Current Situation of Breast Cancer in Pakistan and the Dire Need of Early Diagnosis
Najeeb Ullah Khan*, Imad Azam, and Atif Hayat
Institute of Biotechnology and Genetic Engineering, The University of Agriculture, Peshawar, Pakistan
Abstract
Globocan statistics underscore Pakistan’s noticeable position in terms of the breast cancer burden, highlighting a concerning and escalating trajectory in its daily progression. Breast cancer stands as the most predominant and fatal malignancy in Pakistan, reporting 25,928 cases in the year 2020, accounting for 14% of all cancer diagnosis. The country is reported to have the maximum incidence and mortality rates in Asia, a dire result of the lack of national cancer registry. Late diagnosis, often determined by sociocultural factors, considerably contributes to the high mortality rate. Several risk factors, such as reproductive factors, age, dietary habits, further complicate the situation. Moreover, economic obstacles deter many from receiving the required treatment. The current review features the dire need for inclusive policies and improved affordability to battle breast cancer’s escalating influence in Pakistan.
Introduction
Worldwide, the number of breast cancer cases has seen a persistent increase and such cases remain a significant reason for mortality [1]. In 2020, approximately 2.3 million women were diagnosed with breast cancer, resulting in 685,000 associated mortalities. Breast cancer stands as the most predominant neoplastic growth, worldwide. In this regard, 7.8 million women were determined to have breast cancer disease toward the end of 2020 [2]. The risk of creating breast cancer has ascended in Pakistan, with one in every nine women with a lifetime chance to have this malignant growth [3]. Pakistan exhibits the highest mortality and incidence rates among all other Asian countries [4]. Furthermore, when contrasted with neighboring countries such as India or Iran, the rate of incidence was found to be 2.5 times higher in Pakistan [5, 6]. Pakistan faces a significant challenge in data quality for breast cancer records, primarily due to the lack of a national cancer registry. According to facility-based projections and studies, the estimation of new cases is between 34,000 and 90,000 cases, with 16,232 deaths [7].
2. CURRENT SITUATION OF BREAST CANCER IN PAKISTAN
2.1. Delayed Diagnosis of Breast Cancer as a Major Cause of Mortality
Among all the causative agents for breast cancer, delayed diagnosis is a major factor in increasing breast cancer mortality rate in Pakistan. Delay in seeking proper healthcare treatment is the reason that many cases of breast cancer have been reported at the last stages, resulting in mortality [8]. Based on previous reports, mortality in 1/3rd of women aged 50 or above can be prevented if the cancer is diagnosed in early stages. Patients diagnosed with breast cancer in its early stages have a higher chance of survival than patients diagnosed in later stages. The elevated prevalence of breast cancer may be attributed to certain factors, such as lack of knowledge, as well as social and financial constraints [9]. A noticeable causative factor of mortality among Pakistani women is the reluctance to seek medical help from male physicians, driven by the cultural taboo associated with exposing breasts, which is perceived as a sign of disrespect. A study conducted to evaluate the reasons behind delayed diagnosis demonstrated that approximately 40% of the women surveyed resorted to home remedies and alternative treatments in attempt to self-manage breast cancer, with the primary motivation being the avoidance of disclosing their breasts to male healthcare professionals. Additionally, 17% chose to ignore symptoms, while 10% were cognizant of their cancer but hesitated to seek treatment due to the cultural norms of associating breasts with secrecy and the imperative to conceal them at all costs [10]. The multiple reasons behind the delayed diagnosis of breast cancer are depicted in Figure 1 [11].
The likelihood of survival significantly diminishes when breast cancer is diagnosed at advanced stages. A recent study showed that about 46.26% of patients consulted doctors in Stage II, while 36.46% were in Stage III at the time they presented themselves. This is alarming as the cancer survival chances decrease if presented at later stages [12], as shown in Figure 2.
