Coronavirus Epidemiology, Diagnosis, and Vaccination Statistics in Pakistan, China, and India: A Brief Review
Sana Ashraf*, Shakeela Parveen, Saba Ashraf, Mehwish Sultana, Urwah Ishaque, Zainab Shafqat, Saman Shabbir, Zainab Riaz, and Zunaira Faiz
Department of Zoology, The Government Sadiq College Women University Bahawalpur, Pakistan
Abstract
The global population has witnessed significant disruptions towards healthcare systems due to the Coronavirus pandemic. The World Health Organization (WHO) has designated it as a global health concern. Certain viruses within the Coronaviridae family predominantly inflict damage upon the respiratory system. The symptoms of infection may vary in severity, ranging from mild to severe, and in certain cases, can even lead to fatality. The most commonly observed symptoms include pyrexia, dyspnea, rigours, and gastrointestinal disturbances. Presently, COVID-19 stands as the prevailing subject of investigation within the academic community. The objective of the current study was to consolidate the present comprehensive material in a single source, hence enhancing the fundamental comprehension necessary for subsequent research endeavors.
Graphical Abstract
1. INTRODUCTION
Coronaviruses are enclosed viruses with a zoonotic-derived positive sense single-stranded RNA genome. They belong to the family of Corona viridae, the riboviral kingdom, and the nidoviral order. They carry harmful impacts on the health of birds, other creatures, and people [1]. The symptoms of Coronavirus 2 (SARS-CoV-2) range from minor conditions, such as cold or flu to severe ones including acute respiratory syndrome. The Coronavirus Single-stranded RNA has a helical form with a size between 26 and 32 kbps when coupled with the protein nucleocapsid [2]. These viruses often have a lipid bilayer around them that is home to the spikes and matrix proteins. These structural characteristics play an essential role for viral defense outside of the host organism [3]. The spike (S), small protein (S), and membrane (M) are three viral proteins (E). The virus is commonly referred to as "Corona" due to the spike that gives it a crown-like shape [4].
These viruses' primary target is the host's respiratory system which results in severe symptoms. People who are the carriers of these viruses tend to affect their surroundings including other people as well. The first case of COVID-19 was reported to Ministry of Health on February 26th, 2020 in Karachi, Sindh, Pakistan. On the same day in Islamabad, Pakistan’s Federal Ministry of Health confirmed the second case of COVID-19 [5]. The National Action Plan was submitted on February 12th by the Ministry of National Health Service, Regulation and Coordination in response to the government's requirement to establish strategies and plans in order to contain this outbreak in light of the ongoing surge in COVID-19 positive patients (World Health Organization). On January 30th, 2020, three Indian medical students who had recently returned from Wuhan, the epicenter of the epidemic, became the first people to be diagnosed with COVID-19 in India. These cases were reported in three different places in Kerala. Within a few weeks, a cluster of patients began to be admitted to hospitals in Wuhan with severe pneumonia. Majority of these patients belonged to the Huanan seafood wholesale market [6]. A new strain of coronavirus developed somewhere in November 2019 and within weeks of its emergence, hospitals started getting flooded with COVID-19 positive patients [7, 8].
1.1. COVID19 Epidemiology
In Wuhan, China, many cases of pneumonia were reported in December 2019. The cause of symptoms associated with respiratory system was identified through careful sequencing of samples known as 2019-nCoV (SARS-CoV-2) [9]. Healthcare professionals made up the majority of verified cases, indicating a significant human-human transmission. Since February 15th, 2020, there have been 60,000 pneumonia COVID-19 cases worldwide including China [10].
The SARS-CoV-2 (COVID-19) virus first appeared in Pakistan on February 26th, 2020, after two individuals who had just returned from Iran and were tested positive for the coronavirus. On March 2nd, 2020, ladies from Gilgit, Baltistan were reported to have the fifth Coronavirus case who had travelled from Iran. By 19th March 2020, the number of COVID-19 cases increased from 28-31 in Baluchistan and from 33-80 in Punjab (nih.org.pk). As per October 2022, Pakistan reported 1.57 million total cases of the COVID-19, out of which 30,619 fatalities were reported [11]. The prevalence of patients affected by COVID-19 in Pakistan by regions of residences is displayed in Table 1. This information was obtained from the Pakistani government's website, that is, www.covid.gov.pk.
Table 1. COVID-19 Case Distribution by Province of Origin in Pakistan (www.covid.gov.pk)
|
Region |
Confirmed cases |
Deaths |
|
Punjab |
522K |
13,614 |
|
KPK |
224K |
6370 |
|
Sindh |
594K |
8242 |
|
Baluchistan |
36K |
378 |
|
Islamabad |
139K |
1031 |
|
GB |
12K |
191 |
|
AJK |
44.5K |
793 |
1.2. Daily Cases and Death Statistics
The data of three countries was quantified which showed variation in daily confirmed cases and deaths. The highest mortality and disease spread rate was observed in India (Figure 1 and 2). The figures show that India had highest number of COVID-19 cases as well as death ratio among Pakistan and China.
