
| Review | Open Access |
|---|
Optimizing Surgical Prophylaxis: An Audit of Antibiotic Use and Guideline Adherence in a Tertiary Care Hospital with Focus on Antimicrobial Stewardship |
 |
|---|
![]() Junaid Naeem1,2, Sajid Khan Sadozai1*, Saeed Ahmad Khan1, Syed Majid Shah1, Sajid Hussain1, Majid khan Sadozai3, Farina Kanwal4, and Naveed Safdar5
Junaid Naeem1,2, Sajid Khan Sadozai1*, Saeed Ahmad Khan1, Syed Majid Shah1, Sajid Hussain1, Majid khan Sadozai3, Farina Kanwal4, and Naveed Safdar5
1Department of Pharmacy, Kohat University of Science and Technology, Kohat, Pakistan
2Department of Pharmacy, PAF Hospital, Islamabad, Pakistan
3Department of Pharmacy, Abasyn University, Peshawar, Pakistan
4PCSIR Laboratories Complex, Peshawar, Pakistan
5Department of Pharmacology, Pak International Medical College Peshawar, Pakistan
Inappropriate antibiotic use, particularly in surgical prophylaxis, contributes to increasing antibiotic resistance and surgical site infections (SSIs). This study aimed to evaluate pre- and post-operative antibiotic prescribing practices and compliance with surgical prophylaxis guidelines in a tertiary care hospital, identifying areas for antimicrobial stewardship (AMS) intervention. A prospective study was conducted, collecting data on 250 surgical patients. After excluding 6 patients based on pre-defined criteria, data from 244 patients was analyzed using SPSS 20.0. The audit assessed patient demographics, pre- and post-operative antibiotic regimens, duration of antibiotic administration, and incidence of SSIs. Analysis revealed widespread use of broad-spectrum antibiotics for surgical prophylaxis, often deviating from established guidelines. Intravenous (IV) antibiotics were commonly administered for extended durations (24–72 hours) post-operatively. A significant proportion of patients (n=167) received oral antibiotics upon discharge to complete a 5-day course. The SSI incidence rate was 2.0%, with all infections occurring in patients who underwent open surgical procedures (laparotomies). Staphylococcus aureus was the most frequently isolated organism (including methicillin-resistant strains), followed by Klebsiella pneumoniae and Escherichia coli. Most isolates exhibited multidrug resistance, although they remained sensitive to antibiotics, such as vancomycin, linezolid, meropenem, and colistin. Management was guided by culture and sensitivity in most cases; however, one instance of irrational antibiotic use was observed. These findings emphasize the role of surgical type, duration, and appropriate microbial management in SSI prevention. In conclusion, the study highlighted significant deviations from surgical prophylaxis guidelines and irrational antibiotic use. The presence of multidrug-resistant organisms (MDROs) and inappropriate antibiotic selection further stressed the urgent need for targeted AMS interventions. These should include the development and implementation of hospital-specific prophylaxis protocols aligned with the best national or international practices. Ongoing monitoring is needed to assess AMS effectiveness.
1. INTRODUCTION
Antimicrobial resistance (AMR) is a rapidly escalating global health crisis, projected to cause up to 10 million deaths annually by 2050 if unaddressed [1, 2]. AMR is a serious concern for healthcare systems worldwide, with infections caused by multidrug-resistant organisms (MDROs) becoming more prevalent. Recognized as an emerging global health crisis, a major driver of AMR is the inappropriate and excessive use of antibiotics, particularly in surgical settings, where broad-spectrum antibiotics are often used indiscriminately to manage SSIs [3, 4]. This practice contributes to increased complications, prolonged hospital stays, higher mortality, and greater healthcare costs. In this context, surgical antibiotic prophylaxis (SAP) involves the administration of antibiotics before surgical incision to prevent surgical site infections (SSIs) which plays a vital role in infection control [4]. The rising threat of antimicrobial resistance in surgical settings as well as the integration of well-structured antimicrobial stewardship (AMS) initiatives within surgical departments play a pivotal role in ensuring appropriate antibiotic prescribing. This curbs resistance trends and supports better clinical outcomes [5].
However, SAP is frequently misapplied, with common issues including prolonged administration beyond recommended timeframes, inappropriate antibiotic selection, and use in clean procedures without indication [6]. Such misuse significantly contributes to the overuse of antibiotics and the growing problem of antimicrobial resistance. These irrational practices often stem from poor adherence to clinical guidelines, limited access to evidence-based protocols, insufficient training, and a prevailing culture of defensive medicine driven by fear of postoperative infections. The prevailing culture of defensive medicine rooted in an excessive fear of postoperative infections also plays a significant role, frequently prompting the unwarranted use of broad-spectrum antibiotics as a precaution, even when clinical indications are absent [7]. Addressing these challenges demands a multifaceted approach incorporating continuous medical education, adherence to AMS principles, and fostering a culture of evidence-based prescribing within surgical teams.
The impact of AMR extends far beyond individual patient outcomes, posing significant challenges to the broader healthcare system. The emergence and proliferation of MDROs complicate the management of infections, often requiring the use of broader-spectrum and more costly antibiotics, and are associated with higher rates of morbidity and mortality [8]. Moreover, AMR can undermine surgical outcomes by rendering postoperative infections more difficult to treat, thereby increasing the incidence of SSIs, the need for re-operations, and the duration of hospital stays [9].
