the promotional materials, provided by the manufacturers, influences the prescribing patterns of clinicians as Nepal has limited drug information sources [39].
The pharmacovigilance systems and adverse drug reaction reporting mechanisms in South Asia are similarly inadequate [40]. A review study of pharmacovigilance in the region outlined 11 indicators to assess the functionality of pharmacovigilance centers. These included the existence of legal provisions, national pharmacovigilance centers, ADR reporting forms, advisory committees, guidelines, and public health program integration. However, key gaps were identified [40]:
- India and Sri Lanka lacked affiliations between pharmacovigilance centers and regulatory authorities.
- Nepal and Pakistan did not have pharmacovigilance advisory committees.
- No information was available regarding such committees in Sri Lanka.
- Only India, Pakistan, and Bangladesh had integrated pharmacovigilance systems into public health programs, such as immunization initiatives.
According to WHO report, Pakistan lacks a proper disease surveillance system and use of medical information [41]. Additionally, an established clinical pharmacy system does not exist to optimize, manage, and monitor medication usage, leading towards the irrational use of medicines in Pakistan [41]. Furthermore, another study revealed that the ADRs are under reported by healthcare professionals in Pakistan due to lack of knowledge or national ADR reporting system, and the pharmacology vigilant system of Pakistan is not meeting the minimum standards [42].
These inconsistencies could be addressed through the establishment of DICs to monitor drug safety issues and support pharmacovigilance activities effectively.
South Asian countries face additional healthcare challenges including a growing aging population, a rise in non-communicable diseases, and a healthcare system that is a mix of public and private providers [29]. The region also features diverse traditional, complementary, and alternative medicine practices, such as Ayurveda, Siddha, and Unani, which often coexist with conventional medicine [4, 5]. This diversity contributes to polypharmacy, increasing the risk of adverse health outcomes and ADRs [38, 43]. This is because the polypharmacy and comorbidities’ high prevalence of drug-drug interactions can be seen in developing countries [41, 44].
Self-medication is another prevalent issue, with many individuals relying on over-the-counter medications for illness prevention and management [43]. Common practices include reusing the prior prescriptions, consuming leftover medications, improper use of medical devices, and taking advice from family and friends [32]. Poor accessibility to healthcare and the ease of consuming medication as over-the-counter medications are driving factors for these practices observed in India [27], Nepal [28], Bangladesh [29], Sri Lanka [25], and Pakistan [43]. These behaviors result in increased risks of adverse reactions, incorrect diagnosis of diseases, inappropriate treatment regimen, non-adherence to medication, drug abuse and dependence, as well as hospitalization [38, 43].
In South Asian regions, lack of effective drug policies also facilitates the occurrence of these challenges [23, 28]. In Nepal, the regulation of information flow on promotional materials provided by the pharmaceutical manufacturing companies for the American products has not been strictly monitored [39]. In India, lack of access to unbiased and updated information on drugs and poor drug regulation often leads towards irrational drug use [45]. Additionally, the role of pharmacists in Sri Lanka is often restricted to providing limited medicinal information to patients [46].
To address these pressing issues observed in South Asia, DICs may play an important and transformative role in improving the quality of healthcare. These centers have the potential to significantly enhance the rational use of medication and to reduce the risks associated with self-medication, practices, polypharmacy practices, and AMR. These challenges collectively underscore the urgent need for established DICs across South Asia.
6. CHALLENGES IN ESTABLISHING AND RUNNING DICS IN SOUTH ASIA
Despite their potential, DICs in South Asia face several challenges [12, 15, 47] mentioned as follows:
- Limited public awareness about DICs and their services.
- Outdated or unavailable drug information sources.
- Insufficient staffing and financial support.
- Lack of clinical and managerial expertise.