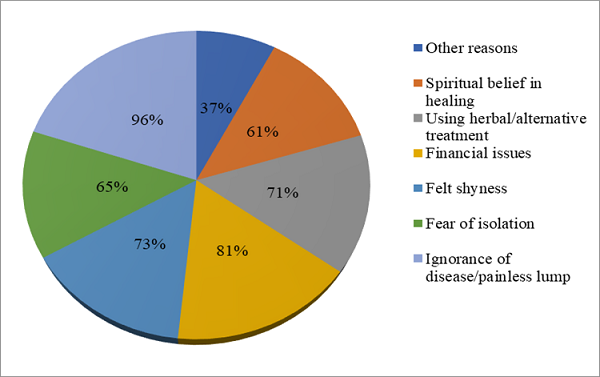
Figure 1. Percentage of Patients with Reasons for Delayed Diagnosis [11]
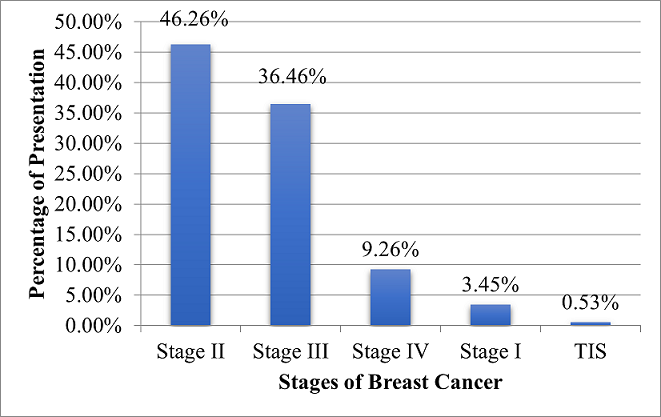
Figure 2. Stages of breast cancer at which patients presented themselves for medical assistance [12]
2.2. Other Risk Factors for Increasing Breast Cancer Prevalence
Age is directly related to the incidence of breast cancer [13]. Women of age 40 years and above have been recorded to suffer from this cancer. Studies reported that women experiencing late menopause at age 55 or above are at the risk of breast cancer more than the ones who undergo menopause at 45 years of age [14]. Likewise, childbearing at an early age lessens the incidence of breast cancer. Delay in child bearing increases the risk of breast cancer by 3% per year. Also, increased number of pregnancies and breastfeeding are protective factors against breast cancer. A study reported that women with one child are 15% more likely to develop breast cancer than women with two children [15].
Melatonin hormone plays an important role in preventing cancer due to its anti-carcinogenic properties. However, reduced and disrupted sleep patterns reduce melatonin which may increase the chances for breast cancer. Reports indicated that more than 4% of breast cancer patients have the risk factor of night shifts and disrupted sleep patterns [16]. Similarly, smokers have a 20% more chance to suffer from breast cancer [17]. Additionally, physical barriers might also cause psychosocial stress as patients are reluctant to go through the demanding screening and treatment processes [18]. Only a few studies have examined the factors that contribute to cancer screening and treatment delays in Pakistan, such as lack of awareness [19], low socioeconomic status, accessibility and affordability of cancer treatments, and other risk factors (exposure to dangerous industrial chemicals) [20]. Vitamin D deficiency can cause the conversion of non-metastatic cells to metastatic cells. Every one out of three women suffers from Vitamin D deficiency in Pakistan. Physical inactivity is directly related to breast cancer as it is associated with obesity which is the mother of all diseases. Females with increased BMI are at a much higher risk of developing breast cancer due to the increased amount of free estrogen produced as a result of elevated aromatase activity in adipose tissues [21]. Hence, physical inactivity is directly related to BMI, hormones, menstrual cycle, and immune system [22]. Women show a high rate of obesity than men (Figure 3). World obesity statistics show a national obesity risk of 6.5/10 in Pakistan.
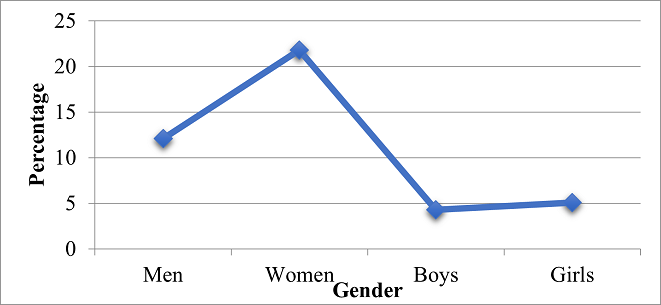
Figure 3. Gender-wise Prevalence of Obesity in Pakistan
Unhealthy dietary habits among the people of Pakistan represent a significant risk factor contributing to the burden of breast cancer. Research suggests that lifestyle modification can reduce the risk of breast cancer up to 40%. Among others, Pakistani diet is composed of fried items, fast foods, and trans fats [23]. The unhealthy diet patterns frequently used by the Pakistani population, which promote breast cancer and reduce immunity, include the consumption of processed meat, refined carbohydrates, white sugar, carbonated drinks, processed juices, excessive tea, tea whiteners, and caffeine (Table 1) [24]. For instance, barbecue produces heterocyclic amines and carcinogens can increase the risk of breast cancer [25].