In response to the growing threat of antimicrobial resistance, various national and international health authorities have advocated for the widespread implementation of AMS programs across all levels of healthcare, with particular emphasis on their integration within surgical departments [5, 10]. The AMS programs are designed to optimize antibiotic use by encouraging compliance with evidence-based guidelines, delivering targeted education and training for healthcare professionals as well as implementing systematic strategies to monitor and enhance prescribing practices. While data from high-income countries guide most SAP recommendations, there is limited evidence on SAP adherence and AMS implementation in low- and middle-income countries, such as Pakistan. This underscores the importance of context-specific audits. In Pakistan, particularly in tertiary care hospitals, antibiotic prescribing often relies on clinical judgment rather than guideline adherence, with limited AMS oversight and overcautious prescribing habits common among surgical teams [7, 11]. This study aimed to evaluate antibiotic utilization patterns in the surgical department, both in the preoperative and postoperative phases at a tertiary care hospital located in Khyber Pakhtunkhwa (KPK), Pakistan.
2. METHODOLOGY
2.1 Study DesignThis prospective cross-sectional study was conducted to assess the prevalence of SSIs in relation to the existing hospital protocol for postoperative prophylactic antibiotic use. The study took place at Rehman Medical Institute, a tertiary care teaching hospital located in Phase-V, Hayatabad, Peshawar, Khyber Pakhtunkhwa (KPK), Pakistan. Data was collected over a six-month period, from September 1, 2023 to February 29, 2024. A sample size of 250 was selected based on feasibility and available resources for prospective data collection over six months, providing sufficient power to detect prescribing trends and infection rates. Patients undergoing abdominal procedures were screened, with 244 meeting the predefined inclusion criteria and being included in the final analysis. Six patients were omitted since they were ineligible according to the exclusion criteria.
2.2. Inclusion and Exclusion CriteriaThe study included male and female patients between the ages of 12 and 65 years who underwent either elective or emergency abdominal surgeries. Immunocompromised persons, patients with cancer at any stage (these groups were excluded to reduce confounding, as their altered immune status may independently increase infection risk and warrant different antibiotic protocols), pregnant women, and patients who died soon after surgery were all excluded.
2.3. Data CollectionData was collected prospectively by daily visits to surgical wards using a structured case proforma. The proforma collected important pre- and post-operative clinical data, such as age, gender, admission date, pre-operative hospital stays, medical and medication history, as well as comorbidities and the type of surgery (elective or emergency).
Preoperative antibiotic data comprised the prophylactic agent's name, dose, time relative to surgical incision, and duration of antibiotic usage. During their hospitalization, patients were examined daily for signs and symptoms of SSIs, such as redness, swelling, and localized pain. Following discharge, patients were followed for up to 30 days via telephone calls or outpatient visits, in accordance with the Centers for Disease Control and Prevention's (CDC) definition of SSIs.
2.4. Ethical ConsiderationsThe study protocol was approved by the Institutional Ethical Review Committee with the reference number KUST/Ethical Committee/1402. All procedures were carried out in compliance with the International Conference on Harmonization (ICH) 2012 criteria for Good Clinical Practice (GCP), which ensured patient confidentiality and privacy. Additionally, the hospital protocols and ethical guidelines of Rehman Medical Complex Peshawar were strictly followed throughout the study.
2.5. Statistical AnalysisThe descriptive statistical analysis was carried out using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). Categorical variables were reported as frequencies and percentages, whilst continuous variables were represented as means and standard deviations. A p-value <0.05 indicated statistical significance.
2.6. Study SummaryThe study was carried out in different phases mentioned as follows:
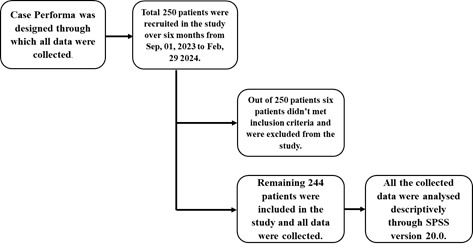
Figure 1. Overview of Study Design and Patient Recruitment Process
This schematic depicts the study's methodological structure, which includes patient selection and data collection. A structured case proforma was used to collect clinical data from 250 patients undergoing abdominal surgery over a six-month period (September 1, 2023–February 29, 2024). After removing 6 patients based on predetermined criteria, data from 244 patients was analyzed using descriptive statistics in SPSS version 20.0.
3. RESULTS AND DISCUSSION
3.1. Patient DemographicsA total of 250 patients were initially enrolled in the study. Following the application of inclusion and exclusion criteria, 244 patients were included in the final analysis, while six patients were excluded due to non-eligibility with females accounting for 145 (59.4%) and males for 99 (40.6%). Although, the incidence of SSIs was observed to be slightly higher among male patients as compared to females, the difference was not statistically significant. This finding aligns with a multicenter study conducted between 2015 and 2018, which reported no significant correlation between patient gender and the risk of SSIs following abdominal surgeries [12]. Similarly, another study suggested that while male patients may show a relatively higher incidence of SSIs post-abdominal surgery, further investigation is necessary to establish gender as a definitive risk factor [13].
3.2. Age and Risk of Surgical Site Infections (SSIs)Age is a well-recognized factor influencing susceptibility to postoperative infections. In this study, the average patient age was in the late 40s, with elderly patients demonstrating a higher tendency towards developing SSIs. This observation is supported by previous literature, which indicates that advancing age, particularly beyond 60 years, is associated with increased SSIs risk due to immunosuppressed and comorbid conditions [14]. Another study similarly concluded that the likelihood of developing SSIs rises progressively with age. This highlights the importance of age-based risk stratification in surgical care planning [15].