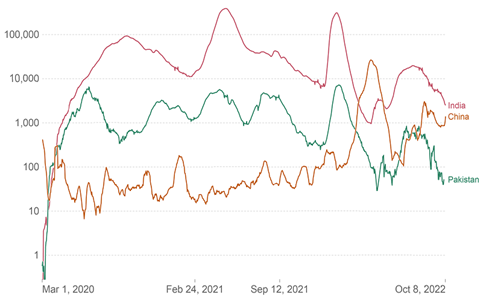
Figure 1. The Daily New Confirmed COVID-19 Cases
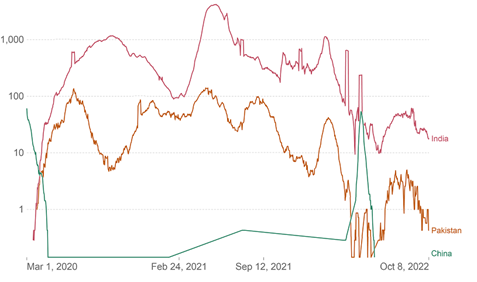
Figure 2. The Daily New Confirmed COVID-19 Deaths. Variable time span: Jan 27, 2020 – Oct, 2022 [Source: COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University]
1.3. Coronaviruses: Cause of Propagation and Illness
Bats have been determined to be the major source of the zoonotic transmission mode for Coronaviruses [12]. Nearly, all human viral outbreaks of Coronaviruses documented a comparable method of transmission, such as coughing and sneezing. Infected individuals can transmit the viruses to healthy individuals if they are in close proximity to one another [13]. Additionally, they might spread diseases to the surfaces of hospitals and other establishments that they visit. One of the primary preventive methods suggested for viral propagation include social estrangement. Coronaviruses impair the immune system's ability to function [14]. Most likely, they tend to infect the respiratory system, harm the respiratory airways, and cause a variety of respiratory disorders. Additionally, they encourage a number of immunological alterations that may render patient’s incapable of battling the infection [15]. For instance, during the acute episode of SARS-CoV transmission, immune cells, primarily T lymphocytes, such as CD4+ & CD8+, dramatically decline [16]. IgG antibodies, specific to SARS, are expected to start developing in the last two weeks of the acute stage of infection [17]. The pathogenesis of SARS-CoV is considerably more complicated, though. Resultantly, the majority of human body's key organs suffer serious harm [18]. As compared to SARS-CoV, Coronaviruses are more pathogenic [19, 20].
1.4. Immunopathology Caused by SARS-CoV-2 and its Effects on Human Health
Fever, shortness of breath, and lymphopenia are symptoms typically associated with SARS. Although, there weren't many upper respiratory-tract side effects, some patients did complain of loose bowels [21]. The illness began with a high fever and minor respiratory issues, however, quickly changed to pneumonia [22]. The acute lung and kidney infection is linked with current viral invasion and contamination known as MERS-CoV [23]. Muscle cramps, fever, migraines, and other common symptoms of illness have been listed here [24]. Pneumonia and kidney impairment are both experienced by MERS-Coronavirus patients [25].
COVID-19 can withstand severe malfunctions, such as pneumonia, a continuous temperature, and breathing difficulties. The symptoms of COVID-19, caused by SARS-CoV2, are similar to those of flu and hypersensitivity together with an increase in body temperature [26].
1.5. Symptoms and Clinical Outcomes of SARS-CoV-2 Induced Immunopathology in Human Beings
The clinical manifestations associated with SARS-CoV-2 infection leading to COVID-19 exhibit a wide range of symptoms, indicating intricate interaction between virus and human immune system (Figure 3). A prominent characteristic is fever which functions as a crucial signal of the body's immunological response to combat the encroaching viral pathogen. Upon entering the human body, SARS-CoV-2 triggers the production of cytokines, which are signaling molecules produced by immune cells. Certain cytokines possess pyrogenic properties, hence exerting their effects on the hypothalamus, a region located inside the brain. Subsequently, the hypothalamus initiates the recalibration of body's thermoregulatory set point to an elevated level, thus inducing pyrexia. The increase in body temperature results in the creation of an environment that is less conducive to the proliferation of viruses and also triggers a reaction from the immune system [27–30].
Furthermore, with the manifestation of fever, the presence of dyspnea, a medical term denoting difficulty in breathing, emerges as a notable sign of COVID-19. The primary target of SARS-CoV-2 is the cells that line the respiratory system including the airways and pulmonary tissue. The viral infection has the potential to inflict harm upon these cellular entities, resulting in an inflammatory response and disturbance of intricate pulmonary structures including the alveoli. The presence of inflammation and subsequent tissue damage within the respiratory system leads to a constriction of airflow and a disruption in the efficient exchange of oxygen and carbon dioxide (CO2). Consequently, individuals experience a sensation of breathlessness. The occurrence of this disease leads to the progression of mild respiratory distress to pneumonia which is a frequently seen consequence of COVID-19 [27–30].