Table 1. Unhealthy Foods Associated with Increased Risk of Breast Cancer in Pakistan
|
Sr. No. |
Unhealthy Food |
Sr. No. |
Unhealthy Food |
|
1 |
Fast food, fried food, oily food (halwa puri, samosas, pakoras) |
8 |
Commercial mayonnaise |
|
2 |
Processed meat |
9 |
Margarine |
|
3 |
Excessive tea, tea whiteners, caffeine |
10 |
Products with fructose corn syrup and sorbitol |
|
4 |
White and brown sugar |
11 |
Doe |
|
5 |
Carbonated drinks, processed juices |
12 |
Supplements for cancer prevention |
|
6 |
Barbecue |
13 |
Fried fish /contaminated fish |
|
7 |
Alcohol |
|
|
A study demonstrated that unmarried women are more likely to be associated with the risk of developing breast cancer as compared to married women [26]. Likewise, breastfeeding and pregnancy reduce the risk of breast cancer. Since pregnancy results in fewer menstrual cycles, the exposure to endogenous hormones is also reduced which reduces the risk of cancer [20]. Also, breastfeeding involves the maturation of breast cells. Matured and differentiated cells are less likely to develop cancer [27].
The effect of oral contraceptives on female hormones is complex. Although, studies show a positive relationship between the use of oral contraceptives and the incidence of breast cancer [28]. There are variable and complex reasons behind this finding. Possible reasons could be the enhancement of mitotic activity in breast cells due to estrogen and progesterone, while protective anovulation as estrogen is directly involved in the proliferation and differentiation of breast cells [29]. Table 2 indicates the list of factors associated with breast cancer incidence in Pakistan.
Table 2. Potential Factors Associated with Breast Cancer Incidence in Pakistan
|
1 |
Age |
11 |
Hesitation for presentation |
|
2 |
Environmental Factors |
12 |
Socioeconomic status |
|
3 |
Genetics |
13 |
Late menopause |
|
4 |
Family history |
14 |
Late first pregnancy |
|
5 |
Unhealthy food |
15 |
Use of local low quality hair dyes |
|
6 |
Physical inactivity |
16 |
Use of low quality plastics for microwave |
|
7 |
Obesity |
17 |
Vitamin D deficiency |
|
8 |
Tobacco |
18 |
Alcohol |
|
9 |
Oral Contraceptives |
19 |
Sleep routine and night shifts |
|
10 |
Marital Status |
20 |
Prolonged use of anti-hypertensive drugs |
2.3. Hospitals and Research Centers
Currently, there are approximately 30 cancer hospitals (Figure 4) that effectively provide services to breast cancer patients including 11 hospitals in the Sindh province, 7 each in Khyber Pakhtunkhwa and Punjab, and 1 each in Gilgit, Baluchistan, and Baltistan. Unfortunately, there is no cancer hospital in Azad Kashmir [30]. Previous studies conducted among different cities in Pakistan illustrated the statistical value of breast cancer among patients, resulting in a higher proportion in Lahore and a lower proportion in Gujrat, Faisalabad, Okara, and Sahiwal [31].
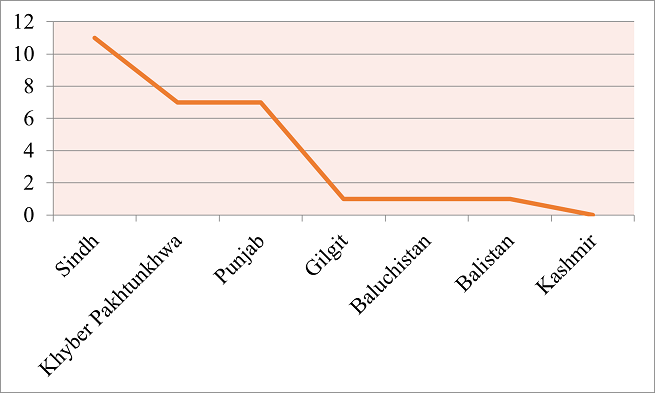
Figure 4. Number of Breast Cancer Hospitals in Pakistan [31]
There are several breast cancer research institutes functioning in Pakistan. Table 3 lists the top 20 research centers that conduct breast cancer research in Pakistan [32].
