Detection of Single Nucleotide Polymorphism (SNP) rs2235371 of IRF6 Gene in Patients with Non-Syndromic Cleft Lip and Palate
Kifayat Ullah1*, Tooba Komal2, and Ghafran Ali1
1Institute of Biotechnology, Gulab Devi Educational Complex, Lahore, Pakistan
2University of Jhang, Jhang, Pakistan
Abstract
The orofacial clefts are the most common structural birth defects among newborn babies. They consist of two groups, namely Cleft Palate (CP) and Cleft Lip (CL). Infants born with clefts have considerable problems during communication, swallowing, and face certain challenges due to facial deformity. These problems remain throughout the life if not treated and entail long-lasting effects on the health and social life of an individual. Untreated infants need special care as they have higher morbidity and mortality rates. The primary objective of this study is to detect the Single Nucleotide Polymorphism (SNP) rs2235371 within the IRF6 gene and assess its potential association in patients diagnosed with Non-Syndromic Cleft Lip/Palate (NSCL/P). The participants were selected through a non-probability sampling technique, specifically the purposive sampling method. In accordance with this approach, a total of 50 patients afflicted with NSCL/P, representing both the genders, were sampled. Furthermore, to establish a comparative baseline, an additional 50 healthy individuals were also recruited to serve as the control group. After taking their informed consent, blood was collected in EDTA vials. PCR (Polymerase Chain Reaction) and RFLP were performed on each sample to find SNP. After sample collection, processing, and analysis, SPSS (20.00 version) was used to analyze all previously generated data. After sample analysis, 72% of CL/P (cleft lip and palate) patients were found to have SNP with or without a family history. The association of SNP rs2235371 with disease was measured by applying chi-square. The results provided no evidence of the association between given SNP and disease. As compared to previous research, this study showed a low frequency of SNP rs2235371 in patients with NSCL/P. To get a better understanding of the association of SNP rs2235371 with NSCL/P, large-scale research with an increased sample size should be conducted.
1. INTRODUCTION
Infants born with disorders of facial deformation face various problems throughout their lives, such as communication problems, aesthetic abnormalities, and difficulty in deglutition [1]. These problems remain throughout life if untreated, and can affect the health and social behavior of the individual. These individuals also require special care from early childhood onward and have an increased rate of morbidity and mortality. Multiple surgeries can be performed to treat these patients, such as speech, dental, and other orthopedic treatments during their early childhood [2].
In several countries, CL/P is the major cause of structural birth defects. It is also one of the most common craniofacial abnormalities among children [3].
In CP, the palate shelves do not close enough such that a gap is left unclosed during 2nd month of prenatal life. It is necessary to treat such openings by surgeries otherwise they remain open. The severity of CP varies, ranging from a small fissure in the soft palate to an entire separation of the soft palate. In some cases, the nasal cavity opens into the mouth by extension of fissure through the hard palate. CP can develop in both soft palate or hard palate [4]. CL/P (cleft lip and palate) is characterized as syndromic or non-syndromic. During early embryogenesis, NSCL/P develops due to the failure of palates to fuse during 4-12 weeks.
There are different factors that are considerably involved in the development of CL/P, such as single gene mutation, chromosomal aberration, specific environmental agents, and the interaction of environmental and genetic differences. Moreover, heredity, maternal drug use, maternal diseases, and maternal exogenous exposure to certain conditions are the common risk factors [5]. A mutation in the IRF6 gene and Poliovirus Receptor-Related 1 gene (PVRL1) is also responsible for cleft lip related abnormalities [6]. The mutations in other genes may also cause clefts, such as TP63 and FGFR1 (Fibroblast Growth Factor Receptor 1). Few genes, such as TBX22 (T-box Transcription Factor 22) and PVRL1 are involved in causing X-linked CL/P. In previous research, the IRF6 gene was determined as a candidate gene because of its participation in CL/P and other syndromes. Due to the presence of SNP in the IRF6 gene, the amino acid at position 274 is changed by either valine or isoleucine [7].
