| Review | Open Access |
|---|
Stress, Coping and Premenstrual Dysphoric Disorder in Young Pakistani Female Students |
 |
|---|
![]() Sana Jaffar* , Faiza Safdar, Ayesha Areej, Zainab Khalid, and Tayyaba Sabir
Sana Jaffar* , Faiza Safdar, Ayesha Areej, Zainab Khalid, and Tayyaba Sabir
Center for Clinical Psychology, University of the Punjab, Lahore, Pakistan
The present research aimed to identify the mediating relationship between stress, coping and premenstrual dysphoric symptoms experienced by university students. A correlational research design was employed in this study. Data was collected from 15 different departments of public university. The sample consisted of 300 female students (18 to 25 years, M = 21, SD=1.16) who were experiencing symptoms of Premenstrual Dysphoric Disorder (PMDD). They were selected through purposive sampling. The Student Stress Inventory, Brief COPE and PMDD symptom tracker were employed to measure the perceived stress level, coping strategy, severity of PMDD symptoms in female university students. Correlation and regression analysis were conducted. Results of the study showed a positive relationship between stress and PMDD symptoms. Avoidant coping and PMDD symptoms were found to have a strong relationship. Coping partially mediates the relationship between stress and PMDD symptoms, highlighting its role in reducing symptom severity under high stress levels. Findings suggest that interventions targeting stress management and adaptive coping strategies may help alleviate PMDD symptoms and inform future research on tailored therapeutic approaches.
1. INTRODUCTION
Premenstrual syndrome (PMS) significantly affects women's lives, with almost 75% women experiencing symptoms and approximately 3-8% suffering with severe symptoms (Alwafa et al., 2021). Premenstrual Dysphoric Disorder (PMDD) characterizes the severe psychosocial manifestation of PMS. As per the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2022), PMDD is diagnosed when a woman exhibits at least five symptoms—such as affective lability, irritability, depressed mood, and anxiety—during most menstrual cycles in the previous year. PMDD frequently leads to significant social and functional impairment, which in the long run impact their well-being and quality of life (Akin & Erbil, 2023). It impacts nearly half of women of reproductive age globally, including college students, and is linked to low productivity and quality of life; nevertheless, causes and useful coping strategies are somehow unknown (Eshetu et al., 2022).
Among the various psychosocial factors influencing PMDD, stress plays a precarious role. Stress is a psychological state characterized by emotional tension and pressure, often exacerbated by academic, social, and environmental demands (American Psychological Association, 2015). According to Ijaz et al. (2023), 86.5% of students experience stress due to multiple life pressures. Persistent stress, whether due to external environmental factors or internal cognitive appraisals, can trigger adverse emotional responses, including anxiety and depressive symptoms, which may aggravate PMDD symptoms (Shahsavarani et al., 2015). Research specifies that fluctuations in stress levels across menstrual cycles correlate with variations in symptom severity, with greater stress levels preceding more intense symptoms (Yamamoto et al., 2009).
The theoretical framework of stress encompasses three major perspectives: stress as a response, a stimulus, and a transaction. The response-based model views stress as a physiological and psychological reaction to demands, the stimulus-based model conceptualizes stress as an external life event altering behavior, and the transactional model considers stress as an interaction between an individual and their environment. Within the context of PMDD, stress is best understood as a response that influences both the physical and emotional symptomatology of the disorder. Women experiencing PMDD may perceive their stressors as exceeding their adaptive capacity, resulting in heightened distress and symptom severity (Jones et al., 2018).
Coping mechanisms play a crucial role in mediating the impact of stress on PMDD. Coping strategies can be categorized into problem-focused, emotion-focused, and social coping approaches (Folkman & Moskowitz, 2004). Problem-focused coping, such as active problem-solving and planning, directly addresses the stressor, whereas emotion-focused coping strategies, such as humor, acceptance, and positive reframing aim to mitigate emotional distress (Madhavi & Reddy, 2022). Social coping includes seeking emotional or contributory support from others to manage stress efficiently (Folkman & Moskowitz, 2004). Women with PMDD often rely on various coping mechanisms including relaxation techniques, engaging in pleasurable activities, and social interactions to manage symptoms (Akin & Erbil, 2023). However, avoidant or escape coping is a maladaptive coping strategy that involves trying to avoid a stressful situation (Gupta et al., 2019).