Table 3. Top 20 Breast Cancer Research Centers in Pakistan [32]
|
Rank |
Name of Research institutes for breast cancer |
City |
|
1 |
Comsats University |
Islamabad |
|
2 |
Aga Khan University |
Karachi |
|
3 |
Quaid e Azam University |
Islamabad |
|
4 |
University of Karachi |
Karachi |
|
5 |
Govt. College University |
Faisalabad |
|
6 |
Shaukat Khanum Memorial Cancer Hospital & Research Center |
Lahore |
|
7 |
University of the Punjab |
Lahore |
|
8 |
Dow University of Health Sciences |
Karachi |
|
9 |
Bahauddin Zakariya University |
Multan |
|
10 |
University of Lahore |
Lahore |
|
11 |
University of Sargodha |
Sargodha |
|
12 |
University of Agriculture |
Faisalabad |
|
13 |
National University of Science & Technology |
Islamabad |
|
14 |
Abdul Wali Khan University |
Khyber-Pakhtunkhwa |
|
15 |
King Edward Medical University |
Lahore |
|
16 |
Islamia University |
Bahawalpur |
|
17 |
University of Veterinary & Animal Sciences |
Lahore |
|
18 |
University of Health Sciences |
Lahore |
|
19 |
University of Gujrat |
Gujrat |
|
20 |
Armed Forces Institute of Pathology |
Rawalpindi |
2.4. Breast Cancer Status in Different Cities of Punjab with BRCA1/BRCA2 Mutations
Among all the cities of Punjab, Lahore shows the highest rate of prevalence of breast cancer with 46% of women with BRCA1/BRCA2 mutations [33], as shown in Figure 5.
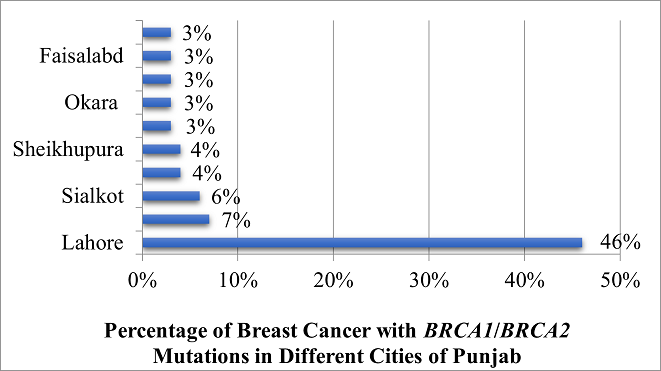
Figure 5. Status of Different Cities of Punjab with BRCA1/BRCA2 Mutations [33]
2.5. Incidence and Mortality Rate of Breast Cancer in 2020
Based on the data provided by Globocan, Asia ranked first for the number of deaths due to breast cancer in 2020. The percentage of mortality was calculated as 50.5% in Asia, 20.7% in Europe, 12.5% in Africa, 8.5% in Latin America, 7.1% in North America, and 0.74% in Oceania, as shown in Figure 6.
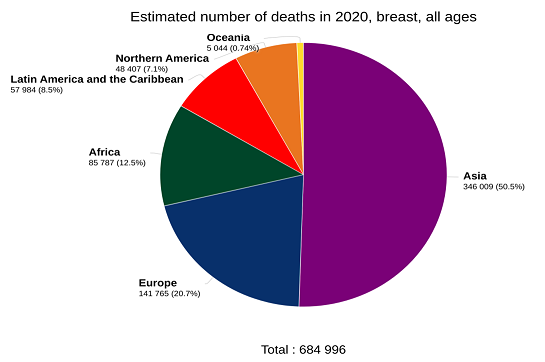
Figure 6. Estimated Deaths in 2020 in Different Continents Due to Breast Cancer [34]
According to the 2020 statistics of the World Health Organization (WHO), the estimated number of breast cancer prevalent cases for a 5-year period in Asia was 3,218,496 (41.3%), for Europe the number was 2,138,117 (27.4%), for North America the number was 1,189,111 (15.3%), for Latin America and the Caribbean the number was 710,039 (9.1%), for Africa the number was 429,220 (5.5%), and for Oceania the number was 105,734 (1.4%), as shown in Figure 7.
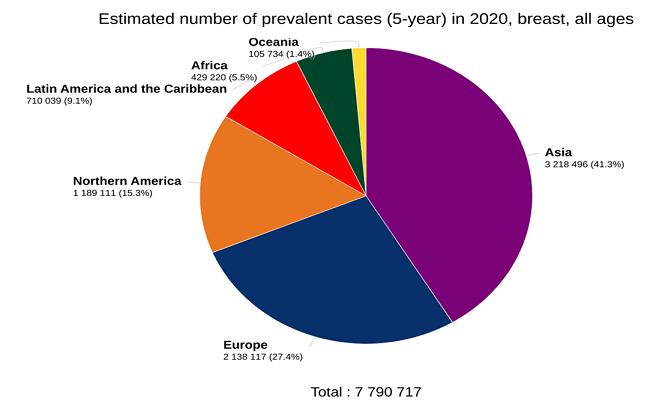
Figure 7. Estimated Number of Prevalent Breast Cancer Cases in 5-year Period (2015-2020) in Various Continents
Similarly, the estimated number of new breast cancer cases in Asia was reported to be 4,482,515, which is higher than other continents, as shown in Figure 8.