Worldwide frequency of CLP is approximately 1/700 in live births. In African populations, the lowest prevalence was reported at about 1/1000, the intermediate prevalence reported in European populations was 1.2/1000, and the Asian population had the highest prevalence rate at about 1/500. This was the highest prevalence ever recorded [8]. Earlier studies showed that the genetic contribution to NSCLP ranges from 12% to 20%. The main concern in CLP is to correct physical defects so that the best possible cosmetic and functional outcomes may be achieved with satisfactory hearing, speech, physical look, orthodontic, and dental wellness. Therefore, multidisciplinary care is required for such children from birth to adulthood [9].
Family history serves as a potent risk factor for the occurrence of Cleft Lip/Palate (CL/P), underscoring the genetic predisposition associated with this condition. Furthermore, consanguineous marriages, while not determinative, can indeed contribute to the development of genetic diseases, including CL/P through the potential amplification of recessive alleles within familial bloodlines [10]. In addition to genetic factors, environmental influences play a crucial role in the etiology of CL/P. Numerous lines of evidence substantiate the significant impact of gene-environment interactions in shaping the occurrence and expression of CL/P. These interactions manifest as a complex interplay between an individual's genetic makeup and external environmental factors, highlighting the multifaceted nature of CL/P development [11, 12].
Following are few maternal factors that cause occurrence of CLP
- Maternal drug use plays a role in the origin of CLP.
- Maternal diseases such as non-gestational diabetes and hyperthermia increase the possibility of having a child with CLP. The risk of congenital malformations has been increased by nutritional deficiencies.
- Maternal vitamin A and B12 deficiencies are also linked with structural birth defects [13].
2. METHODOLOGY
A case-control study design was used to conduct the research. Samples were collected from CLAPP (Cleft Lip and Palate Association of Pakistan) Hospital, Faisal Town, Lahore, Pakistan. The entire process of data collection was performed in the Department of Allied Health Sciences, University of Health Sciences (UHS), Lahore. According to inclusion criteria, blood samples were drawn from 50 patients with NCLP and also from 50 normal healthy individuals. The written informed consent was taken and each participant was asked to complete the questionnaire by providing the details of consanguinity, ethnicity, family history, and others. The samples were drawn from patients by using non probability (purposive) sampling technique. Both genders (male, female) having cleft lip and palate (CL/P) were equally included in this research. After filling out the questionnaire, blood was collected in CBC (complete blood count) vial and kept at -20 °C for further downstream processing and analysis. Patients (male, female) with NSCLP having ages between 1-18 years were involved in the study. However, patients with ages less than 1 year or above 18 years and having any other syndromic characteristics of the disease were excluded from the study.
2.1. DNA Extraction
DNA extraction was carried out on whole blood by using a standard salting out-extraction procedure [14]. In this laboratory procedure, 500 μl of blood was collected into autoclaved 2ml Eppendorf tubes, which were then appropriately labeled. Subsequently, 1000 μl of red blood cells (RBC) lysis buffer was added to each tube. The tubes were securely closed, vortexed, and incubated at 37°C for up to 15 minutes. Following incubation, the tubes underwent centrifugation at 10,000 rpm for 10 minutes to separate the supernatant from the pellets. This washing process was repeated 3 to 4 times, while reducing the lysis buffer volume to 700 μl after the first wash. Next, 10% SDS (30 μl), sodium acetate (400 μl), and proteinase K (13 μl) were added to each tube, thoroughly mixed by inversion, and incubated at 60°C for 1 hour, followed by 24 hours at 37°C. To extract the DNA, 600 μl of ice-chilled chloroform and 1 ml of iso-amyl-alcohol (24:1) were added to each tube after vortexing. After centrifugation at 10,000 rpm, the supernatant was transferred to new marked tubes. Equal volumes of chilled 99% ethanol were added to each tube and centrifuged for 10 minutes at 13,500 rpm. The resulting supernatant was discarded and 70% ethanol (550 μl) was added. This ethanol wash step was repeated twice and the tubes were placed on tissue paper for drying at 37°C. After drying, 50 μl of injection water was added to each tube to dissolve the DNA. In order to deactivate DNase, the tubes were incubated at 65°C for 1 hour. The purified DNA was ultimately stored at -20°C for future use and downstream analysis. This meticulous procedure ensures the isolation and preservation of high-quality DNA samples for research and analytical purposes.