The interaction between stress, coping strategies, and PMDD highlights the need for effective interventions. Cognitive-behavioral therapy (CBT), pharmacological treatments, and lifestyle modifications have shown efficacy in mitigating PMDD symptoms. Moreover, supportive environments and adaptive coping mechanisms can enhance resilience, and reducing the negative impact of stress on PMDD symptoms. As PMDD and PMS impact women’s health significantly, so it is suggested to find its frequency in university students. Also, learn to implement strategies that will help in coping i.e., spending time doing pleasurable activities, positive thinking, distraction techniques, healthy hobbies, increasing physical activates, exercise programs, pain relieving maneuver, and spending quality time with loved ones (Akin & Erbil, 2023).
In conclusion, PMDD is a debilitating condition influenced by multiple biopsychosocial factors, with stress emerging as a significant predictor of symptom severity. Effective coping strategies, social support, and psychological interventions can mitigate the adverse effects of stress, and improve overall well-being. Understanding theoretical linkage between stress, coping mechanisms, and PMDD can aid in developing targeted interventions for affected individuals.
Rationale of the StudyThe premenstrual symptoms that women experience vary in nature, but approximately 90 to 95 percent of women experience some indication of the onset of menstruation. Women's daily ability to function at their best is impaired by these symptoms. Both the frequency and the intensity of premenstrual symptoms are known to be negatively impacted by stress, especially chronic stress. The PMDD symptoms can severely hinder women's overall functioning, including that of female students, who often experience disruptions in academic performance and well-being. According to Delelegn and Getachew (2019), menstruation disorders contribute to around 61.8% of students' regular absences from school and bad grades. Nonetheless, little indigenous research has been conducted in the academic field so far on the relationship between premenstrual symptoms and students' stress levels. Research revealed that the stress caused by luteal phase symptoms rises in response to academic demands such as papers, projects, presentations, and assignments. Students' stress levels skyrocket with time, which has a detrimental impact on their health (Arif, 2013; Pal, 2011). Many students struggle with premenstrual symptoms, but don't know how to cope. This can impact their studies. Let's raise awareness and educate students about this common issue, so they can better manage their symptoms and thrive academically (Kalsoom et al., 2018). Therefore, the current study aimed to to ascertain the level of stress experienced by university students and its effects on their health. To help university students better manage these stressors and enhance their health, this study also sought to evaluate the coping mechanisms associated with academic, interpersonal, physical, and environmental stress on PMDD. This study also helped university administration detect students' stressors more effectively and develop better academic initiatives to reduce stress and improve student’s mental health.
Objectives
- To examine the relationship between stress, coping and premenstrual dysphoric disorder symptoms in university students.
- To find out the mediating role of coping between stress and PMDD symptoms.
Hypotheses
- There is likely to be a significant positive relationship between stress levels and PMDD symptoms in university students.
- Coping is likely to mediate the relationship between stress and PMDD symptoms in university students.
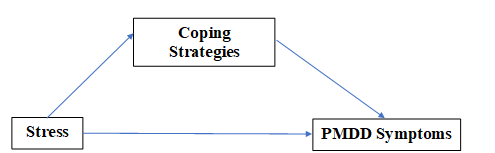
Figure 1
Study Theoretical Model Figure
Method
Research DesignCorrelation research design was used to investigate the relation between stress, coping, and premenstrual dysphoric symptom.
Participants
Sample comprised of 300 young female university students. The participants were taken through purposive sampling, and the mean age was 21. They were from different departments of public university. Participants from undergraduate programs, experiencing some symptoms of PMDD and age between 18-25 years were included.