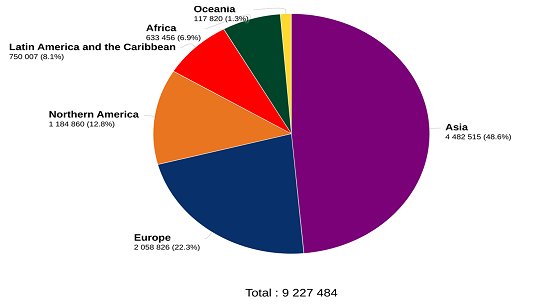
Figure 8. Estimated Number of New Breast Cancer Cases in 2020
Cancer reports of 2020 indicated the incidence of breast cancer to be the highest among all cancers in Pakistan, as shown in Figure 9.
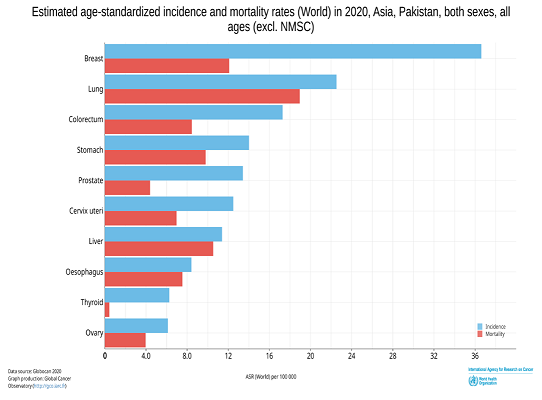
Figure 9. Prevalence of Different Cancers in Pakistan in 2020 with the Highest Incidence of Breast Cancer among All Cancers
2.6. Treatment of Breast Cancer in Pakistan
In low-income countries like Pakistan, it is often impossible for patients to afford breast cancer treatment. According to 2019 statistics, Pakistan is ranked 154th among 195 countries for expanding healthcare and it spends only a fixed 3.4% of GDP for health. On the open Budget Index on health, Pakistan scored poorly at 28/100. The minimum cost of breast cancer treatment is 3-4 hundred thousand PKR and it can go up to a million or more, depending on the stage of cancer. Although many research institutes and hospitals, such as Shaukat Khanum Cancer Hospital, Pink Ribbon Hospital, PAEC, Cancer Care Hospital, Bait-ul-Sakoon, and INMOL offer discounted treatments to low-income patients but the cost is so high that even the middle class cannot afford it. Figure 10 shows the comparison of total GDP spent on health among a few countries in 2019, while the current treatment methodologies available in Pakistan and a list of novel strategies used worldwide are listed in Table 4.
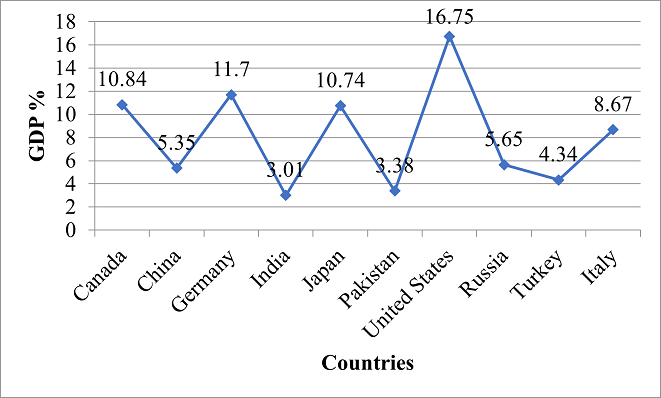
Figure 10. Country-wise Percentage of GDP Spent on Healthcare in 2019
Table 4. List of Breast Cancer Treatment Methods Used in Pakistan and Worldwide
|
Novel Treatments of Breast Cancer in the World |
Treatment of Breast Cancer in Pakistan |
|
Repurposing drugs |
Surgery · Lumpectomy · Mastectomy · Lymph node removal · Breast reconstruction · Prophylactic mastectomy · Prophylactic ovary removal |
|
Metronomic therapy |
Radiotherapy |
|
Antibody-Drug Conjugation Systems (ADCs) |
Chemotherapy |
|
Nanoparticles and micelles |
Targeted Therapy |
|
Targeting Breast Cancer Stem Cells (BCSCs) |
Anti-Hormone Therapy |
2.7. Future of Breast Cancer in Pakistan (2020-2040)
The escalating burden of breast cancer and its rising trend over the past few decades remains an alarming concern for the future of healthcare in Pakistan. WHO estimated that the number of new cases in 2020 in Pakistan was 25928. This number is predicted to get doubled to 49008 in 2040, if the current situational factors such as lack of awareness, delayed diagnosis, and lack of latest treatment methods continue to prevail (Figure 11).