Table 1. Gender-wise Distribution of Patients Included in the Study (n=244)
|
Gender |
Frequency |
Percentages |
|---|---|---|
|
Males |
99 |
40.6 |
|
Females |
145 |
59.4 |
|
Total |
244 |
100.0 |
Comorbidities were evaluated to assess their potential association with the development of SSIs. Among the 244 patients included in the study, the majority (n = 134, 54.9%) had no comorbid conditions. The remaining 110 patients (45.1%) presented with one or more of the following comorbidities.
Although, patients with hypertension and/or diabetes mellitus were observed among those who developed SSIs, no statistically significant association was found between these comorbidities and SSI incidence (p = 0.317, chi-square test). These findings are in contrast with previous studies, which identified hypertension and diabetes as significant risk factors for SSI development [16]. The lack of statistical significance in the current study may be attributed to sample size or clinical management protocols that minimize infection risk in comorbid patients.
Table 2. Prevalence of Comorbidities among Patients (N = 244)
|
Comorbidities |
Frequency |
Percentages |
|---|---|---|
|
Hypertension |
57 |
23.4 |
|
Diabetes Mellitus |
11 |
4.5 |
|
Hypertension + Diabetes Mellitus |
42 |
17.2 |
|
No comorbidities |
134 |
54.9 |
|
Total |
244 |
100.0 |
The duration of hospital stays before and after surgery was documented to assess its potential relationship with the incidence of SSIs and the associated healthcare costs. Among the 244 patients included in the study, the majority (n = 226; 92.6%) were admitted one day prior to their surgical procedure. A smaller proportion of patients underwent surgery two days after admission (n = 8; 3.3%), while 10 patients (4.1%) had surgery performed on the same day as their admission.
Table 3. Distribution of Patients by Number of Pre-operative Hospitalization Days
|
No. of Pre-operative Days |
Frequency |
Percentages |
|---|---|---|
|
0 |
10 |
4.1 |
|
1 |
226 |
92.6 |
|
2 |
8 |
3.3 |
|
Total |
244 |
100.0 |
Post-operatively, most patients (n = 185; 75.8%) were discharged within 24 hours of surgery. Forty-five patients (18.4%) were discharged after 48 hours, while 10 patients (4.1%) remained hospitalized for 3 days post-surgery. Only 4 patients (1.6%) required a hospital stay of 4 days following the procedure. Although, a trend was observed toward longer post-operative stays among patients who developed SSIs, statistical analysis showed no significant association between length of hospital stay and SSI occurrence (p = 0.091). Nonetheless, prolonged hospitalization is widely recognized as a contributor to increased risk of healthcare-associated infections, including SSIs, and represents a substantial economic burden. These findings underscore the importance of timely surgical care and effective infection prevention strategies to reduce unnecessary hospital stays and healthcare costs.
Table 4. Distribution of Patients by Number of Post-operative Hospitalization Days
|
No. of Post-operative Days |
Frequency |
Percentages |
|---|---|---|
|
1 |
185 |
75.8 |
|
2 |
45 |
18.4 |
|
3 |
10 |
4.1 |
|
4 |
4 |
1.6 |
|
Total |
244 |
100.0 |
SAP was administered to patients undergoing surgical procedures in order to prevent the development of SSIs. Out of the 244 patients included in the study, 236 (96.7%) received prophylactic antibiotics, while 8 patients (3.3%) did not receive any preoperative antibiotic coverage due to various clinical considerations.
Among the patients who received prophylaxis, a range of antibiotics was used. Intravenous (IV) meropenem 1 g was the most frequently administered antibiotic, prescribed to 98 patients (40.2%), followed by IV ceftriaxone 1 g, which was given to 42 patients (17.2%). Ceftriaxone (IV) 2 g was administered in 4 patients (1.6%), while 27 patients (11.1%) received IV cefoperazone/sulbactam 2 g. Other regimens included IV meropenem 2 g (n = 5; 2.0%), IV amoxicillin/clavulanate 1.2 g (n = 3; 1.2%), and IV metronidazole 500 mg alone (n = 8; 3.3%). Combination regimens were also noted, including IV meropenem 1 g plus IV metronidazole 500 mg (n = 24; 9.8%), IV cefoperazone/sulbactam 1 g plus IV metronidazole 500 mg (n = 1; 0.4%), and IV cefoperazone/sulbactam 2 g plus IV metronidazole 500 mg (n = 14; 5.7%).
Current guidelines issued by the World Health Organization (WHO) and the American Society of Health-System Pharmacists (ASHP) recommend administering a single dose of prophylactic antibiotic within 60 minutes prior to surgical incision. When used appropriately, prophylactic antibiotics have been shown to significantly reduce the risk of SSIs. Numerous studies support this strategy, highlighting that the timely and appropriate use of surgical SAP is associated with substantially lower SSI rates as compared to patients who receive antibiotics only postoperatively or not at all [17, 18].
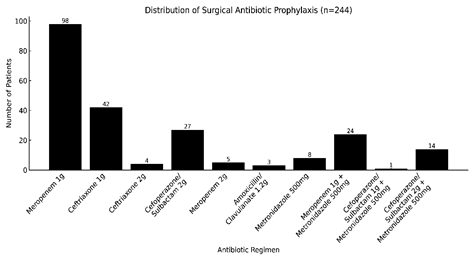
Figure 2. Frequency of Various Antibiotic Regimens Used for Surgical Prophylaxis in the Study Population (n = 244)
This bar chart depicts the frequency of SAP treatments provided to 244 patients. Meropenem 1g was the most popular antibiotic (n=98), followed by Ceftriaxone 1g (n=42) and cefoperazone/sulbactam 2g (n=27). Meropenem plus Metronidazole (n=24) and other regimen were used less frequently. The widespread use of broad-spectrum antibiotics indicates a significant emphasis on broad preventive coverage, which is likely impacted by local AMR patterns and infection control policies. These findings emphasize crucial aspects of antibiotic management in surgical settings.