Simultaneously, it has been shown that COVID-19 might result in lymphopenia, that is, a condition marked by a reduced number of lymphocytes, particularly T cells. The virus has the capability to directly infect and cause harm to lymphocytes, or the immune response mounted against the virus may result in the depletion of these cells. The compromised immune response impedes the body's capacity to adequately counteract the pathogen [27–30].
Certain people may also develop gastrointestinal issues, such as diarrhea. There is a prevailing belief that SARS-CoV-2 has the capability to penetrate and subsequently infect the cells inside the gastrointestinal system. The infiltration of this viral pathogen has the potential to induce inflammation inside the gastrointestinal tract, resulting in manifestations, such as diarrhea [28, 30].
Moreover, renal dysfunction, such as the occurrence of acute kidney injury (AKI), may arise as a consequence of viral infection or an inflammatory reaction occurring inside the renal system. In some cases, dialysis may be required to effectively treat the renal impairment. It is noteworthy to mention that previous instances of severe lung and kidney infections have been linked to other Coronaviruses, such as MERS-CoV [28, 31].
Non-specific symptoms, such as muscle cramps and headaches may be experienced by those afflicted with COVID-19. Muscle cramps may be associated with electrolyte imbalances and dehydration generated by fever, while headaches might potentially result from brain inflammation or vascular alterations [27, 28].
Moreover, some people may develop hypersensitivity responses that resemble the symptoms often associated with allergies when their immune system reacts to viral proteins. Although, the mechanisms behind these responses are not yet comprehensively elucidated, they have the potential to exacerbate the clinical manifestation of COVID-19 [28, 29]. As research continues to uncover more about the underlying processes driving these clinical outcomes, it becomes increasingly important to acknowledge the diverse and evolving nature of COVID-19 symptoms. Comprehending these symptoms and their fundamental causes is essential for the proficient identification, control, and intervention of individuals afflicted with COVID-19.
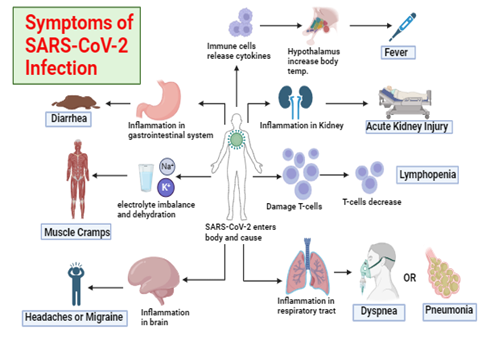
Figure 3. Symptoms of SARS-CoV-2 Infection Leading to COVID-19
1.6. Latest Diagnosis Methods - WHO and FDA Approved
Significant advancements have been made in the field of medical diagnostics, with a focus on accuracy, speed, and accessibility during the recent years. The World Health Organization (WHO) and the U.S. Food and Drug Administration (FDA) are two major regulatory bodies that play a crucial role in approving and endorsing the diagnostic methods.
1.6.1. Nucleic Acid Amplification Tests (NAATs). All the studies that were selected provided evidences that there is an immediate requirement for the development of improved procedures to diagnose COVID-19. The most common method, known as reverse transcription-PCR (RT-PCR), enables the processing of DNA and RNA to identify particular genes. This method is frequently applied to diagnose various viruses, such as Grapevine virus T and Zaire Ebola virus. With regard to SARS-CoV-2, the genes N, S, E, M, ORF1a, and ORF1b are typically utilized to determine whether or not the virus is present [32]. As soon as the genomic sequence of SARS-CoV-2 was determined, it became possible to run RT-PCR on the sequence. It became the gold-standard method for the diagnosis of COVID-19 and also ensured excellent accuracy [33]. RT-PCR has been recommended as the most sensitive NAAT, however, the majority of studies report RT-PCR as an assay that cannot fulfill the urgent requirements of the COVID-19 pandemic. This is because the technology behind RT-PCR relies on expensive and sophisticated equipment and reagents (with all of the logistical complications that arise as a result of their high prices). Moreover, it can only be performed by qualified individuals working in a laboratory, specifically equipped to handle pathogens [34].
1.6.2. Point-of-Care Testing (POCT). Point-of-Care Testing (POCT) refers to diagnostic tests that can be performed near the patient, often at their bedside, rather than in a centralized laboratory. These tests are designed to provide rapid results, enabling timely clinical decision-making. Rapid antigen tests for COVID-19 are a prime example of POCT. These tests are valuable for screening and diagnosing infectious diseases quickly, allowing for immediate isolation and treatment [35, 36].