Table 1
Demographic Characteristics of the Sample (N=300)
|
Variables |
f |
% |
M |
SD |
|---|---|---|---|---|
|
Age |
|
|
20.88 |
1.16 |
|
Birth Order |
|
|
|
|
|
1st Born |
89 |
29.64 |
|
|
|
Middle Born |
145 |
48.23 |
|
|
|
Last Born |
40 |
13.13 |
|
|
|
Only Child |
27 |
9 |
|
|
|
Family System |
|
|
|
|
|
Nuclear Family |
121 |
40.3 |
|
|
|
Joint Family |
179 |
59.7 |
|
|
|
Family Income |
|
|
|
|
|
Less than 20000 |
34 |
11.3 |
|
|
|
21000 to 50000 |
135 |
45 |
|
|
|
More than 50000 |
131 |
43.7 |
|
|
|
Scholar |
|
|
|
|
|
Day Scholar |
172 |
57.4 |
|
|
|
Hostelite |
128 |
42.6 |
|
|
|
Part Time Job |
|
|
|
|
|
Yes |
69 |
23 |
|
|
|
No |
231 |
77 |
|
|
|
Age of Menarche |
|
|
12.98 |
2.21 |
|
Period Days (Cycle) |
|
|
5.58 |
1.58 |
|
Cramps During Menstruation |
|
|
|
|
|
Yes |
231 |
77 |
|
|
|
No |
7 |
2.3 |
|
|
|
Sometimes |
62 |
20.6 |
|
|
|
Strategies Used to Relief Cramps |
|
|
|
|
|
Take Medicines |
85 |
28.3 |
|
|
|
Desi Totky |
50 |
16.6 |
|
|
|
Both |
98 |
32.6 |
|
|
|
Nothing |
67 |
22.3 |
|
|
The socio-demographic sheet was used to get information of participants, i.e., age, socio-economic status, department, family members, birth order, educational level, family system, etc. Information related to sleep patterns, food patterns, menstrual cycle, age of menarche were also asked from participants.
Student Stress InventoryThe Student Stress Inventory (Arip et al., 2015) was used to measure the level of stress among university students. It consists of 40 items, and it has 4 subscales, i.e., Physical, Interpersonal relationship, Academic, and Environmental stress. It has a five-point Likert type scale ranging from 0 (never) to 4 (always). Its alpha reliability coefficient value is 0.85 and subscales have a value of 0.84, 0.80, 0.68, and 0.62 respectively.
Brief COPEThe Coping Orientation to Problems Experienced Inventory is a self-report questionnaire developed by Carver (1997) to measure a broad range of coping responses. It consisted of 28 items that measure 14 factors of 2 items each. Which corresponded to a Likert scale ranging from 0-3. Cronbach’s alpha value of the scale was 0.70.
PMDD Symptoms TrackerPMDD Symptoms Tracker (Eisenlohr-Moul, 2019) was used to assess the premenstrual dysphoric disorder symptoms. It consists of 21 premenstrual symptoms, and it was required to mark the severity of every symptom. It was a 6-point Likert type scale ranging from 1 to 6. It also measured the maladjustment or impairment in the client’s life that was caused by symptoms of PMDD. The Cronbach’s alpha reliability coefficient value was 0.76.
ProcedureThe research was conducted after getting institutional approval from the departmental doctoral committee. The tools were translated and administered only after taking permissions from their respective authors. It was made sure that information given by participants would be kept confidential and used only for research purposes. Consent was taken from the participants to ensure their willingness to participate in research.
The questionnaires were scored according to the instructions given by the authors. After scoring, data was entered. The data analysis was done by using Statistical Package for Social Sciences (SPSS) version 22.0 and by employing procedures of statistical analysis. Reliability analysis was conducted on each scale to get its respective Cronbach’s alpha value. Then, descriptive analysis, frequency, mean, standard deviation, and correlation analysis were carried out.
Results
Pearson product moment correlation coefficient was employed to find out the relationship between Stress, Coping and PMDD.
Table 2
Descriptive Statistics and Reliability Analysis for Study Variables (N=300)
|
Variables |
M |
SD |
k |
α |
Range |
|
|---|---|---|---|---|---|---|
|
Potential |
Actual |
|||||
|
Stress |
|
|
|
|
|
|
|
P.S |
4.6 |
1.67 |
10 |
.90 |
0-40 |
5-38 |
|
R.S |
3.7 |
1.23 |
10 |
.89 |
0-40 |
3-29.4 |
|
A.S |
2.5 |
.65 |
10 |
.91 |
0-40 |
6-36 |
|
E.S |
3.3 |
1.23 |
10 |
.86 |
0-40 |
1-31 |
|
SSI |
4.3 |
1.07 |
40 |
.93 |
0-160 |
55-154 |
|
Coping |
|
|
|
|
|
|
|
A.C |
2.8 |
1.23 |
8 |
.86 |
0-32 |
2-30 |
|
PF.C |
2.6 |
.87 |
8 |
.90 |
0-32 |
3-22 |
|
EF.C |
3.6 |
.68 |
12 |
.87 |
0-48 |
5-45 |
Note. P.S = physical stress, R.S = relationship stress, A.C= academic stress, E.S = environmental stress, SSI= student stress inventory, A.C= avoidant coping, PF.C= problem focused coping, EF.C= emotion focused coping
The above table 2 showed descriptive statistics and reliability analysis of variables. The reliability coefficients for all scales were significant and indicated strong internal consistency.