Even though, there are challenges in establishing DICs in South Asia, the established DICs have successfully expanded the services. These services include the provision of accurate and updated medicine information, involvement in pharmacology, vigilance activities, counseling, supporting, and academic and research activities involving continuous professional development programs. Additionally, ADR monitoring and even fighting challenging healthcare situations, such as COVID-19 pandemic are among the services provided by DICs [5, 6, 12, 13, 16, 47, 48]. Innovative approaches, such as telemedical services [10] and collaborations with forensic pharmacology and toxicology departments, drug regulatory authorities, and with other complimentary medication practices could effectively enhance the efficiency of DICs [4, 5].
7. POST-IMPLEMENTATION SCENARIO OF DICS IN SOUTH ASIA
7.1. IndiaThe establishment of DICs in hospitals has significantly improved the quality of healthcare. Studies reveal that 86% of healthcare professionals recognize the value of DICs and 95% of patients believe DICs enhance healthcare quality [47]. For instance, a DIC in a Hyderabad care hospital received positive feedback for providing timely and appropriate responses to drug queries [47]. Similarly, services provided by DICs in Karnataka have been instrumental in promoting rational drug use and improving patient care [48]. Upon the evaluation of drug information services provided by Baseweshwara Medical College Hospital and Research Center Chitradurga, Karnataka, the DICs proved to be efficient for the provision of unbiased services. These services are beneficial to patients as well as healthcare professionals in providing better patient care and updating knowledge on medication use [49].
The DIC in Kasturba Teaching Hospital in South India contributes to the betterment of patient care. This study evaluated the quality of services provided by the DICs and showed that physicians (82%) and patients (16%) were satisfied by these services [50]. Similarly, the studies conducted to evaluate the services provided by the DICs established in SRM Medical College Hospital and Research Center, Kanjipurum [51], Mahatma Gandhi Memorial Hospital [52], and JSS Medical College Hospital [53] revealed that most of the respondents rated the performance of DICs as good. They mentioned receiving appropriate answers for drug-related queries. These studies showed that the drug information services are important for better patient care.
7.2. NepalDICs in Nepal, including those in Lalitpur, Kathmandu, Pokhara, and Kavre, address queries on drug interactions, ADRs, medication availability, costs, and administration methods [1, 12]. Studies highlight that approximately 40% of queries are related to ADRs, underscoring the importance of DICs in mitigating drug-related issues [54].
The drug information unit and pharmacovigilance cell established at Hetauba Hospital in Nepal, delivers information on queries regarding drug allergies, OTC drugs and adverse drug reactions and ADR reporting forms, delivering medication counseling and diabetic diet counseling as well as creating antibiotic awareness [55]. This center also aims to provide information about complimentary and alternate medication in future as well [55].
7.3. PakistanIn Pakistan, a cross-sectional study involving public and private tertiary hospitals in Karachi revealed that over 90% of healthcare professionals emphasized the need for DICs and over 50% of queries were related to drug interactions and dosages [15].
The evaluation of a drug and poison information center operated by pharmacists in Pakistan revealed that the queries received by centers were mainly from general public on patient counseling, disease awareness, and diet counseling with most queries related to indication of drugs, identification of drugs, side effects, and administration [18]. The study also exhibited that the awareness by the activates enhanced the use of such centers, which is a crucial step for effective running of such centers in Pakistan [18].
7.4. Sri LankaThe Department of Pharmacology at Colombo Medical Faculty initiated a Drug Information Service in 1999 [19]. While there are no regulated DICs in government hospitals, the available services provide independent drug information as well as publish drug bulletins for medical practitioners [19].
7.5. Perceptions from Patients and Healthcare OutcomesAn assessment of DICs in a tertiary care hospital in India found that 54.93% of users were satisfied with the information provided. Feedback responses indicated that the performance of drug information services was rated as excellent and good [48]. Similarly, DICs in Manipal Teaching Hospital played a significant role in enhancing knowledge and understanding of patient medication by providing adequate counseling services [12].
In a tertiary care hospital, Hyderabad, feedback from both healthcare professionals and patients highlighted the impact of DICs. Approximately, 38.38% of respondents agreed that drug information services improved patient care, while 88% of healthcare professionals and 92% of patients rated the responses from DICs as excellent. Additionally, 20% of patients showed a keen interest in legal compliances regarding drug information services [47].