1.6.3. Serological Assays. Serological assays detect antibodies in blood that are produced in response to an infection or vaccination. These tests are helpful to determine an individual's immune response and exposure history. Enzyme-Linked Immunosorbent Assay (ELISA) and chemiluminescent immunoassays are commonly used serological methods. They have been crucial in assessing immunity against diseases, such as COVID-19 and monitoring vaccine effectiveness [37, 38].
1.6.4. Imaging and Radiological Techniques. Advancements in medical imaging and radiology have led to more accurate and non-invasive diagnostic methods [37]. Techniques, such as magnetic resonance imaging (MRI), computed tomography (CT), and positron emission tomography (PET) scans allow healthcare professionals to visualize internal structures and detect abnormalities with high precision. These methods are widely used in diagnosing conditions ranging from neurological disorders to cardiovascular diseases [39].
1.6.5. Digital Pathology. Digital pathology involves the digitization of histopathological slides, enabling remote viewing, analysis, and sharing of microscopic images. This approach has improved collaboration among pathologists and specialists, leading to faster and more accurate diagnoses of diseases, such as cancer [40]. Digital pathology platforms enhance accuracy, reduce turnaround time, and facilitate the integration of artificial intelligence algorithms for automated analysis [41].
For the identification of viral agents and support of treatment, a rapid diagnostic method is required [30]. Real-time reverse transcription PCR (RT-PCR), reverse transcription loop mediated-isothermal amplification PCR, reverse transcription PCR, multiplex nucleic acid amplification, and microarray-based techniques are all strongly advised for the quick detection of respiratory virus invasion. These methods can be used to identify and treat this new Coronavirus, known as SARS-CoV-2 [42]. Amplicon sequencing can also employ the Pan Corona test [31]. For COVID-19, next-generation sequencing (NGS), real-time RT-PCR, cell culture, and electron microscopy are employed as methods of detection. Pathogenic agents in respiratory invasions can be found in virology labs using nucleic acid amplification assays (NAAT) and CT scans [29].
1.7. Vaccination
Vaccination against COVID-19 plays a crucial role in reducing the prevalence of the disease by offering protection to individuals and contributing to herd immunity. It is possible to develop vaccines using a variety of methods including viral-based vaccines, DNA-based vaccines, live-attenuated or inactivated vaccines, recombinant protein-based vaccines, and sub-unit vaccines [43]. Following points explain how COVID-19 vaccination helps to reduce its prevalence.
1.7.1. Protection for the Individual. The COVID-19 vaccines are made to provoke an immune response in the body without actually causing the disease itself. After receiving vaccination, a person's immune system is trained to detect the spike protein that is present on the surface of the SARS-CoV-2 virus which is responsible for causing COVID-19 [44]. The vaccinated individual is later put in a situation where they are exposed to real virus and then their immune system would be able to react swiftly and fight off the infection before it attempts to cause severe sickness.
1.7.2. Reduction in Severe Illness and Hospitalization. COVID-19 vaccines have proven to be highly effective in preventing severe illness, hospitalization, and deaths caused by the virus [45] (Fig 4). Even if vaccinated individuals do contract the virus, they are less likely to experience severe symptoms, hence reducing the burden on healthcare systems.
1.7.3. Herd Immunity. Herd immunity is acquired when a substantial percentage of a population develops immunity to a disease, either as a result of vaccination or having had the disease in the past. This may happen either naturally or as a result of vaccination. This makes it more difficult for the virus to propagate across the society which protects even those people who do not have an immunity to the disease [46]. It is expected that herd immunity against COVID-19 can be achieved when between seventy and eighty-five percent of the population becomes immune to the virus. The total transmission of the virus is reduced as more people become vaccinated against it which ultimately leads to a drop in the disease's prevalence.
1.7.4. Break the Chain of Transmission. Vaccinated individuals are less likely to transmit the virus to others because their immune systems can quickly neutralize the virus, preventing it from replicating in their bodies. This reduces the overall transmission of the virus within the community, helping to control its spread [44].
1.7.5. Variants Control. Vaccination also plays an effective role in controlling the emergence of new variants. When the virus spreads widely within a population, it has more opportunities to mutate, potentially giving rise to variants that could evade immunity generated from previous infections or vaccinations [47]. By reducing the prevalence of the virus, vaccines can limit the opportunities for new variants to develop and spread.
1.7.8. Global Impact. Widespread vaccination doesn't just protect a single community or country. It has a global impact as it slows down the international spread of the virus [48]. This is particularly important because the virus knows no borders and international travel can contribute to its rapid dissemination.
1.7.9. Economic Recovery. Reducing the prevalence of COVID-19 through vaccination also supports economic recovery [49]. As the virus is brought under control, businesses can operate more safely and lockdowns and restrictions can be eased, leading to a revitalized economy.