3.6. Surgical Procedures PerformedDuring the six-month study period, a total of 244 abdominal surgical procedures were performed. The majority of procedures were carried out using laparoscopic techniques. Laparoscopic cholecystectomy was the most frequently performed procedure, accounting for 119 cases (48.8%), followed by hernioplasty in 73 patients (29.9%), laparotomy in 29 patients (11.9%), appendectomy in 20 patients (8.2%), hemorrhoidectomy in 8 patients (3.3%), and gastrojejunostomy in 1 patient (0.4%).
The preference for laparoscopic procedures among surgeons has grown considerably, supported by various studies indicating a lower risk of SSIs associated with minimally invasive techniques. The adoption of laparoscopic surgery has significantly increased since the 1990s [19, 20]. A multicenter study involving 25 hospitals reported that the incidence of SSIs following laparoscopic cholecystectomy was 1.08%, compared to 4.41% for open cholecystectomy procedures [21].
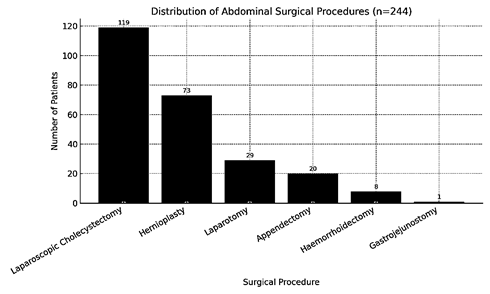
Figure 3. Distribution of Abdominal Surgical Procedures among Patients (n = 244)
This bar chart depicts the frequency of abdominal surgeries performed on 244 people. The most commonly performed procedure was laparoscopic cholecystectomy (n=119), followed by hernioplasty (n=73) and laparotomy (n=29). Less common operations were appendectomy (n=20), hemorrhoidectomy (n=8), and gastrojejunostomy (n=1). The popularity of minimally invasive techniques, such as laparoscopic cholecystectomy reflects modern surgical preferences to reduce complications and improve recovery. These data provide insights into surgical case mix and service consumption at the research site.
3.7. Duration of Surgical ProcedureIn this study, the majority of surgical procedures were completed within 80 minutes, with a mean operative time of 66.56 minutes. Only a few surgeries extended beyond 2 hours, and no procedure exceeded 3 hours in duration. The length of a surgical procedure is a critical factor influencing the risk of SSIs. Procedures with extended durations are more likely to increase the patient's exposure to environmental contaminants and compromise aseptic conditions, thereby increasing the risk of SSI.
A systematic review has reported that the likelihood of developing an SSI increases proportionally with the duration of surgery. Specifically, the risk increases by approximately 13% for every additional 15 minutes, 17% for every 30 minutes, and up to 37% for every 60 minutes beyond the standard operative time [22]. In the current study, the relatively shorter durations of surgery may have contributed to the lower incidence of SSI observed.
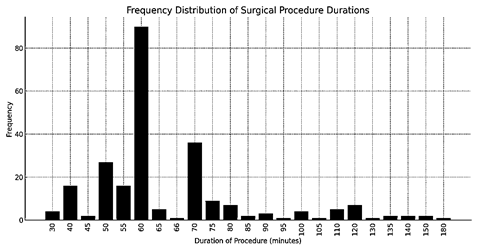
Figure 4. Distribution of Surgical Procedure Duration among Patients Undergoing Surgery (n = 228)
This bar graph depicts the distribution of surgical procedures by duration. Most procedures (36.88%) were finished in less than 60 minutes, with notable frequencies of 50 (11.8%) and 70 minutes (14.75%). Procedures longer than 75 minutes were less prevalent. These findings suggest efficient surgical scheduling and are consistent with infection control efforts, as shorter operating times are associated with lower SSI risk.
3.8. Post-operative AntibioticsAll 244 patients in the study received post-operative IV antibiotics, regardless of whether they had received prophylactic antibiotics prior to surgery. The most commonly prescribed regimens included cefoperazone/sulbactam 1g for two doses (n = 59), meropenem 1g for two doses (n = 52), and ceftriaxone 1g for two doses (n = 38). Other combinations included cefoperazone/sulbactam 1g for two doses with metronidazole 500 mg for two doses (n = 22), cefoperazone/sulbactam 1g for four doses (n = 17), meropenem 1g for four doses (n = 15), and meropenem 1g for two doses combined with metronidazole 500 mg for two doses (n = 10). A smaller number of patients received ceftriaxone 1g for two doses with metronidazole 500 mg for two doses (n = 4), meropenem 1g for six doses with metronidazole 500 mg for nine doses (n = 4), and amoxicillin/clavulanate 600 mg for two doses (n = 4). According to WHO and other international guidelines, antibiotic prophylaxis should be limited to a single dose or continued for no more than 24 hours post-operatively, except in specific cases, such as cardiac surgeries where a 48-hour course may be justified. The use of antibiotics beyond this period is not associated with a reduction in SSIs and may contribute to adverse effects, increased healthcare costs, and the development of antimicrobial resistance. Despite guidelines advising discontinuation within 24 hours post-operatively, all patients (100%) received antibiotics beyond this duration, underscoring a critical AMS gap. This practice represents a significant deviation from established guidelines and highlights a potential area for intervention to reduce unnecessary antibiotic use and its associated risks.