Table 3
Correlation between Stress, Coping, and PMDD Symptoms in Young Females (N=300)
|
|
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
M |
SD |
|---|---|---|---|---|---|---|---|---|---|---|
|
1.P.S |
.65** |
.48** |
.43** |
.75** |
.43** |
.33* |
.53** |
.29* |
20.60 |
5.18 |
|
2.R.S |
- |
.65** |
.60** |
.86** |
.62** |
.33* |
.62** |
.40** |
21.62 |
5.35 |
|
3.A.S |
|
- |
.66** |
.87** |
.55** |
.23 |
.52** |
.34* |
23.63 |
7.07 |
|
4.E.S |
|
|
- |
.82** |
.62** |
.16 |
.50** |
.24* |
25.94 |
6.13 |
|
5.SSI |
|
|
|
- |
.67** |
.31* |
.65** |
.38** |
91.79 |
19.74 |
|
6. A.C |
|
|
|
|
- |
.23 |
.60** |
.32* |
26.65 |
4.40 |
|
7.PF.C |
|
|
|
|
|
- |
.38** |
.18* |
30.75 |
5.05 |
|
8.EF.C |
|
|
|
|
|
|
- |
.40** |
74.02 |
20.57 |
|
9.PMDD.ST |
|
|
|
|
|
|
|
- |
10.48 |
15.31 |
Note. *p< .05 (two-tailed), **p< .01 (two-tailed). P.S = physical stress, R.S = relationship stress, A.C= academic stress, E.S = environmental stress, SSI= student stress inventory, A.C= avoidant coping, PF.C= problem focused coping, EF.C= emotion focused coping, PMDD.ST= PMDD symptom tracker
Table 3 shows correlation analysis, depicting statistically significant positive relationships between stress, coping, and PMDD symptoms. Academic and relationship stress indicates statistically strongest correlation with PMDD symptoms, while avoidant, emotions focused and problem-focused coping also reveal statistically significant correlation.
Table 4
Hierarchical Regression and Mediation Analysis of Coping Strategies Between Stress and PMDD Symptoms (N = 300)
|
Step / Path |
β |
SE |
t |
p |
95% CI |
R² |
|---|---|---|---|---|---|---|
|
Model 1: Total Effect |
||||||
|
Stress → PMDD Symptoms |
.50 |
.08 |
7.75 |
< .001 |
[.35, .65] |
.25 |
|
Model 2: Mediators (Path a) |
||||||
|
Stress → Avoidant Coping |
.42 |
.06 |
8.00 |
< .001 |
[.30, .54] |
.18 |
|
Stress → Emotion-Focused Coping |
.53 |
.05 |
10.60 |
< .001 |
[.43, .63] |
.28 |
|
Stress → Problem-Focused Coping |
.33 |
.06 |
5.50 |
< .001 |
[.22, .45] |
.11 |
|
Model 3: Path b (Mediators → PMDD) |
||||||
|
Avoidant Coping → PMDD |
.38 |
.07 |
5.71 |
< .001 |
[.26, .54] |
.33 |
|
Emotion-Focused Coping → PMDD |
.40 |
.06 |
6.67 |
< .001 |
[.28, .52] |
.36 |
|
Problem-Focused Coping → PMDD |
.18 |
.07 |
2.57 |
.011 |
[.04, .32] |
.29 |
|
Model 4: Direct + Mediators |
||||||
|
Stress → PMDD Symptoms |
.27 |
.08 |
3.38 |
< .001 |
[.14, .45] |
.39 |
|
Indirect Effects (Bootstrap) |
||||||
|
Stress → A.C. → PMDD |
.16 |
.04 |
— |
< .001 |
[.09, .25] |
— |
|
Stress → EF.C. → PMDD |
.21 |
.04 |
— |
< .001 |
[.14, .30] |
— |
|
Stress → PF.C. → PMDD |
.06 |
.03 |
— |
.015 |
[.01, .13] |
— |
Note. PMDD = premenstrual dysphoric disorder symptoms; A.C. = avoidant coping; EF.C. = emotion-focused coping; PF.C. = problem-focused coping. R² = variance explained; ΔR² = change in variance explained from the previous step. F values represent model significance. Indirect effects tested using 5,000 bootstrap samples.
p < .05, p < .01, p < .001 (two-tailed).