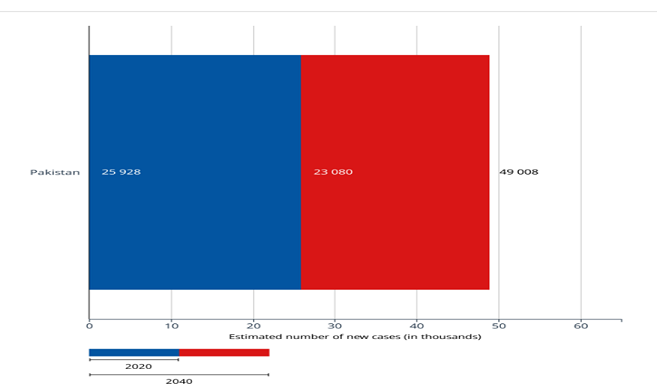
Figure 11. Estimated Number of New Cases of Breast Cancer from 2020 to 2040 in Pakistan [1]
Similarly, the estimated number of deaths in Pakistan due to breast cancer in 2020 was 13725, which is likely to become 26491 by 2040, considering the same situational factors prevail as of today (Figure 12 and Figure 13).
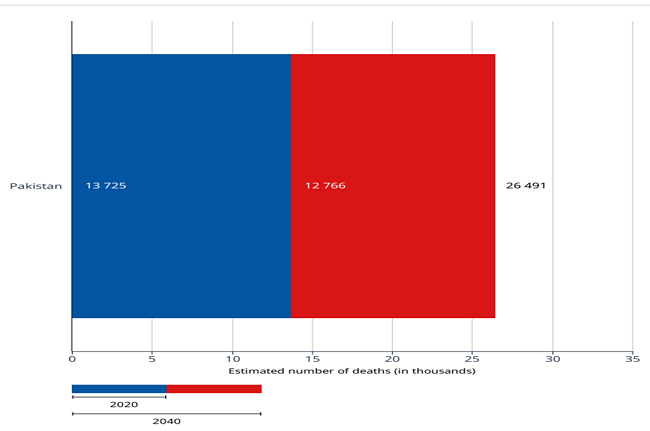
Figure 12. Estimated Number of Deaths from 2020 to 2040 Due to Breast Cancer in Pakistan [2]
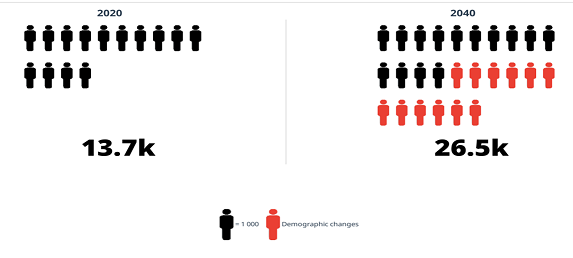
Figure 13. Estimated Number of Deaths from 2020 to 2040 Due to Breast Cancer in Pakistan[3]
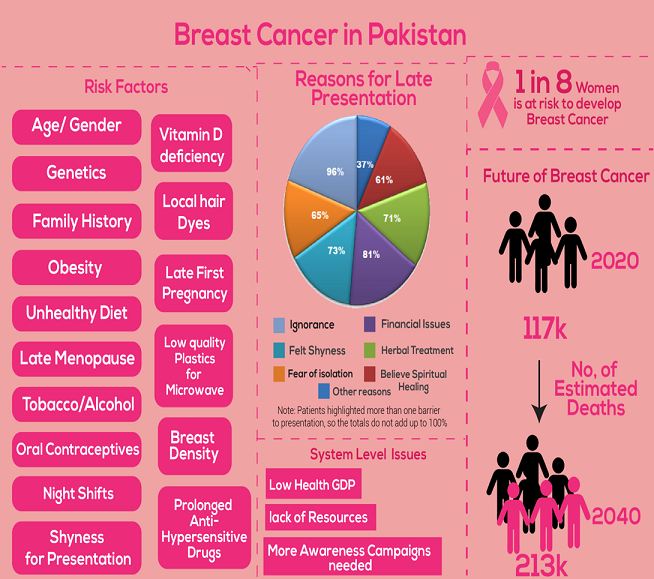
Figure 14. Graphic Representation of the Prevailing Breast Cancer Situation in Pakistan
CONCLUSION
According to Globocon observatory statistics, Pakistan ranks among the top countries with a substantial burden of breast cancer cases. The statistics underscore an alarming situation due to the upward trend of breast cancer cases in the country. Several risk factors contribute to this concerning situation including lack of awareness, hesitation of female patients toward male doctors, the prevailing social stigma surrouding the secreacy of breasts irrespecrive of life-threatning consequences, socioeconomic disparities, a small health budget, unhealthy diet patterns, reliance on homemade remedies for the cure, and spiritual superstitions. Multifactorial barriers in diagnosis including cultural pressure and low income have led to a late-stage presentation to doctors which is a leading cause of mortality. There is a dire need to increase awareness among the local population of Pakistan regarding the early symptoms of breast cancer in order to avoid the disease burden. The lack of patient follow-up is the reason why accurate data cannot be calculated, as most of the women do not present for diagnosis and bear the pain to death. Currently, 30 cancer hospitals and 20 cancer research institutes provide services to patinets. Many awareness campaigns have been launched also. Still, a lot needs to be done to overcome this health hazard (Figure 14). Global statistics predict the doubling of the burden of this disease by year 2040 if the current conditions persist unchecked.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Funding details
This research did not receive grant from any funding source or agency.