It is important to note that while vaccines are a powerful tool to reduce the prevalence of COVID-19, their effectiveness can be influenced by various factors, such as vaccine coverage, vaccine efficacy against variants, and the duration of immunity. To maximize the benefits of vaccination, a combination of vaccination efforts, public health measures, and ongoing research to monitor and adapt to changes in the virus is essential (Table 2). Likewise, a summary of covid-19 vaccine development and their approvals by various companies and countries is also given below in table 3.
Table 2. Vaccines Available and their Frequency in Different Sub-Continents
|
Vaccine |
Type |
Notable Regions of Distribution |
Administration Frequency |
References |
|
Pfizer-BioNTech |
mRNA |
North America, Europe, Asia |
Two doses, 3-6 weeks apart |
[50] |
|
Moderna |
mRNA |
North America, Europe, Asia |
Two doses, 4 weeks apart |
[51] |
|
AstraZeneca |
Viral Vector |
Europe, Asia, Africa, South America |
Varies (usually 2 doses) |
[52] |
|
Johnson & Johnson |
Viral Vector |
North America, Europe, Asia, Africa |
Single dose |
[53] |
|
Sinopharm |
Inactivated |
Asia, Middle East, Africa |
Two doses, 3-4 weeks apart |
[54] |
|
Sinovac |
Inactivated |
Asia, South America |
Two doses, 2-4 weeks apart |
[55] |
|
Sputnik V |
Viral Vector |
Russia, Latin America, Middle East, Asia |
Two doses, 3 weeks apart |
[56] |
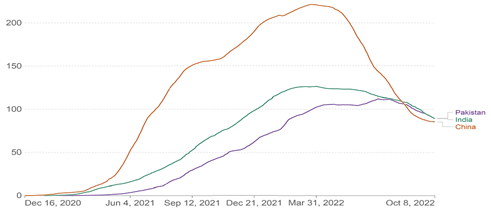
Figure 4. No. of COVID-19 vaccines administered per 100 people in population in last 12 months {Source: COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University}
Table 3. Summary of COVID-19 Vaccine Development and Approvals by Various Companies and Countries
|
Company and country |
Vaccine name |
Number of doses |
Approval and registration |
Reference |
|
Pfizer, USA and BioNTech, Germany |
BNT162b2 |
2 |
Phase III data from 45-539 individuals showed that the BNT162b2 vaccination proved to be 95% effective. Pfizer has received emergency vaccination registration in the United Kingdom and the United States, and the European Medicines Agency (EMA) is now reviewing a conditional marketing authorization. |
[57] |
|
Moderna, USA and US Government |
mRNA-1273 |
2 |
Nobody vaccinated with mRNA-1273 got infected with severe COVID-19 symptoms according to the final results of a Phase III study conducted in the United States that enrolled 30,000 participants. The FDA, EMA, and MHRA are continuously analyzing the study data. |
[57] |
|
CanSino Biologicals |
Ad5-nCov |
1 |
Before the completion of Phase III experiment, Chinese healthcare professionals and troops would be able to receive a vaccine made from human adenovirus Ad5 that carries the mRNA for the Spike protein. |
[58] |
|
Gamaleya Res Inst, Russia |
Sputnik V |
2 |
This sequentially given vaccination based on two human adenoviruses (Ad5 and Ad26) containing Spike protein mRNA was authorized for limited use before phase III study completion. |
[58] |
|
Johnson & Johnson, USA |
Ad26COVs1 |
1 |
The phase II study with a human adenovirus Ad26 containing Spike protein mRNA with up to 60, 000 participants was planned to be completed in 2020. A second phase II experiment examined two vaccination doses. |
[58] |
|
AstraZeneca, Sweden-UK Univ. Oxford, UK |
ChAdOx1 |
2 |
The Phase III experiment on this vaccine uses a chimpanzee adenovirus containing the Spike proteiniad mRNA and has 62 percent effectiveness. When ChAdox 1 was given a half dose and then a full dose, protection increased 90%. This vaccine's effectiveness is being studied further. |
[58] |
2. CONCLUSION
Coronaviruses are a type of non-segmented and positive-sense RNA viruses that are capable to infect the respiratory systems of both human beings and many animal species. The individual in question belongs to the taxonomic order Nidovirales and the family Coronaviridae. SARS-CoV, characterized by a 5% mortality rate, and MERS-CoV, associated with a fatality rate of 37%, were first identified in China and Saudi Arabia in 2002 and 2013, correspondingly. Coronaviruses have the potential to induce non-specific infestations, along with symptoms, such as moderate fever, tremors, chest infection, influenza-like illness, and alterations in respiratory rate, sore throat, and high fevers followed by pneumonia that pose a risk to life. Gastrointestinal and renal complications are also included within this category. At present, the Coronavirus presents a significant threat to global public health. As of the present, there have been reports of 6.56 million fatalities along with 622 million confirmed cases on a global scale. It is strongly recommended to employ multiplex nucleic acid amplification tests (NAAT), reverse transcription loop-mediated isothermal amplification (RTLAMP), and pan Coronavirus testing to diagnose disorders caused by Coronaviruses. Both Chloroquine, a medicine used to treat malaria, and Remdesivir (RDV), a broad-spectrum inhibitor of RNA polymerase, have demonstrated efficacy against SARS-CoV-2. Moreover, in order to prevent further infections, various antibiotic and antifungal drugs are used.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Bibliography
- Habas K, Nganwuchu C, Shahzad F, et al. Resolution of coronavirus disease 2019 (COVID-19). Expert Rev Anti-Infect Ther. 2020;18(12):1201–1211. https://doi.org/10.1080/14787210.2020.1797487
- Syed A. Coronavirus: a mini-review. Int J Curr Res Med Sci. 2020;6(1):8–10.