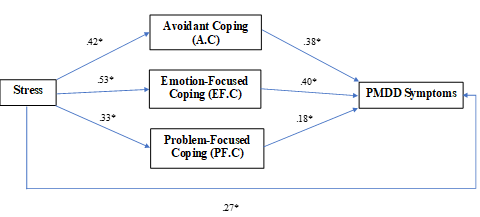
The hierarchical multiple mediation was performed to examine whether avoidant coping, emotion-focused coping, and problem-focused coping mediate the relation between stress and premenstrual dysphoric disorder PMDD symptoms.
It was observed that stress made a significant contribution to PMDD symptoms (.50, p < .001) and explained 25% of the variance (R2 = .25, F (1, 298) = 60.06, p < .001). It also predicted each coping strategy suggestion that an increment in the level of stress was related to a larger application of all the three coping mechanisms and most noteworthy among them was the emotion-oriented coping (.53, p < .001). In addition, coping styles were observed as significant predictors of symptoms of PMDD. After stress was added to the model with coping strategies, the direct effect between stress and PMDD symptoms was reduced, however remained significant (.27, p < .001), reflecting partial mediation. The total model explained 39% of the variance in PMDD symptoms (R2 =.39), and there was a statistically significant increment of 14% in explained variance over Step 1 (ΔR²=.14, F = 47.15, p <.001). Collectively, results suggest that the association between stress and PMDD is in part mediated by coping strategies. These results are indicative of the fact that apart from stress, coping strategies utilized by an individual add further variability to the symptoms of PMDD.
Indirect effects of stress on PMDD symptoms through avoidant coping (p < .001, 95% CI [.09, .25], b =.16), emotion-focused coping (p < .001, 95% CI [.14, .30], b =.21), and problem-focused coping (p =.015, 95% CI [.01, .13], b =.06) were confirmed by bootstrap analyses.
Figure 2
Model Figure of Mediation Analyses
Discussion
The present research intended to investigate the relationship between stress, coping and PMDD symptoms in young university students. Descriptive analysis of present study showed that the number of females expiring PMDD symptoms in university is higher than those in school (Gupta et al., 2019). The reason of this discrepancy is that university population experience more hectic routine as compared to school going female adolescents. Besides exams, university students had to do more assignments and presentations than the adolescent students at schools, this is consistent with previous research which asserts that workload is associated with severity of premenstrual symptoms (Hardy & Hunter, 2021).
Academic stress and physical stress are widely reported by the sample which showed that academic demand distress for assignments, papers and projects/presentations, interpersonal conflict exacerbate the PMDD symptoms in luteal phase. Overall severe levels of stress reported by sample of present research which gives rise to negative emotions like frustrations, pressure, hopelessness, irritability and mood changes and irregularities in menstruation. These findings are supported by previous literature available on PMDD and stress (Ozimek et al., 2022).
For the present research the first hypothesis was to find out the positive relationship between stress and PMDD symptoms. The results showed that stress has a highly significant positive correlation with PMDD symptoms which support the present research hypothesis. Academic stress and physical stress are widely reported by the sample which showed that academic demands, distress for assignments, papers and projects/presentations, interpersonal conflict exacerbate the PMDD symptoms in luteal phase. Women tend to develop more PMDD symptoms when they were already experiencing perceived stress which might affect their academic performance. Overall severe levels of stress reported by sample of present research which gives rise to negative emotions like frustrations, pressure, hopelessness, irritability, and mood changes. These findings are supported by previous literature available on PMDD and stress (Hameed & Fatima, 2022).
In present research, coping also has a high positive correlation with PMDD symptoms. Avoidant coping has high positive correlation while approach coping has moderate correlation with PMDD (Atim et al., 2022). Present research showed that most of the female university students used denial, behavioral disengagement, or the distraction to combat with stress and tension caused by PMDD symptoms, with is consistent with research findings (Ozimek et al., 2022).