2.1.1 Qualitative and Quantitative Analysis of DNA.
2.1.1.1. Gel Electrophoresis. For detecting isolated DNA from samples, agarose gel electrophoresis was performed [15]. The agarose gel preparation commenced by creating a 1% agarose solution as per the recommended protocol, to which 3μl of ethidium bromide was added. Subsequently, combs were strategically placed on a gel caster plate. The gel electrophoresis tank was filled with 1x Tae buffer and the prepared gel was introduced into the tank. Next, 3μl of the sample was mixed with 2μl of 6x loading dye, consisting of bromophenol blue and xylene along with glycerol and loaded into individual wells. The electrophoresis process was initiated with 150 volts of electric current applied for duration of 40 minutes. Post-electrophoresis, the DNA bands were visualized using a gel documentation system.
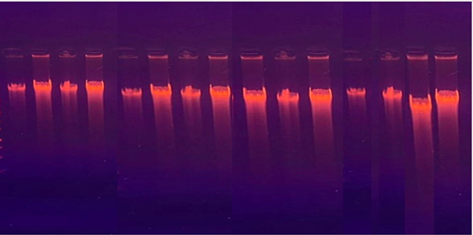
Figure 1. Agarose Gel Electrophoresis Results of Extracted DNAs
For quantitative analysis, 10μl of purified extracted DNA was diluted with 2ml of DNase-free distilled water and the absorbance was measured at 260nm.
2.1.1.2. SNP Selection. The IRF6 SNP rs2235371 was selected according to the db SNP http://www.ncbi.nlm.nih.gov/snp/.
Table 1. SNP Position in the Given Gene
|
No. |
Gene |
db SNP |
Allele |
Position |
NCBI No. |
|
1 |
IRF6 |
rs2235371 |
(C>T) |
Exone |
NG-007081.2 |
2.1.1.3. Primer Designing. By using NCBI (National Center for Biotechnology Information), the sequences of the selected gene were obtained, copied, and saved. Through 50bp upstream and downstream regions, the primers were selected with the help of Primer3Plus (https://blast.ncbi.nlm.nih.gov/Blast.cgi) and SNAP gene bioinformatics tool [16]. For evaluating the specificity of each primer, Primer-BLAST was applied on the designed primers. The sequences of both forward and reverse primers are given below.
Table 2. Primer Sequences
|
No. |
SNP |
Primers |
Sequences |
GC Contents (%) |
Product Size |
|
1 |
rs2235371 |
Forward |
5’- TTCAGTACCGTGGGAAGGAG -3’ |
55 |
995 bp |
|
2 |
Reverse |
5’- TCAGTCTCTGTCCATGACG -3’ |
46 |
2.1.2. Polymerase Chain Reaction (PCR)
2.1.2.1. DNA Amplification. For PCR, Taq polymerase was used along with 2X Master Mix (Thermo Scientific). By using the conventional PCR, 1μl of DNA was amplified. By employing standard optimized conditions, forward and reverse primers of specific gene were used in the reaction. The standardized cycling parameters and reaction mixture are given below.
Table 3. PCR Reaction Mixture
|
Components |
Concentrations |
|
DNA |
1μl |
|
Reverse Primer (10 pm) |
0.5μl |
|
Forward Primer (10 pm) |
0.5μl |
|
Taq Master Mix (2X) |
8 μl |
|
Nuclease Free H2O |
up to 15.0 μl |
The Thermal Cycling Parameters for PCR of rs223537
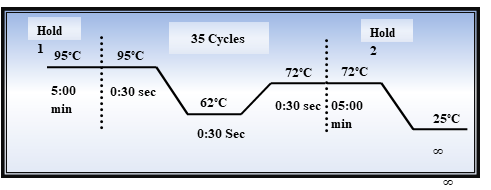
Figure 2. The Optimal Thermal Cycling Condition for PCR
After PCR amplification, the products were analyzed, revealing a product size of 998bp. To verify this size, comparison was made using a 1kb DNA ladder during agarose gel electrophoresis.