- Chavez S, Long B, Koyfman A, Liang SY. Coronavirus disease (COVID-19): a primer for emergency physicians. Am J Emerg Med. 2021;44:220–229. https://doi.org/10.1016/j.ajem.2020.03.036
- Javaid S, Javaid M. Survey on corona virus: a case study in Pakistan. Int J Med Sci Clin Res Rev. 2020;3(2):223–227.
- Quandt T, Wahl-Jorgensen K. The coronavirus pandemic as a critical moment for digital journalism: introduction to special issue: covering covid-19: the coronavirus pandemic as a critical moment for digital journalism. Digital Journal. 2021;9(9):1199–1207. https://doi.org/10.1080/21670811.2021.1996253
- Andrews M, Areekal B, Rajesh K, et al. First confirmed case of COVID-19 infection in India: a case report. Ind J Med Res. 2020;151(5):490–492. https://doi.org/10.4103/ijmr.IJMR_2131_20
- Kojima N, Adams K, Self WH, et al. Changing severity and epidemiology of adults hospitalized with Coronavirus Disease 2019 (COVID-19) in the United States after introduction of COVID-19 vaccines, March 2021–August 2022. Clin Infect Dis. 2023;77(4):547–557. https://doi.org/10.1093/cid/ciad276
- Tang B, Bragazzi NL, Li Q, Tang S, Xiao Y, Wu J. An updated estimation of the risk of transmission of the novel coronavirus (2019-nCov). Infect Dis Model. 2020;5:248–255. https://doi.org/10.1016/j.idm.2020.02.001
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:e102433. https://doi.org/10.1016/j.jaut.2020.102433
- Zhang Y, You L, Zou Y, et al. Epidemiology and molecular characterizations of Coronavirus from companion animals living in Chengdu, Southwest China. Transbound Emerg Dis, 2023;2023:e5056492. https://doi.org/10.1155/2023/5056492
- Chaudhry RM, Hanif A, Chaudhary M, et al. Coronavirus disease 2019 (COVID-19): forecast of an emerging urgency in Pakistan. Cureus. 2020;12(5):e8346. https://doi.org/10.7759%2Fcureus.8346
- Bakar NA, Rosbi S. Effect of coronavirus disease (COVID-19) to tourism industry. Int J Adv Enginer Res Sci. 2020;7(4):198–193.
- Chang L, Yan Y, Wang L. Coronavirus disease 2019: cronaviruses and blood safety. Trans Med Rev. 2020;34(2):75–80. https://doi.org/10.1016/j.tmrv.2020.02.003
- Singhal T. A review of coronavirus disease-2019 (COVID-19). Ind J Pediat. 2020;87(4):281–286. https://doi.org/10.1007/s12098-020-03263-6
- Zubair AS, McAlpine LS, Gardin T, Farhadian S, Kuruvilla DE, Spudich S. Neuropathogenesis and neurologic manifestations of the Coronaviruses in the age of Coronavirus Disease 2019: a review. JAMA Neurol. 2020;77(8):1018–1027. https://doi.org/10.1001/jamaneurol.2020.2065
- Rasmussen SA, Smulian JC, Lednicky JA, Wen TS, Jamieson DJ. Coronavirus disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obst Gynecol. 2020;222(5):415–426. https://doi.org/10.1016/j.ajog.2020.02.017
- Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. https://doi.org/10.1136/postgradmedj-2020-138234
- Sharma A, Farouk IA, Lal SK. COVID-19: a review on the novel coronavirus disease evolution, transmission, detection, control and prevention. Viruses. 2021;13(2):e202. https://doi.org/3390/v13020202
- Haslak F, Gunalp A, Kasapcopur O. A cursed goodbye kiss from severe acute respiratory syndrome-coronavirus-2 to its pediatric hosts: multisystem inflammatory syndrome in children. Curr Opin Rheumatol. 2023;35(1):6–16. https://doi.org/10.1097/BOR.0000000000000910
- Parsamanesh N, Pezeshgi A, Hemmati M, Jameshorani M, Saboory E. Neurological manifestations of coronavirus infections: role of angiotensin-converting enzyme 2 in COVID-19. Int J Neurosci. 2022;132(9):917–924. https://doi.org/10.1080/00207454.2020.1849193
- Feldman DE, Mazer B. Long covid in persons with self-reported arthritis - symptoms, associated factors and functional limitations. Arthritis Care Res. 2024;76(1):57–62. https://doi.org/10.1002/acr.25200