A cross-sectional study conducted in Pakistan revealed that 92% of physicians emphasized the need for drug information services in hospitals. Furthermore, 70% of physicians reported that it took them around 15 minutes to search for drug-related information when needed. This indicates that establishing DICs within hospitals could reduce treatment delays and improve the quality of healthcare [15].
In evaluating the utilization of Drug and Poison Information Centers in Pakistan, the study found that services, such as counseling on medications, dietary changes, and diseases were well-received by the general public. The study also suggested that creating awareness about these services could increase their utilization [18].
An assessment of DICs at Kasturba Hospital, Manipal, showed that 65% of users had a positive experience, with the study concluding that DICs support better patient care [50]. Likewise, in tertiary care hospital, Kanchipuram District, 77.4% of respondents rated the performance of DICs as good and suggested expanding the services to operate 24 hours a day [51].
The positive impact of medicine information services on countries, such as the UK, Saudi Arabia, Malaysia, Uganda, and Egypt also aligns with these findings. Data from the UK indicates that medicine information services contributed to a 27.4% reduction in adverse drug reactions, and 77.1% of medicine information services had a positive impact on medication safety [56].
A study conducted in Saudi Arabia found that 88.1% of prescribing errors and 6.6% of administration errors were prevented by drug information specialists. The study emphasized that DICs can significantly enhance the quality of healthcare services in Saudi Arabia [6].
In Sungai Buloh Hospital, Malaysia, research indicated that optimizing therapy through the provision of drug information to both healthcare providers and patients plays a crucial role in improving healthcare outcomes [57].
A pilot DIC established at a university teaching hospital in Uganda reported that the majority of drug-related queries (54.2%) came from physicians, with 41.2% of inquiries related to drug interactions. The study highlighted the necessity of establishing DICs in Uganda, as the pilot center performed well and was enthusiastically utilized by both physicians and patients [58].
Similarly, a study conducted in Egypt to assess the need for DICs revealed that 73.3% of the general public and over 50% of healthcare professionals considered having a DIC to be very important. The study concluded that ensuring safe, effective, and high-quality healthcare can be achieved through the establishment of DICs [59].
Overall, the implementation of DICs in South Asia has proven invaluable in reducing ADRs, minimizing medication errors, and improving patient safety, satisfaction, and knowledge. The DIC plays a crucial role in providing information on rational drug use and keeping healthcare professionals updated. These post-implementation scenarios collectively demonstrate that establishing DICs in healthcare systems, can significantly improve medication safety, healthcare quality, and informed decision-making for both patient and professionals.
8. CONCLUSION
Although, there are challenges in establishing DICs in South Asia, the services of already established centers have expanded from providing reliable drug information, medication, counseling, and pharmacology activities to fighting against sudden pandemic situations, as well as emerging healthcare challenges, such as AMR. These achievements highlight the potential for further establishment and expansion of DIC in South Asian healthcare systems. By highlighting the positive impact of DICs on healthcare, it would be more effective when the government takes initiatives to implement and expand DICs in all tertiary and regional healthcare facilities. This would ensure the widespread use of reliable drug information among patients as well as healthcare professionals. Allocating sufficient funds and resources to support DIC establishments, providing trainings to pharmacists and other staff to run DICs as well as conducting continuous professional development programs for healthcare workers to stay updated and creating awareness among public on the services and functions of DICs would considerably improve the overall healthcare through improving medication safety, minimizing treatment costs and delays, and reducing medication side effects. The government and healthcare stakeholders must take actions to implement these types of services in healthcare facilities.
8.1 Strengths of the StudyThis is the first narrative review that analyzed the development and impact of DICs on South Asia healthcare systems. Additionally, the study provided valuable insights regarding the impact of such centers on healthcare systems. Moreover, the healthcare challenges in South Asia, the role of DICs in tackling those challenges may be obtained in a single glance of this review.