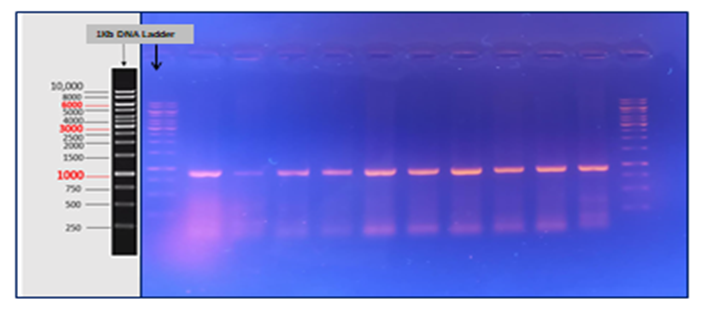
Figure 3. PCR Amplification Product of SNP rs2235371
2.1.2.2. Restriction Fragment Length Polymorphism (RFLP). PCR products were cleaved using restriction enzyme Dpn1. This enzyme specifically recognizes the methylated and, in some way, hemi-methylated sites. Its specificity is reduced in hemimethylated regions of DNA. The restriction site of this enzyme is GA^TC. RFLP was performed by following the protocol reported by Jing [17]. In the presence of a Single Nucleotide Polymorphism (SNP), the restriction enzyme cleaves the PCR amplified product between 625-373bp, resulting in two fragments upon 1% gel electrophoresis. Conversely, if the SNP was absent, the enzyme cutting site was altered, preventing restriction, and a full-length fragment of 998bp was obtained on 2% agarose gel. SNP analysis was conducted based on the number and sizes of cleaved fragments observed on agarose gel electrophoresis.
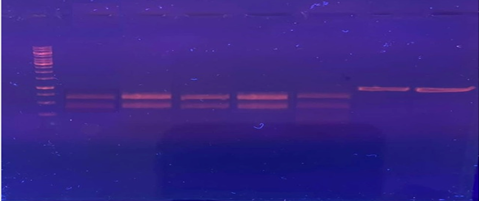
Figure 4. RFLP Digestion of SNP rs2235371
RESULTS
Informed consent from the parents of 50 patients with NSCLP was taken. About 21 (42.00%) of those participants were females and 29 (58.00%) were males. Same number of healthy controls was also involved in this study. The maximum and minimum ages of the subjects lie between 1 to 18 years but most (33%) of the patients were between 2-5 years. As CL/P is treated in early childhood, most of the patients were brought to the hospital at an early age with few exceptions.
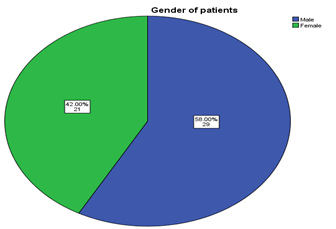
Figure 5. Descriptive Statistics of Patients’ Genders
As many factors are responsible for causing CL/P, genetic elements are also considered one of the key influencers of the disease. The findings showed that 16% of the patients had family history of CL/P and remaining 84% had no family history of malformation. Only a small number of cases were reported in which patients have either their maternal or paternal relatives born with the disease while most of them were new in their family having that specific conditions. NSCL/P is transferred in an autosomal dominant and sometimes autosomal recessive manner. Sample data showed that only a small number of patients had previous family history of NSCL/P. However, none of the patients whose parents suffered from similar conditions in their childhood were identified.
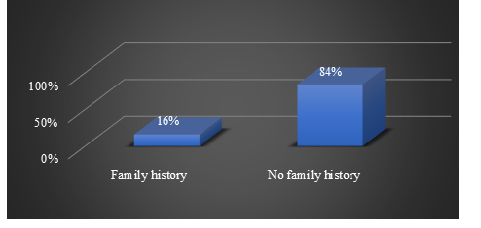
Figure 6. Descriptive Statistics of Family History of CL/P
3.1. Caste of Patients
About 4% of the study’s participants were Malik, 6. % were Jutt, 7% were Arain, 7% were Mughal, 16% were Rajput, and 21% belonged to other various castes from Punjab, Pakistan. The other castes included in this research were Gujjar, Awan, Sheikh, Meo, and others. According to the data, the highest frequencies of NSCL/P were detected in Rajputs and lowest in Jutts. These are the two major castes that are settled in Punjab. Rajput’s have very strict family rituals and consanguineous marriages are considered a source of pride. Therefore, it was found to be one of the key factors of malformation diseases in such families. The same proportion of normal controlled individuals was also included in this study. The caste of the cases and controls are given below in Figure 6.