- Nandadeva D, Young BE, Stephens BY, et al. Blunted peripheral but not cerebral vasodilator function in young otherwise healthy adults with persistent symptoms following COVID-19. Am J Physiol Heart Circ Physiol. 2021;321(3):H479–H484. https://doi.org/10.1152/ajpheart.00368.2021
- Kang K, Lee SY, Lee DC. Neuro-ophthalmologic symptoms after coronavirus disease 2019 vaccination: a retrospective study. BMC Ophthalmol. 2023;23(1):e11. https://doi.org/10.1186/s12886-022-02747-7
- Zhang K, Liu X, Fu P, et al. Phenome-wide association study to explore the long-term symptoms after infection with novel coronavirus in the UK Biobank. medRxiv. 2023. https://doi.org/10.1101/2023.03.03.23286122
- McGuinn LA, Rivera NR, Osorio-Valencia E, et al. Changes in depressive and anxiety symptoms during COVID-19 in children from the PROGRESS cohort. Pediatr Res. 2023;94(1):349–355. https://doi.org/10.1038/s41390-022-02379-z
- Laracy JC, Robilotti EV, Yan J, et al. Comparison of coronavirus disease 2019 (COVID-19) symptoms at diagnosis among healthcare personnel before and after the emergence of the omicron variant. Infect Control Hosp Epidemiol. 2022;44(5):821–823. https://doi.org/10.1017/ice.2022.105
- Alraddadi BM, Al-Salmi HS, Jacobs-Slifka K, et al. Risk factors for Middle East respiratory syndrome coronavirus infection among healthcare personnel. Emerg Infect Dis. 2016;22(11):1915–1920. https://doi.org/10.3201/eid2211.160920
- Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, Evaluation, And Treatment of Coronavirus (COVID-19). StatPearls Publishing, 2022.
- Fani M, Teimoori A, Ghafari S. Comparison of the COVID-2019 (SARS-CoV-2) pathogenesis with SARS-CoV and MERS-CoV infections. Future Virol. 2020;15(5):317–323. https://doi.org/10.2217/fvl-2020-0050
- Lee JY, Kim Y-J, Chung EH, et al. The clinical and virological features of the first imported case causing MERS-CoV outbreak in South Korea, 2015. BMC Infect Dis. 2017;17(1):e498. https://doi.org/10.1186/s12879-017-2576-5
- Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. https://doi.org/10.1056/NEJMoa2001017
- Mustafa HM, Górska A, Mazzaferri F, et al. Nucleic acid amplification tests on respiratory samples for the diagnosis of coronavirus infections: a systematic review and meta-analysis. Clin Microbiol Infect. 2021;27(3):341–351. https://doi.org/10.1016/j.cmi.2020.11.002
- Xie C, Jiang L, Huang G, et al. Comparison of different samples for 2019 novel coronavirus detection by nucleic acid amplification tests. Int J Infect Dis. 2020;93:264–267. https://doi.org/10.1016/j.ijid.2020.02.050
- Payne D, Williams C, Jacob J, et al. Comparison of an ID NOW COVID-19 assay used at the point of care to laboratory-based nucleic acid amplification tests. J Clin Microbiol. 2023;61(7):e00413-23. https://doi.org/10.1128/jcm.00413-23
- Kumar A, Parihar A, Panda U, Parihar DS. Microfluidics-based point-of-care testing (POCT) devices in dealing with waves of COVID-19 pandemic: the emerging solution. ACS Appl Bio Mater. 2022;5(5):2046–2068. https://doi.org/10.1021/acsabm.1c01320
- Luppa PB, Müller C, Schlichtiger A, Schlebusch H. Point-of-care testing (POCT): current techniques and future perspectives. TrAC Trends Anal Chem. 2011;30(6):887–898. https://doi.org/10.1016/j.trac.2011.01.019
- Machado BAS, Hodel KVS, Barbosa-Júnior VG, Soares MBP, Badaró R. The main molecular and serological methods for diagnosing COVID-19: an overview based on the literature. Viruses. 2021;13(1):e40. https://doi.org/10.3390/v13010040
- Sidiq Z, Hanif M, Dwivedi KK, Chopra KK. Benefits and limitations of serological assays in COVID-19 infection. Indian J Tuberc. 2020;67(4), S163–S166. https://doi.org/10.1016/j.ijtb.2020.07.034
- Shibly KH, Dey SK, Islam MT-U, Rahman MM. COVID faster R–CNN: a novel framework to diagnose novel coronavirus disease (COVID-19) in X-ray images. Inform Med Unlocked. 2020;20:e100405. https://doi.org/10.1016/j.imu.2020.100405