8.2. Limitations of the StudyThe current study only reviewed the available literature without conducting a systematic review or meta-analysis. Studies were included only from accessible data bases and open access articles were analyzed where there was a possibility of omitting relevant subscribed articles. As most of the review studies and research articles were in English, findings and analyses from other languages might be underrepresented. Additionally, the absence of statistical analysis limits the assess to precise impact of DIC on healthcare outcomes.
CONFLICT OF INTEREST
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
No data was generated for this study as this was a review article. All the data analyzed in this article was derived from the cited sources mentioned under references.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Shrestha S, Khatiwada AP, Gyawali S, Shankar PR, Palaian S. Overview, challenges and future prospects of drug information services in Nepal: a reflective commentary. J Multidiscip Healthc. 2020;13:287–295. https://doi.org/10.2147/JMDH.S238262
- Canadian Society of Hospital Pharmacists. Drug information services: guidelines. 3rd ed. Ottawa, Ontario: Canadian Society of Hospital Pharmacists; 2015.
- Manosalva MAN, Gutiérrez JJL, Cañas M. Drug information centers: an overview to the concept. Rev Colomb Cienc Quim Farm. 2016;45(2):243–245. https://doi.org/10.15446/rcciquifa.v45n2.59940
- Kumar BS, Samraksha M, Parvathi K. Overview of status and challenges of drug information services in India. Res Rev. 2022;5(4):1175–1183. https://doi.org/10.52845/CMRO/2022/5-4-2
- Chandola A, Ratnakar, Kandari S, Joshi Y. Status of drug information centre and services in India: an overview and challenges. Int J Pharm Sci Res. 2020;64(2):60–64. https://doi.org/10.47583/ijpsrr.2020.v64i02.010
- Chhetri A, Palaian S, Mishra P. Drug information services in Nepal: the changing perspectives. Kathmandu Univ Med J. 2008;6(1):117–121. https://pubmed.ncbi.nlm.nih.gov/18604128
- Almuqbil M, Alrojaie L, Alturki H, AlRuthia Y, Alrumaih A, Alothman F, Alsoghayer S, Alkofide H. The role of drug information centers to improve medication safety in Saudi Arabia - a study from healthcare professionals’ perspective. Saudi Pharm J. 2022;30(4):377–381. https://doi.org/10.1016/j.jsps.2022.01.024
- Kalra M, Pakhale SP, Khatak MS, Khatak S. Drug information centers - need of the hour. Int J Pharm Sci. 2011;1(1):69–76. https://www.indianjournals.com/ijor.aspx?target=ijor:ijps&volume=1&issue=1&article=012
- Khatiwada AP, Shakya S, Shrestha S. Paradigm shift of drug information centers during the COVID-19 pandemic. Drugs Ther Perspect. 2020;36:389–395. https://doi.org/10.1007/s40267-020-00757-3
- Santos JRBD. Regional drug information center disseminates educational materials related to the COVID-19 pandemic. Explor Res Clin Soc Pharm. 2021;4:100080. https://doi.org/10.1016/j.rcsop.2021.100080
- Gabay MP. The evolution of drug information centers and specialists. Hosp Pharm. 2017;52(7):452–453. https://doi.org/10.1177/0018578717724235
- Shankar PR, Mishra P, Subish P, Upadhyay DK. The drug information center at the Manipal teaching hospital—going beyond drug information. Ther Innov Regul Sci. 2007;41:761–768. https://doi.org/10.1177/009286150704100608
- Thireesha P, Mounika K, Adusumilli P, Harsha CS. An overview of drug information center – functions and challenges in India. Asian J Pharm Clin Res. 2020;13(5):11–15. https://doi.org/10.22159/ajpcr.2020.v13i5.37052
- Carlos V. Drug information centers in developing countries and the promotion of rational use of drugs: a viewpoint about challenges and perspectives. Int Pharm J. 2004;18:21–23.