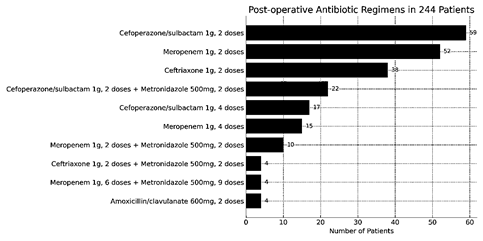
Figure 5. The Frequency of each Post-operative Antibiotic Regimen Administered to 244 Patients
This bar chart depicts the frequency of post-operative antibiotic regimens for 244 individuals. Cefoperazone/sulbactam 1g (2 doses) was the most often prescribed medication (n=59), followed by meropenem 1g (2 doses, n=52) and ceftriaxone 1g (2 doses, n=38). Combination therapy, such as cefoperazone/sulbactam with metronidazole and meropenem with metronidazole, were less popular. The distribution reflects efforts to ensure adequate coverage while adhering to AMS standards specific to surgical risk and local practices.
3.9. Discharge Antibiotic UseOf the 244 patients included in the study, 164 (67.2%) were prescribed oral antibiotics at the time of discharge, typically for a duration of five days. The most commonly prescribed oral antibiotics included moxifloxacin 400 mg once daily (n = 62) and a combination of ciprofloxacin 500 mg twice daily with metronidazole 400 mg three times daily (n = 52). Other discharge regimens included ciprofloxacin 500 mg twice daily (n = 25), linezolid 600 mg twice daily for 10 days (n = 9), and amoxicillin/clavulanate 625 mg three times daily (n = 5). Less frequently prescribed combinations included linezolid 600 mg twice daily for 10 days with metronidazole 400 mg three times daily (n = 4), metronidazole 400 mg three times daily alone (n = 3), moxifloxacin 400 mg once daily with metronidazole 400 mg three times daily (n = 2), and cefixime 400 mg once daily (n = 2). Additionally, 4 patients were discharged on IV antibiotics: two received meropenem 1 g twice daily for 3 days combined with metronidazole 400 mg three times daily for 5 days, and two received cefoperazone/sulbactam 1 g twice daily for 3 days along with metronidazole 400 mg three times daily for 5 days.
The 20th century marked a significant advancement in medicine with the introduction of antibiotics; however, antibiotic resistance has since emerged as a global public health crisis. A point prevalence survey conducted in surgical departments in Italy from 2008 to 2016 revealed an increase in prophylactic antibiotic use from 6.1% to 24.2% [23]. The overuse and misuse of antibiotics, especially in surgical care, is a key driver of resistance and associated healthcare costs. In this study, more than half of the patients were discharged with antibiotics in the absence of clinical indications or adherence to established guidelines. This reflects a pattern of irrational prescribing, which not only fails to provide additional benefit but also contributes to the growing threat of AMR and unnecessary financial burden on patients and healthcare systems.
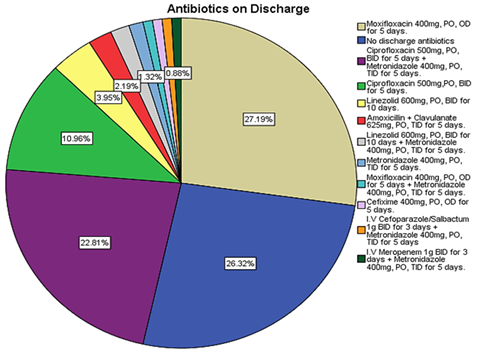
Figure 6. Distribution of antibiotic regimens among the 164 patients who received antibiotics upon discharge.
This pie chart depicts the distribution of antibiotics provided upon discharge. Moxifloxacin 400 mg once daily for 5 days was the most commonly used medication (27.19%), followed by ciprofloxacin plus metronidazole (26.32%) and ciprofloxacin alone (22.81%). Notably, 10.96% of patients were released without antimicrobials. Less prevalent regimens included linezolid, amoxicillin-clavulanate, and a transition from IV to oral antibiotics. These patterns reflect the various clinical decisions made depending on infection risk, surgical outcomes, and patient-specific characteristics.
3.10. Prevalence of Surgical Site Infections (SSIs)SSIs were observed in 5 out of 244 patients, representing a prevalence rate of 2.0%. All SSIs identified in the study were superficial and confirmed through positive pus cultures obtained from the surgical site. According to a WHO report, the incidence of SSIs in LMICs ranges from 1.2% to 23.6% [23]. The SSI rate observed in this study is consistent with findings from similar studies and reflects the effectiveness of preventive measures implemented during the pri-operative period. One notable factor contributing to the low SSI rate was the high proportion of laparoscopic procedures, which are associated with a significantly lower risk of infection compared to open surgeries. In this study, all SSIs occurred in patients who underwent open surgical procedures, specifically laparotomies. This aligns with the results of a large retrospective study involving 6,000 patients, which demonstrated that the incidence of SSIs was substantially lower in laparoscopic surgeries (2.0%) compared to open surgeries (10.0%) [24]. Another contributing factor to the low SSI rate was the short duration of surgical procedures; all operations in this study were completed within 3 hours. Previous studies demonstrated that the risk of SSIs increases progressively with longer operative durations, rising by approximately 13%, 17%, and 37% with each additional 15, 30, and 60 minutes of surgery, respectively [25]. These findings highlight the significance of adopting minimally invasive surgical techniques and maintaining efficient operative timing as key strategies to reduce the risk of SSIs.
3.11. Microorganisms IdentifiedPus samples were collected from patients with SSIs and submitted for microbiological analysis to identify the causative pathogens. Laboratory cultures revealed Staphylococcus aureus in two samples, while Klebsiella pneumoniae was isolated from one. Another sample demonstrated mixed growth of S. aureus and Escherichia coli, and one culture showed no microbial growth. Among the identified organisms, S. aureus was the most frequently isolated pathogen. As a common component of the normal skin flora, S. aureus is frequently associated with both superficial and deep wound infections, particularly when introduced into a surgical site.