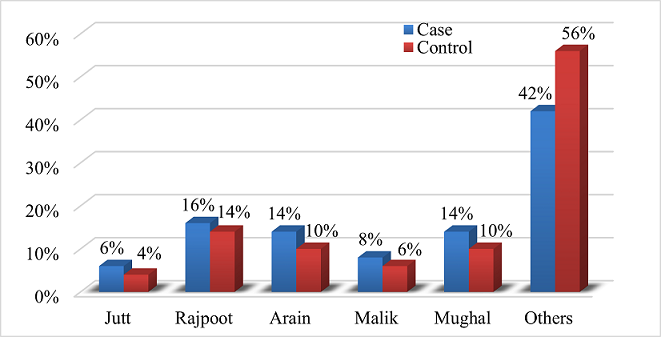
Figure 7. Caste of Cases and Controls Population
3.2. Consanguinity
According to the findings, 80% of patient’s parents have cousin marriages and 20% of the parents have marriages out of their family. Most of the consanguineous couples are married to their first cousins. It has been enlisted earlier that 16% of the subjects belonged to the Rajput family and 14% belonged to Arain and Mughals, collectively. Patients belonging to these castes had consanguineous marriages due to the rigid family approaches toward cousin and inter-caste marriages
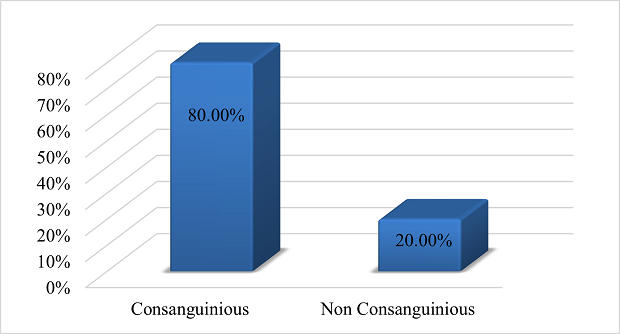
Figure 8. Consanguineous Marriage Statistics
3.3. Cleft Lip and Palate (CL/P) Patients
The current study was conducted on 50 patients of NSCLP, which covered all three forms of CL/P. Out of 50, 11 patients were detected with both Cleft Lip and Palate (CL/P), 17 patients with only Cleft Lip (CL), and 10 patients with only Cleft Palate (CP). The following Table 4 shows the number of occurrences of cleft lip, cleft palate and combined cleft lip and palate among participants.
Table 4. Cleft Lip and Palate
|
Cleft Lip |
Total |
|||
|
Yes |
No |
|||
|
Cleft Palate |
Yes |
11 |
10 |
21 |
|
No |
17 |
12 |
29 |
|
|
Total |
28 |
22 |
50 |
|
3.4. Association of CL and CP with SNP
Out of 28 cleft lip patients, only 17 were detected positive for SNP while the rest was found with no SNP.
Table 5. Association of Cleft Lip with SNP rs2235375
|
SNP |
Total |
|||
|
Present |
Absent |
|||
|
Cleft Lip |
Present |
12 |
16 |
28 |
|
Absent |
5 |
17 |
22 |
|
|
Total |
17 |
33 |
50 |
|
(Chi-square value 1.523 and p value 0.152)
Similarly, the findings also detected 19 patients that had SNP rs2235375 in CP. However, cleft lip and palate showed no significant association with SNPs.
Of the total 50 individuals studied, 17 were found to have SNP. Specifically, within the group of individuals with Cleft Lip (CL), 12 had SNP whereas 16 did not. The statistical analysis, as indicated by the chi-square value of 1.523 and a p-value of 0.152, does not reveal a statistically significant association between the presence of SNP and the occurrence of Cleft Lip. These findings suggested that SNP under investigation may not be a substantial contributing factor to cleft lip in this cohort. However, it is important to note that additional factors, which were not within the scope of this analysis, may play a role in the development of cleft lip.