- Cimadamore A, Lopez-Beltran A, Scarpelli M, Cheng L, Montironi R. Digital pathology and COVID-19 and future crises: pathologists can safely diagnose cases from home using a consumer monitor and a mini PC. J Clin Pathol. 2020;73(11):695–696. https://doi.org/10.1136/jclinpath-2020-206943
- Lujan GM, Savage J, Shana'ah A, et al. Digital pathology initiatives and experience of a large academic institution during the coronavirus disease 2019 (COVID-19) pandemic. Arch Pathol Lab Med. 2021;145(9):1051–1061. https://doi.org/10.5858/arpa.2020-0715-SA
- Scobey T, Yount BL, Sims AC, et al. Reverse genetics with a full-length infectious cDNA of the Middle East respiratory syndrome coronavirus. Proc Natl Acad Sci USA. 2013;110(40):16157–16162. https://doi.org/10.1073/pnas.1311542110
- Shahcheraghi SH, Ayatollahi J, Aljabali AA, et al. An overview of vaccine development for COVID-19. Ther Deliv. 2021;12(3):235–244. https://doi.org/10.4155/tde-2020-0129
- Atzrodt CL, Maknojia I, McCarthy RD, et al. A guide to COVID-19: a global pandemic caused by the novel coronavirus SARS-CoV-2. FEBS J. 2020;287(17):3633–3650. https://doi.org/10.1111/febs.15375
- Mohammed I, Nauman A, Paul P, et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: a systematic review. Hum Vaccin Immunother. 2022;18(1):e2027160. https://doi.org/10.1080/21645515.2022.2027160
- Omer SB, Yildirim I, Forman HP. Herd Immunity and Implications for SARS-CoV-2 Control. JAMA. 2020;324(20):2095–2096. https://doi.org/10.1001/jama.2020.20892
- Bian L, Gao Q, Gao F, et al. Impact of the Delta variant on vaccine efficacy and response strategies. Expert Rev Vaccines. 2021;20(10):1201–1209. https://doi.org/10.1080/14760584.2021.1976153
- Hiscott J, Alexandridi M, Muscolini M, et al. The global impact of the coronavirus pandemic. Cytokine Growth Factor Rev. 2020;53:1–9. https://doi.org/10.1016/j.cytogfr.2020.05.010
- Sucheran R. The COVID-19 pandemic and guesthouses in South Africa: Economic impacts and recovery measures. Dev South Afr. 2022;39(1):35–50. https://doi.org/10.1080/0376835X.2021.2003758
- Jeffery-Smith A, Dun-Campbell K, Janarthanan R, et al. Infection and transmission of SARS-CoV-2 in London care homes reporting no cases or outbreaks of COVID-19: prospective observational cohort study, England 2020. Lancet Reg Health Eur. 2021;3:e100038. https://doi.org/10.1016/j.lanepe.2021.100038
- Noor R, Maniha SM. A brief outline of respiratory viral disease outbreaks: 1889–till date on the public health perspectives. Virus disease. 2020;31(4):441–449. https://doi.org/10.1007/s13337-020-00628-5
- Zini G, De Cristofaro R. Diagnostic testing for differential diagnosis in thrombotic microangiopathies. Turk J Haematol. 2019;36(4):222–229. https://doi.org/10.4274/tjh.galenos.2019.2019.0165
- Tenforde MW, Patel MM, Ginde AA, et al. Effectiveness of severe acute respiratory syndrome coronavirus 2 messenger RNA vaccines for preventing coronavirus disease 2019 hospitalizations in the United States. Clin Infect Dis. 2021;74(9):1515–1524. https://doi.org/10.1093/cid/ciab687
- Xia S, Zhang Y, Wang Y, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect Dis. 2021;21(1):39–51. https://doi.org/10.1016/S1473-3099(20)30831-8
- Liu Y, Mao B, Liang S, et al. Association between age and clinical characteristics and outcomes of COVID-19. Eur Respir J. 2020;55(5):e2001112. https://doi.org/10.1183/13993003.01112-2020
- Baraniuk C. Covid-19: what do we know about Sputnik V and other Russian vaccines? BMJ. 2021;372:en743. https://doi.org/10.1136/bmj.n743
- AZD1222 vaccine met primary efficacy endpoint in preventing COVID‐19. AstraZeneca Web site. https://www.astrazeneca.com/media-centre/press-releases/2020/azd1222hlr.html#. Updated November, 2020. Accessed February, 2024.
- Shabir AM, Vicky B, Clare LC, et al. Safety and efficacy of the ChAdOx1 nCoV-19 (AZD1222) Covid-19 vaccine against the B.1.351 variant in South Africa. medRxiv. 2021. https://doi.org/10.1101/2021.02.10.21251247