These findings align with the existing literature that identifies S. aureus as a primary causative agent of SSIs. A study conducted at a tertiary care hospital in India similarly reported S. aureus as the most commonly isolated pathogen, followed by E. coli and Pseudomonas aeruginosa [26–28]. These results underscore the need for targeted AMS interventions and rigorous adherence to aseptic techniques to prevent infections caused by common skin flora and healthcare-associated pathogens..
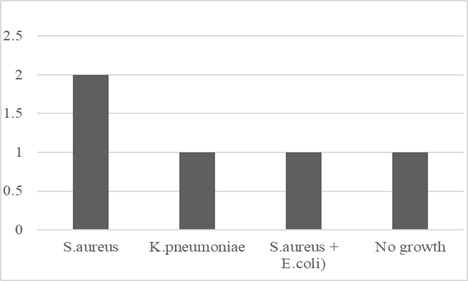
Figure 7. Distribution of Microorganisms Identified in SSIs
The bar chart illustrates the distribution of bacterial isolates obtained from wound cultures in patients with SSIs. S. aureus was the most frequently identified pathogen (n=2), followed by K. pneumoniae (n=1), and a mixed infection involving S. aureus and E. coli (n=1). One culture showed no microbial growth, which may be attributed to prior antibiotic administration or inadequate sample collection. These findings underscore the importance of microbiological identification in guiding targeted antibiotic therapy for SSIs..
3.12. Resistance Pattern of MicroorganismsA total of 3 distinct bacterial species were isolated from SSIs: S. aureus, E. coli, and K. pneumoniae. The S. aureus isolate was identified as MRSA and was susceptible to vancomycin and linezolid. E. coli demonstrated resistance to penicillin and cephalosporins but remained sensitive to meropenem, doxycycline, and minocycline. K. pneumoniae exhibited resistance to penicillin and first and second generation cephalosporins while retaining susceptibility to higher generation cephalosporins, aminoglycosides, meropenem, and colistin.
The detection of MDROs in this study represents a significant clinical concern, emphasizing the urgent need for a comprehensive strategy to combat antimicrobial resistance. Key measures include the prompt initiation of appropriate empirical therapy upon clinical suspicion of SSIs, timely collection of microbiological cultures, and the prudent de-escalation of antibiotic therapy based on culture results. These findings reinforce the importance of strict adherence to established prophylactic antibiotic guidelines and the implementation of robust infection prevention and control protocols. This aligns with previous studies, including one conducted at a tertiary care hospital, which reported methicillin resistance in 90% of S. aureus related SSIs [22].
3.13. Management of Surgical Site Infections (SSIs)All patients diagnosed with SSIs received antibiotic therapy tailored to culture and sensitivity findings. In one case, K. pneumoniae demonstrated susceptibility to cefoperazone/sulbactam, which was administered intravenously at a dose of 2.0 g every 12 hours for five days. In 2 cases involving S. aureus, patients were treated with oral linezolid 600 mg every 12 hours. One patient had a mixed culture of S. aureus and E. coli and was prescribed moxifloxacin 400 mg orally for 5 days. However, sensitivity testing did not support this therapy and it was not regarded active against the isolated pathogens.
Three of the 4 culture-positive patients were treated with antibiotics relevant to their culture and sensitivity results. One patient was given an antibiotic regimen that did not match the sensitivity pattern of the identified pathogens, indicating irrational antibiotic use.
SSIs are among the most prevalent surgical complications, contributing considerably to increased morbidity, longer hospitalization, and healthcare expenses [29]. Proper SSI management entails rapid diagnosis, microbiological identification, and an appropriate administration of antibiotics based on culture and sensitivity tests. In the current investigation, 4 patients had SSIs and their therapy indicated both reasonable and irrational antibiotic utilization strategies [30].
Currently, there is no formal AMS program or audit-feedback mechanism in place at the study site, limiting the capacity to enforce or monitor rational antibiotic use. Antibiotic stewardship programs stress the significance of adopting targeted therapy based on microbiological data to decrease resistance and adverse medication responses [31]. A 2022 multicenter study in South Asia underlined that empirical broad-spectrum antibiotics should be avoided until critically vital, and that de-escalation based on sensitivity testing should be followed regularly [32]. Another study from Pakistan emphasized that misuse and improper selection of antibiotics after surgery contribute considerably to antibiotic resistance, especially in low- and middle-income countries where surveillance is poor [33].
Furthermore, observing evidence-based guidelines from the WHO and the CDC is critical to implementing effective SSI therapy. These guidelines promote culture-directed therapy and oppose prolonged post-operative antibiotic usage, unless clinically required [34, 35].
The findings of current study showed that moxifloxacin was clearly overused, highlighting a serious flaw in current clinical prescribing guidelines. This trend emphasizes the critical need for ongoing medical education initiatives designed to improve physicians' understanding of sensible antibiotic usage. Furthermore, it highlighted the inadequate implementation of AMS procedures, which are critical for guiding clinicians toward evidence-based decisions in the management of SSIs.
In the local clinical context of Pakistan, the practice of defensive medicine is commonly observed. Surgeons often prescribe prolonged courses of antibiotics, influenced not only by limited microbiological support but also by concerns over medico-legal issues and patient expectations. These cultural norms and institutional gaps may help explain the continued pattern of inappropriate antibiotic use noted in the findings.