Table 6. Association of Cleft Palate with SNP rs2235375
|
SNP |
Total |
|||
|
Present |
Absent |
|||
|
Cleft Palate |
Present |
7 |
15 |
22 |
|
Absent |
12 |
16 |
28 |
|
|
Total |
19 |
31 |
50 |
|
(Chi-square value is 3.854 and p value is 0.54)
The above table presents the distribution of SNP occurrences among individuals with and without cleft palate. In the "Cleft Palate" category, 7 individuals were found to have SNP, while 15 individuals did not exhibit SNP, resulting in a total of 22 cases.
Conversely, among those without cleft palate, 12 individuals had SNP, while 16 individuals did not. The overall summary of results indicated that out of 50 individuals, 19 had SNP, while 31 did not demonstrate SNP. The statistical analysis yielded a chi-square value of 3.854 and a corresponding p-value of 0.54. These findings suggest that there is no statistically significant association between the presence of the SNP and the occurrence of cleft palate.
4. DISCUSSION
The non-syndromic clefts are the most common structural birth defects in newborn babies which consist of two groups, CL with or without CP and isolated CP. The infants born with CL/P have slight problems during communication and have beauty challenges and they feel difficulties during swallowing [18]. Health and social integration are also affected by these long-lasting adverse issues. Typically, these children need special care throughout their lifespan and have higher mortality and morbidity than unaffected individuals [19]. Patients with clefts can be divided into three groups according to the principles of Fogh-Adersen and Kernahan and Stark. These include, isolated CL, isolated CP, and combined CL/P. Moreover, they may be further subdivided into unilateral, bilateral, and sub mucous cleft palate [20].
In this study, the gender distribution of the patients was 58% males and 46% females. The ages of all subjects were ranging from 3 months to 18 years. Only 16% of the subjects have inherited the disease from their families. After a comprehensive study, we have found that some of the close relatives of the patients were found with similar conditions [21]. Although this was a very low proportion of relatedness, it can be said on the basis of this that family history is not compulsory for the development of diseases. Only a small proportion of the patients have a family history of disease whereas the majority did not. Only a few maternal or paternal cousins were affected but most of the patients have their distant relatives who were were affected with this disease [22]. A higher disease percentage was calculated among the castes which strictly believe in cousin marriages.
Pearson's chai-square for CL was 1.523 and the p-value was 0.152 and for CP was 3.854 and the p-value for it was 0.54. Whereas, in cleft lip patients, the percentage of SNP was very low. Only 17 patients of CL showed SNP in the IRF6 gene. These results showed that there is no significant association of cleft lip with SNP. It may also be stated that cleft lip can be caused by many environmental factors and not by a single point mutation in the gene. According to the results, 19 patients with cleft palate were detected with SNPs.
Several other studies showed almost similar results while studying different genetic diseases, where consanguineous marriages and inter-caste marriages are common [23]. Similar findings of CLP were found in certain castes where strict family terms are followed [24]. Considerably, SNP rs2235371 were found in all patients of CP except one. The chi-square value and p value are given above for CP and the results showed that there is no significant association of CP with the given SNP. Previous researches have also presented the same results. This signified that the cleft lip and palate may also be developed with or without the contribution of parental carrier genes [25].
Various other studies showed that CL/P is mainly developed from several other environmental factors other than inheritance [26]. In Chinese and Caucasian populations, IRF6 in several SNPs were detected as contributing factors for orofacial clefts [27]. Kung Yee Liang et al. highlighted several gene environmental interactions that were contributing to the NSCLP [28]. However, SNP rs2235371 was found highly significant (p value <0.001) in the Norwegian population but not in the Pakistani population [5]. These contradicted results indicated genetic heterogeneity among different populations.