Bibliography
- Suleiman AK. Awareness and attitudes regarding breast cancer and breast self-examination among female Jordanian students. J basic Clin Pharm. 2014;5(3):74–78. https://doi.org/10.4103/0976-0105.139730
- Hussain I, Majeed A, Masood I, et al. A national survey to assess breast cancer awareness among the female university students of Pakistan. PLoS One. 2022;17(1):e0262030. https://doi.org/10.1371/journal.pone.0262030
- Zaheer S, Shah N, Maqbool SA, Soomro NM. Estimates of past and future time trends in age-specific breast cancer incidence among women in Karachi, Pakistan: 2004–2025. BMC Public Health. 2019;19:1–9 https://doi.org/10.1186/s12889-019-7330-z
- Mahmood S, Rana TF, Ahmad M. Common determinants of Ca breast - a case control study in Lahore. Ann King Edward Med Univ. 2016;12(2). https://doi.org/10.21649/akemu.v12i2.880
- Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2014;64(3):381–387. https://doi.org/10.1136/gutjnl-2014-308124
- Majeed AI, Hafeez A, Khan SA. Strengthening Breast Cancer Screening Mammography Services in Pakistan Using Islamabad Capital Territory as a Pilot Public Health Intervention. Healthcare. 2022;10(6):e1106. https://doi.org/10.3390/healthcare10061106
- Baloch AH, Shuja J, Daud S, et al. Various Aspects, Patterns and Risk Factors in Breast Cancer Patients of Balochistan. Asian Pacific J Cancer Prev. 2012;13(8):4013–4016. https://doi.org/10.7314/APJCP.2012.13.8.4013
- Rivera-Franco MM, Leon-Rodriguez E. Delays in breast cancer detection and treatment in developing countries. Breast Cancer Basic Clin Res. 2018;12:1–5. https://doi.org/10.1177/1178223417752677
- Banning M, Hafeez H, Faisal S, Hassan M, Zafar A. The impact of culture and sociological and psychological issues on muslim patients with breast cancer in Pakistan. Cancer Nurs. 2009;32(4):317–324. https://doi.org/10.1097/NCC.0b013e31819b240f
- Khan NH, Duan S-F, Wu D-D, Ji X-Y. Better reporting and awareness campaigns needed for breast cancer in Pakistani women. Cancer Manag Res. 2021;13:2125–2129.
- Gulzar F. Identifying the barriers of delayed presentation in pakistani breast cancer patients undergoing care at tertiary hospital. J Glob Oncol. 2018;4(2). https://doi.org/10.1200/jgo.18.86600
- Soomro R, Faridi S, Khurshaidi N, Zahid N, Mamshad I. Age and stage of breast cancer in Pakistan: An experience at a tertiary care center. J Pak Med Assoc. 2018;68(11):1682–1685.