According to the findings, it is evident that excessive use of broad-spectrum antibiotics, without culture sensitivity data, may lead towards the emergence of resistant bacterial strains, hence limiting future treatment options. Resultantly, it is critical to implement strong antibiotic stewardship methods that not only monitor prescribing patterns but also ensure compliance with hospital or national norms.
To address developing antibiotic resistance and ensure optimal patient outcomes, healthcare providers must be trained and encouraged to properly evaluate microbiological culture and sensitivity results. This would allow for the selection of the most appropriate and focused antibiotic therapy, reducing unnecessary exposure to broad-spectrum medicines while keeping their efficacy in cases when they are actually needed.
3.14. ConclusionThe current study highlighted notable trends in the use of surgical antibiotic prophylaxis and post-operative care practices in a tertiary care hospital. While the preference for laparoscopic procedures is associated with a lower risk of SSIs, the widespread and prolonged use of post-operative antibiotics often exceeding 24 hours and lacking culture-guided justification raises serious concerns about AMS and the risk of promoting AMR. Although, most SSIs were managed based on microbial sensitivity, instances of irrational antibiotic use were observed. These findings underscore the urgent need to implement standardized, evidence-based protocols for surgical prophylaxis and SSI management. The study recommended implementing a mandatory AMS review for all discharge prescriptions, along with the integration of audit and feedback mechanisms into routine surgical workflows. Development and enforcement of hospital-specific SAP protocols, combined with regular training sessions for prescribers, should be prioritized to enhance compliance and optimized antibiotic use.
3.15. LimitationsThis study has several limitations. It was conducted at a single tertiary care hospital, limiting the generalizability of findings. The follow-up period was restricted to 30 days, potentially underreporting late-onset SSIs. The absence of a control group and detailed cost analysis limits assessment of the clinical and economic impact of antibiotic overuse. Microbiological data were only obtained from patients with SSIs, and the rationale behind prescribing practices was not explored.
CONFLICT OF INTEREST
The authors have no financial or non-financial conflict of interest in this manuscript.
DATA AVAILABILITY STATEMENT
Relevant data generated and analyzed during this study can be obtained from the corresponding author upon request. Access to certain portions of the dataset may be limited in order to maintain patient confidentiality and comply with institutional guidelines.
FUNDING DETAILS
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
- Kourbeti I, Aikaterini K, Michael S. Antibiotic stewardship in surgical departments. Antibiotics. 2024;13(4):329. https://doi.org/10.3390/antibiotics13040329
- Gautam S, Simranpreet K. Revolutionizing biomedicine: metal-organic frameworks combating multi-drug resistance. Mater Lett. 2024;354:135306. https://doi.org/10.1016/j.matlet.2023.135306
- Perez KK, Drake TC, Fuentes A, Gentry CN. Prevalence and characteristics of self-reported antibiotic allergies across a multi-hospital healthcare system. Open Forum Infect Dis. 2019;6(Suppl 2):S389–S390. https://doi.org/10.1093/ofid/ofz360.959
- Seah XFV. Impact of antimicrobial stewardship interventions on post-elective caesarean antibiotic prophylaxis and surgical site infections. Open Forum Infect Dis. 2020;7(Suppl 1):S53. https://doi.org/10.1093/ofid/ofaa439.114
- Hickman K, Nicolas F, Mandelin C, Shivanne B, Brandy R. Implementing a health-system-wide antibiotic stewardship program in ambulatory surgery centers. Antimicrob Steward Healthc Epidemiol. 2023;3(S2):s2–s27. https://doi.org/10.1017/ash.2023.250
- Giordano M, Lorena S, Maria P. Appropriateness of surgical antibiotic prophylaxis in pediatric patients in Italy. Infect Control Hosp Epidemiol. 2017;38(7):823–831. https://doi.org/10.1017/ice.2017.79
- Brink AJ, Messina AP, Feldman C, Richards GA, van den Bergh D. From guidelines to practice: a pharmacist-driven prospective audit and feedback improvement model for peri-operative antibiotic prophylaxis in 34 South African hospitals. J Antimicrob Chemother. 2017;72(4):1227–1234. https://doi.org/10.1093/jac/dkw523
- Sharma R, Dinesh L. Acinetobacter baumannii: a comprehensive review of global epidemiology, clinical implications, host interactions, mechanisms of antimicrobial resistance and mitigation strategies. Microb Pathog. 2025;204:107605. https://doi.org/10.1016/j.micpath.2025.107605
- Jerome JTJ, Arun K, Mauli C. Surgical management for distal phalanx osteomyelitis: a narrative review. J Clin Orthop Trauma. 2025;66:103021. https://doi.org/10.1016/j.jcot.2025.103021
- Simoni A, Laura S, Guillermo YJ, Christina BC, John DS. Current and emerging strategies to curb antibiotic-resistant urinary tract infections. Nat Rev Urol. 2024;21(12):1–16. https://doi.org/10.1038/s41585-024-00877-9
- Mzumara GW, Michael M, Pui-Ying IT. Protocols, policies and practices for antimicrobial stewardship in hospitalized patients in least-developed and low-income countries: a systematic review. Antimicrob Resist Infect Control. 2023;12(1):131. https://doi.org/10.1186/s13756-023-01335-8
- Zwicky SN, Severin G, Franziska T, et al. No impact of sex on surgical site infections in abdominal surgery: a multi-center study. Langenbecks Arch Surg. 2022;407(8):3763–3769. https://doi.org/10.1007/s00423-022-02691-6
- Iqbal S, Iftikhar M, Qureshi HU, Khan AG, Ullah S. Frequency of surgical site infection after appendicectomy. J Peoples Univ Med Health Sci Nawabshah. 2024;14(3):32–37. https://doi.org/10.46536/jpumhs/2024/14.03.532
- Bucataru A, Maria B, Alice EG, et al. Factors contributing to surgical site infections: a comprehensive systematic review of etiology and risk factors. Clin Pract. 2023;14(1):52–68. https://doi.org/10.3390/clinpract14010006
- Li H, Xufeng Z, Jie G. Extensive analysis of risk factors associated with surgical site infections post-cardiothoracic open surgery. Int Wound J. 2024;21(3):14842. https://doi.org/10.1111/iwj.14842
- Zhang L, Er-Nan L. Risk factors for surgical site infection following lumbar spinal surgery: a meta-analysis. Ther Clin Risk Manag. 2018;14:2161–2169. https://doi.org/10.2147/TCRM.S181477
- Chola B. Evaluation of the compliance of antibiotic prescribing with international clinical practice guidelines for surgical antibiotic prophylaxis at Intermediate Hospital Rundu, Namibia. University of Namibia; 2022.