4.1. Conclusion
In conclusion, the study on non-syndromic clefts provides valuable insights into the prevalence, familial patterns, and genetic associations of such birth defects. The study's findings suggested that while genetic factors may contribute to cleft palate development, environmental factors play a significant role in both cleft lip and palate. The lack of a significant association between the studied SNP (rs2235371) in the IRF6 gene and cleft lip or palate indicated the complexity of these conditions, which are likely influenced by multiple genetic and environmental factors. The study also emphasized on the importance of considering genetic heterogeneity across different populations, as the significance of SNP varied among populations. Overall, this research contributes to the current understanding of non-syndromic clefts and highlights the need for further investigations to unravel the intricate interplay between genetics and the environment in the development of such conditions of malformation. Continued research in this field will help advance prevention, diagnosis, and treatment strategies for individuals affected by cleft lip and palate.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Bibliography
- Yang R, Dong C, Chen Y, et al. Analysis of the clinical features and surgical outcomes of first branchial cleft anomalies. Laryngoscope. 2022;132(5):1008–1014. https://doi.org/10.1002/lary.29896
- Aljohani M, Yates J, Ashley M, O’Malley L. Evaluation of quality of life in adult individuals with cleft lip and/or palate. J Craniomaxillofac Surg. 2021;32(2):505–508. https://doi.org/10.1097/SCS.0000000000007071
- Vinas MJ, Galiotto-Barba F, Cortez-Lede MG, et al. Craniofacial and three-dimensional palatal analysis in cleft lip and palate patients treated in Spain. J Clin Med. 2022;12(1):e18837. https://doi.org/10.1038/s41598-022-23584-0
- Faure JM, Mousty E, Bigorre M, et al. Prenatal ultrasound diagnosis of cleft palate without cleft lip: the new ultrasound semiology. Ultrasound Obstet Gynecol. 2020;40(11):1447–1458. https://doi.org/10.1002/pd.5794
- Nasroen SL, Maskoen AM, Soedjana H, Hilmanto D, Gani BAJD, Problems M. IRF6 rs2235371 as a risk factor for non-syndromic cleft palate only among the Deutero-Malay race in Indonesia and its effect on the IRF6 mRNA expression level. Dent Med Probl. 2022;59(1):59–65. https://doi.org/10.17219/dmp/142760
- Pavlova NI, Diakonova AT, Alekseev VA, et al. Association of the IRF6 rs2235371 and rs861019 polymorphisms with non-syndromic cleft lip with or without cleft palate in the Yakut population. Int J Biomed. 2021;11(4):570–575. https://doio.org/10.21103/Article11(4)_OA28
- Escher PJ, Zavala H, Lee D, Roby BB, Chinnadurai SJTL. Malnutrition as a risk factor in cleft lip and palate surgery. Laryngoscope. 2021;131(6):E2060–E2065. https://doi.org/10.1002/lary.29209
- Salari N, Darvishi N, Heydari M, et al. Global prevalence of cleft palate, cleft lip and cleft palate and lip: a comprehensive systematic review and meta-analysis. J Stomatol Oral Maxillofac Surg. 2022;123(2):110–120. https://doi.org/10.1016/j.jormas.2021.05.008
- Yasin L, Becker M, Svensson H, Wiedel A-P. Long-term patient-reported outcomes after anterior distraction osteogenesis of the maxilla in patients with cleft. J Plast Surg Hand Surg. 2023;57(1-6):488–493. https://doi.org/10.1080/2000656X.2022.2164294
- Beluci ML, Mondini CCdSD, Trettene AdS, Dantas RAS. Correlation between quality of life and burden of family caregivers of infants with cleft lip and palate. Rev Esc Enferm USP. 2019;53:e03432. https://doi.org/10.1590/S1980-220X2017047603432
- Rusdy H, Siregar IB. Cleft lip and palate based on birth order and family history at Mitra Sejati General Hospital, Indonesia. Dent J. 2022;55(4):221–225. https://doi.org/10.20473/j.djmkg.v55.i4.p221-225
- Wright CY, Kapwata T, Wernecke B, et al. The risk of Orofacial Cleft Lip/Palate due to maternal ambient air pollution exposure: a call for further research in South Africa. Ann Glob Health. 2023;89(1):e6. https://doi.org/10.5334/aogh.4007
- Chairunas SHE, Yusuf HY, Riyanti E, Suhanda R, Nandini NJ. Correlation between zinc level of mothers and case of babies with non-syndromic cleft lip and palate. Int J Public Health. 2019;10(11):e1869. https://doi.org/10.5958/0976-5506.2019.03825.7
- Dairawan M, Shetty P. The evolution of DNA extraction methods. J Appl Biotechnol Bioeng. 2020;8(1):39–45. https://doi.org/10.34297/AJBSR.2020.08.001234
- Kasibhatla S, Amarante-Mendes GP, Finucane D, Brunner T, Bossy-Wetzel E, Green DR. Analysis of DNA fragmentation using agarose gel electrophoresis. CSH Protoc. 2006;2006(1):e4429. https://doi.org/10.1101/pdb.prot4429
- Blast. Basic local alignment search tool. Blast Web site. https://blast.ncbi.nlm.nih.gov/Blast.cgi. Accessed January 11, 2024.