- Hisam Z, Soomro NM, Lakhiar RA. Evaluation of risk factors for breast cancer in pakistani women. Pakistan J Public Heal. 2020;9(3):139–143. https://doi.org/10.32413/pjph.v9i3.168
- Asif HM, Sultana S, Akhtar N, Rehman JU, Rehman RU. Prevalence, risk factors and disease knowledge of breast cancer in Pakistan. Asian Pac J Cancer Prev. 2014;15(11):4411–4416. https://doi.org/10.7314/APJCP.2014.15.11.4411
- Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, Stanisławek A. Breast cancer-epidemiology, risk factors, classification, prognostic markers, and current treatment strategies-an updated review. Cancers. 2021;13(17):e4287 https://doi.org/10.3390/cancers13174287
- Li Y, Li S, Zhou Y, et al. Melatonin for the prevention and treatment of cancer. Oncotarget. 2017;8(24):39896–39921. https://doi.org/10.18632%2Foncotarget.16379
- Goldvaser H, Gal O, Rizel S, et al. The association between smoking and breast cancer characteristics and outcome. BMC Cancer. 2017;17(1):e624. https://doi.org/10.1186/s12885-017-3611-z
- Mclaughlin B, Yang J, Yoo W, et al. The effects of expressing religious support online for breast cancer patients. Health Commun. 2015;31(6):762–771. https://doi.org/10.1080/10410236.2015.1007550
- Raza S, Sajun SZ, Selhorst CC. Breast cancer in Pakistan: Identifying local beliefs and knowledge. J Am Coll Radiol. 2012;9(8):571–577. https://doi.org/10.1016/j.jacr.2012.02.020
- Bano R, Ismail M, Nadeem A, Khan MH, Rashid H. Potential risk factors for breast cancer in Pakistani women. Asian Pacific J Cancer Prev. 2016;17(9):4307–4312.
- Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults. Lancet. 2014;384(9945):755–765. https://doi.org/10.1016/S0140-6736(14)60892-8
- Xia X, Chen W, Li J, et al. Body mass index and risk of breast cancer: a nonlinear dose-response meta-analysis of prospective studies. Sci Rep. 2014;4:e7480. https://doi.org/10.1038/srep07480
- Seiler A, Chen MA, Brown RL, Fagundes CP. Obesity, dietary factors, nutrition, and breast cancer risk. Curr Breast Cancer Rep. 2018;10(1):14–27. https://doi.org/10.1007/s12609-018-0264-0
- Yue G. The pink ribbon campaign in Chinese fashion magazines. Lifestyle Media Asia. 2016:82–95. https://doi.org10.4324/9781315736563-6
- Basra MAR, Saher M, Athar MM, Raza MH. Breast cancer in Pakistan a critical appraisal of the situation regarding female health and where the nation stands. Asian Pac J Cancer Prev. 2016;17(7):3035–3041.
- Aizer AA, Chen M-H, McCarthy EP, et al. Marital status and survival in patients with cancer. J Clin Oncol. 2013;31(31):3869–3876. https://doi.org/10.1200%2FJCO.2013.49.6489
- Ilic M, Vlajinac H, Marinkovic J. Breastfeeding and risk of breast cancer: Case-control study. Women Health. 2015;55(7):778–794. https://doi.org/10.1080/03630242.2015.1050547
- Marchbanks PA, Curtis KM, Mandel MG, et al. Oral contraceptive formulation and risk of breast cancer. Contraception. 2012;85(4):342–350. https://doi.org/10.1016/j.contraception.2011.08.007
- Casey PM, Cerhan JR, Pruthi S. Oral contraceptive use and the risk of breast cancer. Mayo Clin Proc. 2008;83(1):86–91. https://doi.org/10.4065/83.1.86
- Arshad S, Rehman MU, Abid F, Yasir S. Current situation of breast cancer in Pakistan with the available interventions. Int J Biosci. 2019;14(6):232–240. http://dx.doi.org/10.12692/ijb/14.6.232-240
- Khokher S, Qureshi MU, Fatima W, Mahmood S, Saleem A. Impact of a Breast health awareness activity on the knowledge level of the participants and its association with socio-demographic features. Asian Pacific J Cancer Prev. 2015;16(14):5817–5822. http://dx.doi.org/10.7314/apjcp.2015.16.14.5817
- Ahmad S, Rehman SU, Iqbal A, Farooq RK, Shahid A, Ullah MI. Breast cancer research in Pakistan: A bibliometric analysis. SAGE Open. 2021;11(3):1–17. https://doi.org/10.1177/21582440211046934
- Abbas S, Siddique A, Shahid N, Khan RT, Fatima W. Breast cancer risk associated with BRCA1/2 variants in the Pakistani population. Breast Cancer. 2018;26(3):365–372. https://doi.org/10.1007/s12282-018-0932-y
- Li J, Kuang XH, Zhang Y, Hu DM, Liu K. Global burden of gastric cancer in adolescents and young adults: estimates from GLOBOCAN 2020. Public Health. 2022;210:58–64. https://doi.org/10.1016/j.puhe.2022.06.010