- Hyland SJ. Perioperative antimicrobial stewardship and pharmacy’s role. Premier Inc; 2023. https://ce.pharmacy.premierinc.com/assets/ClientID_168/EventAssets/perioperative-abx-stewardship-hs-handout.pdf. Accessed January 15, 2025.
- Kelley WE Jr. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. JSLS. 2008;12(4):351–357. https://doi.org/10.4293/108680808X163766
- Alkatout I, Ulrich M, Liselotte M, et al. The development of laparoscopy—a historical overview. Front Surg. 2021;8:799442. https://doi.org/10.3389/fsurg.2021.799442
- Wang SH. Evaluating risk factors for surgical site infections and the effectiveness of prophylactic antibiotics in patients undergoing laparoscopic cholecystectomy. World J Gastrointest Surg. 2025;17(1):98567. https://doi.org/10.4240/wjgs.v17.i1.98567
- Muhamad AN, Cindy SJT, Mohd RD, et al. High incidence of multidrug-resistant organisms and modifiable risk factors associated with surgical site infections: a cohort study in a tertiary medical center in Kuala Lumpur, Malaysia from 2020 to 2023. Antimicrob Resist Infect Control. 2025;14(1):22. https://doi.org/10.1186/s13756-025-01537-2
- World Health Organization. Global report on infection prevention and control 2024. World Health Organization; 2024. https://www.who.int/publications/i/item/9789240103986. Accessed January 16, 2025.
- Hoffman T, Shitrit P, Chowers M. Risk factors for surgical site infections following open versus laparoscopic colectomies: a cohort study. BMC Surg. 2021;21:376. https://doi.org/10.1186/s12893-021-01379-w
- Cheng H, Brian PHC, Ireena MS, Nicole CF, Chris GC, Piet H. Prolonged operative duration increases risk of surgical site infections: a systematic review. Surg Infect. 2017;18(6):722–735. https://doi.org/10.1089/sur.2017.089
- Afifi IK, Eman AL, Khalil MA. Surgical site infections after elective general surgery in Tanta University Hospital: rate, risk factors and microbiological profile. Egypt J Med Microbiol. 2009;18(2):61–72. https://doi.org/10.12816/0024867
- Mundhada AS, Sunita T. A study of organisms causing surgical site infections and their antimicrobial susceptibility in a tertiary care government hospital. Indian J Pathol Microbiol. 2015;58(2):195–200. https://doi.org/10.4103/0377-4929.155313
- Iqbal R, Palwasha A, Zumaira T. Antimicrobial susceptibility pattern of pathogens isolated from surgical wound infections in tertiary care hospitals of Pakistan. Afr Health Sci. 2025;25(1):1–11. https://doi.org/10.4314/ahs.v25i1.2
- Nimkar P, Kanyal D. Understanding the financial burden of surgical site infections: a narrative review. Multidiscip Rev. 2025;8(3):2025084. https://doi.org/10.31893/multirev.2025084
- Liu H, Xing H, Zhang G, Wei A, Chang Z. Risk factors for surgical site infections after orthopaedic surgery: a meta-analysis and systematic review. Int Wound J. 2025;22(5):70068. https://doi.org/10.1111/iwj.70068
- Karnwal A, Jassim AY, Mohammed AA, Al-Tawaha ARMS, Selvaraj M, Malik T. Addressing the global challenge of bacterial drug resistance: insights, strategies, and future directions. Front Microbiol. 2025;16:1517772. https://doi.org/10.3389/fmicb.2025.1517772
- Rosa WE, Pandey S, Wisniewski R, et al. Antimicrobials in serious illness and end-of-life care: lifting the veil of silence. Lancet Infect Dis. 2025;25(5):e416–e431. https://doi.org/10.1016/S1473-3099(24)00832-6
- Hassan A, Rehman NU, Maqbool S, Arif M. Pharmacist-led antibiotic interventions in infectious disease patients: a Pakistani tertiary care antimicrobial stewardship study. J Pharm Policy Pract. 2025;18(1):2450017. https://doi.org/10.1080/20523211.2025.2450017
- Bwire GM, Magati RB, Ntissi HH, et al. Synthesizing evidence to guide the design and implementation of effective strategies for discontinuing postoperative antibiotic prophylaxis in surgical settings: an umbrella review post-WHO 2018 recommendations. Syst Rev. 2025;14(1):7. https://doi.org/10.1186/s13643-024-02750-7
- Paganetti C, Subotic U, Sanchez C, et al. Implementation of surgical site infection prophylaxis in children—a cross sectional prospective study. J Hosp Infect. 2025. https://doi.org/10.1016/j.jhin.2025.03.018