- Jing L. Site-directed mutagenesis using Dpn1. Bio-Protocol. 2011;1(3):e29.
- Frederick R, Hogan AC, Seabolt N, Stocks R. An ideal multidisciplinary cleft lip and cleft palate care team. Oral Dis. 2022;28(5):1412–1417. https://doi.org/10.1111/odi.14213
- Ryu JY, Park TH, Cho BC, Choi KY. The prevalence, risk of premature births, mortality and causes of death of cleft lip with or without palate in South Korea: a nationwide population-based cohort study. Int J Environ Res Public Health. 2022;51(3):974–983. https://doi.org/10.1093/ije/dyac019
- Zhu Y, Miao H, Zeng Q, et al. Prevalence of cleft lip and/or cleft palate in Guangdong province, China, 2015–2018: a spatio-temporal descriptive analysis. BMJ Open. 2021;11(8):e046430. https://doi.org/10.1136/bmjopen-2020-046430
- Silva CM, de Moraes Pereira MC, de Queiroz TB, das Neves LT. Can parental consanguinity be a risk factor for the occurrence of nonsyndromic oral cleft? Early Hum Dev. 2019;135:23–26. https://doi.org/10.1016/j.earlhumdev.2019.06.005
- Neela PK, Reddy SG, Husain A, Mohan V. Association of cleft lip and/or palate in people born to consanguineous parents: a 13-year retrospective study from a very high-volume cleft center. J Cleft Lip Palate Carniofac Anomal. 2019;6(1):33–37. https://doi.ord/ 10.4103/jclpca.jclpca_34_18
- Gul M, Nazir G, Saidal A, Bahadar H. Parental consanguinity increases the risk of congenital malformations. Rehman J Health Sci. 2021;3(1):48–51. https://doi.org/10.52442/rjhs.v3i1.81
- Bhatti NA, Mumtaz S, Malik SJ. Epidemiological study of congenital and hereditary anomalies in Sialkot District of Pakistan revealed a high incidence of limb and neurological disorders. Ann Biol. 2019;13(2):49–60. https://doi.org/10.1515/abm-2019-0040
- Xu H, Yan F, Hu R, et al. CleftGeneDB: a resource for annotating genes associated with cleft lip and cleft palate. Sci Bull. 2021;66(23):2340–2342. https://doi.org/10.1016/j.scib.2021.07.008
- de Paula Silva KC, Messias TS, Soares S. The public health importance of flaviviruses as an etiological environmental factor in nonsyndromic cleft lip and/or palate: in silico study. Cleft Palate Craniofac J. 2023;60(5):544–550. https://doi.org/10.1177/10556656221074206
- Mukhopadhyay N, Feingold E, Moreno-Uribe L, et al. Genome-wide association study of non-syndromic orofacial clefts in a multiethnic sample of families and controls identifies novel regions. Front Cell Dev Biol. 22021;9:e621482. https://doi.org/10.3389/fcell.2021.621482
- Gowans LJ, Comnick CL, Mossey PA, et al. Genome-wide scan for parent-of-origin effects in a sub-Saharan African cohort with nonsyndromic cleft lip and/or cleft palate (CL/P). Cleft Palate Craniofac J. 2022;59(7):841–851. https://doi.org/10.1177/10556656211036316