- Khaliq A, Sayed SA. Drug and poison information centres: an emergent need for health care professionals in Pakistan. J Pak Med Assoc. 2016;66(6):639–643. https://pubmed.ncbi.nlm.nih.gov/27339562
- Joshi MP. Drug information service at teaching hospitals in developing countries. Indian J Pharmacol. 1998;30(1):1–5. https://www.ijp-online.com/article.asp?issn=0253-7613;year=1998;volume=30;issue=1;spage=1;epage=5;aulast=Joshi
- Paul TR, Rahman MA, Biswas M, Rashid M, Islam MAU. Practice of hospital pharmacy in Bangladesh: current perspective. Bangladesh Pharm J. 2015;17(2):187–192. https://doi.org/10.3329/bpj.v17i2.22339
- Batool M, Muzzamil U, Qureshi R. Assessment and utilization of a pharmacist-assisted drug and poison information centre in Pakistan. Int J Med Res Health Sci. 2019;8(4):117–123. https://www.ijmrhs.com/medical-research/assessment-and-utilization-of-a-pharmacistassisted-drug-and-poison-information-centre-in-pakistan.pdf
- University of Colombo. Department of pharmacology – service. University of Colombo. https://med.cmb.ac.lk/pharmac/services/. Published 2024. Accessed November 14, 2024.
- Ministry of Health Care and Nutrition. The national medicinal drug policy for Sri Lanka. Ministry of Health, Sri Lanka. https://www.health.gov.lk/wp-content/uploads/2022/10/17-National-Medicinal-Drug-Policy-for-Sri-Lanka-2005-compressed.pdf. Published 2005. Accessed November 14, 2024.
- Ashenef A, Reshid E, Yilma Z, Melaku T, Chane T. Assessment of the use and status of new drug information centers in a developing country, Ethiopia: the case of public university hospital drug information centers. Biomed Res Int. 2018;2018:3840976. https://doi.org/10.1155/2018/3840976
- Markind JE, Stachnik JM. European drug information centers. J Hum Lact. 1996;12(3):239–242. https://doi.org/10.1177/089033449601200324
- Gandra S, Alvarez-Uria G, Turner P, Joshi J, Limmathurotsakul D, Van Doorn HR. Antimicrobial resistance surveillance in low- and middle-income countries: progress and challenges in eight South Asian and Southeast Asian countries. Clin Microbiol Rev. 2020;33(3):e00048-19. https://doi.org/10.1128/CMR.00048-19
- Reppe LA, Spigset O, Schjøtt J. Drug information services today: current role and future perspectives in rational drug therapy. Clin Ther. 2016;38(2):414–421. https://doi.org/10.1016/j.clinthera.2015.12.019
- Perera T, Ranasinghe P, Perera U, Perera M, Wijesinghe P, Wijesekara M, Wijayabandara J. Knowledge of prescribed medication information among patients with limited English proficiency in Sri Lanka. BMC Res Notes. 2012;5:658. https://doi.org/10.1186/1756-0500-5-658
- Alahendra AMAAU, Perera OTS, Guruge ML, Anthony DK, Dasanayaka C, Wijekoon WMPDS. Perceived self-medication practices and associated factors among undergraduates in a non-state university. SLIIT J Humanit Sci. 2021;2(1):29–47. https://doi.org/10.4038/sjhs.v2i1.38
- Rashid M, Chhabra M, Kashyap A, Undela K, Gudi SK. Prevalence and predictors of self-medication practices in India: a systematic literature review and meta-analysis. Curr Clin Pharmacol. 2019;15(2):90–101. https://doi.org/10.2174/1574884714666191122103953
- Shankar P, Partha P, Shenoy N. Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: a questionnaire-based study. BMC Fam Pract. 2002;3:17. https://doi.org/10.1186/1471-2296-3-17
- Prinja S, Purohit N, Kaur N, Aggarwal AK, Gupta R, Bahuguna P, Kumar R, Kanavos P, Kumar R. The state of primary health care in South Asia. Lancet Glob Health. 2024;12(10):e1693–e1705. https://doi.org/10.1016/S2214-109X(24)00119-0
- Khan N, Chattopadhyay K, Leonardi-Bee J. Incidence, prevalence, risk factors and health consequences of polypharmacy in adults in South Asia: a systematic review protocol. JBI Evid Synth. 2019;17(11):2370–2377. https://doi.org/10.11124/JBISRIR-D-18-00001
- Delara M, Murray L, Jafari B, Bahji A, Goodarzi Z, Kirkham J, Chowdhury N, Seitz DP. Prevalence and factors associated with polypharmacy: a systematic review and meta-analysis. BMC Geriatr. 2022;22:601. https://doi.org/10.1186/s12877-022-03279-x
- Nualdaisri P, Corlett SA, Krska J. Provision and need for medicine information in Asia and Africa: a scoping review of the literature. Drug Saf. 2021;44:421–437. https://doi.org/10.1007/s40264-020-01038-8
- Bhosale UA. Evaluation of knowledge and awareness of patients about prescribed drugs and their package inserts: a cross-sectional study. Asian J Pharm. 2016;10(2):S96–S99. https://www.asiapharmaceutics.info/index.php/ajp/article/view/1048
- Rahim N, Rafiq K. Judgement of pharmaceutical package inserts available in Pakistan from local and multinational companies. Asian J Pharm Health Sci. 2013;3(1):597–600. https://www.ajphs.com/index.php?option=com_content&view=article&id=211
- Arsalan A, Qureshi S, Alam M, Ahmed S, Jabeen S, Masroor M. Errors in patients’ information leaflets of marketed medicines in Pakistan. J Appl Pharm Sci. 2015;5(5):068–074. https://doi.org/10.7324/JAPS.2015.50513
- Saheeha MSS, Piumanthi MHS, Perera SP, Samaranayake NR, Fernando GH. Quality of medicine information in product information leaflets: a retrospective audit. Ther Innov Regul Sci. 2018;52(5):656–660. https://doi.org/10.1177/2168479017753128
- Islam MS, Farah S. Availability and characteristics of information on drug-drug interactions in the drug package inserts: an experience from Bangladesh. Internet J Health. 2007;6:9. https://ispub.com/IJH/6/2/10854
- Patel S, Ganguly B. Audit of patient information leaflets available with topical medicines for patient use. Int J Pharm Res. 2014;6:50–55. https://ijpronline.com/index.php/IJPR/article/view/1626
- Alam K, Shah AK, Ojha P, Palaian S, Shankar PR. Evaluation of drug promotional materials in a hospital setting in Nepal. South Med Rev. 2009;2(1):2–6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3471187/
- Khan MAA, Hamid S, Babar ZUD. Pharmacovigilance practices in South Asian Association for regional cooperation countries: the need for collaboration. J Pharm Health Serv Res. 2022;13(4):378–386. https://doi.org/10.1093/jphsr/rmac046
- Ismail M, Iqbal Z, Khattak MB, Javaid A, Khan MI, Khan TM, Asim SM. Potential drug–drug interactions in internal medicine wards in hospital setting in Pakistan. Int J Clin Pharm. 2013;35:455–462. https://doi.org/10.1007/s11096-013-9764-1
- Khan MAA, Hamid S, Ur-Rehman T, Babar ZUD. Assessment of the current state of pharmacovigilance system in Pakistan using indicator-based assessment tool. Front Pharmacol. 2022;12:789103. https://doi.org/10.3389/fphar.2021.789103
- Khan J, Karatas Y, Khan Z. Self-medication in Pakistan: urgent need for medical education and policy implementation. Pak J Med Dent. 2021;10(4):104–105. https://doi.org/10.36283/PJMD10-4/018
- Navaratinaraja TS, Kumanan T, Siraj S, Sreeharan N. Potential drug–drug interactions among hospitalised elderly patients in northern Sri Lanka, a lower middle-income country: a retrospective analysis. Drugs Real World Outcomes. 2022;10:83–95. https://doi.org/10.1007/s40801-022-00333-3
- Chauhan N, Moin S, Pandey A, Mittal A, Bajaj U. Indian aspects of drug information resources and impact of drug information centre on community. J Adv Pharm Technol Res. 2013;4(2):84–93. https://doi.org/10.4103/2231-4040.111524
- Sakeena MHF, Bennett AA, McLachlan AJ. The need to strengthen the role of the pharmacist in Sri Lanka: perspectives. Pharmacy. 2019;7(2):54. https://doi.org/10.3390/pharmacy7020054
- Shankpal A, Yogita YV, Chinmayee R, Reddy S, Lakshmi PK. Implementation of drug information services in a tertiary care hospital: patients’ and physicians’ perception. Int J Pharm Investig. 2023;14(1):62–67. https://doi.org/10.5530/ijpi.14.1.9
- Peter AV, Murali A, Tomy T, Londhe SP. Assessment and utilization of drug information services and creating awareness for enhanced utilization of drug information centre in a tertiary care teaching hospital. Asian J Pharm Clin Res. 2017;10(5):270–274. https://doi.org/10.22159/ajpcr.2017.v10i5.17180
- Mudigubba MK, Sowmya B, Dinesh R, Rajashekar V, Yogananda R. Evaluation of performance of drug information center providing quality of information services to healthcare professionals in a tertiary care teaching hospital of South India. Innov Pharm Pharmacother. 2013;1(2):81–90. https://www.innovationalpublishers.com/Content/uploads/PDF/1520689259_IPP%20Vol%201%20Issue%202%2081-90.pdf
- Rao P, George B. Assessment and evaluation of drug information services provided in a South Indian teaching hospital. Indian J Pharmacol. 2005;37(5):315–319. https://doi.org/10.4103/0253-7613.16856
- Rajanandh MG, Varghese R, Ramasamy C. Assessment of drug information services in a South Indian tertiary care hospital in Kanchipuram district. Int J Pharm Pharm Sci. 2011;3(3):273–276. https://www.ijpps.com/index.php/IJPPS/article/view/737
- Kumar SV, Chakilam V. Quality of services provided by the drug information centre of the pharmacy practice department in a tertiary care teaching hospital at Warangal District: Andhra Pradesh, India. Indian J Hosp Pharm. 2012;49:151–156. https://www.indianjournals.com/ijor.aspx?target=ijor:ijhp&volume=49&issue=4&article=005
- Nibu P, Ramesh M, Parthasarathi G. Review of a drug information service in an Indian teaching hospital. Aust J Hosp Pharm. 2001;31(2):144–145. https://doi.org/10.1002/jppr2001312144
- Palaian S, Mishra P, Shankar P, Bista D, Pawar B. Contribution of the regional drug information center towards drug safety. J Nepal Med Assoc. 2006;45(161):216–218. https://pubmed.ncbi.nlm.nih.gov/17160096
- Pathak N, Rasaili A, Barma S, Nepal B, Nepal S, Thapa S, Khanal S, Subedi M, Adhikari S. Establishment of a drug information unit and pharmacovigilance cell in a provincial hospital of Nepal: implementation of the 2015 hospital pharmacy service guidelines. Hosp Pharm. 2025:00185787241306689. https://doi.org/10.1177/00185787241306689
- Innes AJ, Bramley DM, Wills S. The impact of UK medicines information services on patient care, clinical outcomes and medicines safety: an evaluation of healthcare professionals’ opinions. Eur J Hosp Pharm. 2014;21(4):222–228. https://doi.org/10.1136/ejhpharm-2014-000462
- Ali A, Yusoff SM, Joffry SM, Wahab MS. Drug information service awareness program and its impact on characteristics of inquiries at DIS unit in Malaysian public hospital. Arch Pharm Pract. 2013;4(1):9–14. https://doi.org/10.4103/2045-080X.112982
- Tumwikirize AW, Ogwal-Okeng JW, Vernby A, Anokbonggo WW, Gustafsson LL, Lundborg CS. Use of a pilot drug information centre. Afr Health Sci. 2011;11(3):493–498. https://pubmed.ncbi.nlm.nih.gov/22275941
- Wen MM, Aref H, Abozaid A, Kandil NH, Elsobky YH. Quality evaluation and survey of the essential need for drug information centers. Int J Pharm Pharm Sci. 2016;8(11):137–143. https://doi.org/10.22159/ijpps.2016v8i11.14085