The findings of this study indicate that coping partially mediates the relationship between stress and PMDD symptoms. Consistent with previous research, stress was found to be a significant predictor of PMDD symptoms, suggesting that individuals experiencing higher levels of stress are more likely to report severe premenstrual distress (Alwafa et al., 2021). Moreover, coping strategies played a crucial role in moderating this relationship, reinforcing the idea that adaptive coping mechanisms can mitigate the negative impact of stress on psychological well-being (Folkman & Moskowitz, 2004). The significant indirect effect suggests that individuals who engage in effective coping strategies may experience reduced PMDD symptoms, aligning with prior findings that emphasize the importance of coping in managing stress-related health conditions (Akin & Erbil, 2023). Given that maladaptive coping strategies have been linked to poorer mental health outcomes (Gupta et al., 2019), interventions targeting stress management and promoting adaptive coping strategies may be beneficial for individuals experiencing PMDD symptoms. Future research should explore the role of specific coping mechanisms in different populations to further understand their effectiveness in reducing premenstrual distress.
The results also revealed that PMDD symptoms mostly interfere with their routine work, academic performance, and affect their relationships. In present research, 260 out of 300 participants provisionally diagnose to have PMDD, which reflects the burgeoning need to take preventive measure and introduce strategies to reduce the stress of the university students, which will result in better health outcome, Lessing of PMDD symptoms, and efficient performance in all areas of woman’s life. Physical symptoms predominate in the premenstrual experience of the Pakistani women in the present research study and have a significant impact on their daily life activities, which is consistent with previous indigenous research (Pal, 2011).
Conclusion
The study revealed a strong positive relationship between stress and PMDD symptoms in young females. Avoidant coping was strongly associated with greater PMDD symptoms, while approach coping showed a moderate association. Mediation analysis confirmed that coping—particularly avoidant and emotion-focused styles—partially mediated the link between stress and PMDD symptoms. These findings suggest that stress increases PMDD severity, and maladaptive coping strategies amplify this effect, highlighting the need for targeted coping-based interventions.
Limitations and Suggestions
The students enrolled in public university were included in this study. To capture a bigger picture, research with a larger sample size and other universities will be carried out. One vital component influencing PMDD symptoms is quality of life. Studies that concentrate more on life quality can be conducted. The current investigation included a tentative PMDD diagnosis. Better diagnosis and understanding of PMDD can be achieved by directing follow-up studies and daily diary records for symptoms.
Future Implications
This research can help improvise more effective therapy strategies for PMDD in college students. It is more effective to use preventive measures to lessen university students' stress and the negative impacts it has on their health. Better counselling and guidelines can be offered if the reasons, such as stress, that worsen PMDD symptoms and disrupt university students' lives are identified early. Organizing seminars and workshops on PMDD and stress can also help raise student's awareness regarding this condition. Findings suggest that interventions targeting stress management and adaptive coping strategies may help alleviate PMDD symptoms, thereby guiding future research on tailored therapeutic approaches.
Conflict of Interest
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability
The data associated with this study will be provided by the corresponding author upon request.
Funding Details
No funding has been received for this research.
Akın, Ö., & Erbil, N. (2023). Investigation of coping behaviors and premenstrual syndrome among university students. Current Psychology, 43, 1685–1695. https://doi.org/10.1007/s12144-023-04419-1
Alwafa, R. A., Badrasawi, M., & Haj Hamad, R. (2021). Prevalence of premenstrual syndrome in college going girls – A cross-sectional study. BMC Women's Health, 21(1), Article e13746. https://doi.org/10.1186/s12905-021-01374-6
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
American Psychological Association. (2015). Stress in America: A national mental health crisis. https://www.apa.org/news/press/releases/stress/2020/report-october
Arif, A. (2013). Premenstrual syndrome symptoms (PMS) and prevalence among university students in Karachi, Pakistan. International Research Journal of Pharmacy, 4(4), 113–116. https://doi.org/10.7897/2230-8407.04425
Arip, M. M., Kamaruzaman, D. N., Roslan, A., Ahmad, A., Rahman, M. A., & Malim, T. (2015). Development, validity, and reliability of student stress inventory (SSI). The Social Sciences, 10(7), 1631–1638.
Atim, E., Okecho, F. N., Ndagire, R., & Lwanira, C. N. (2022). Effects and coping mechanisms associated with premenstrual syndrome among female university students in Central Uganda: A cross-sectional study. Scientific Journal of Humanities and Social Sciences, 3(9), Article e219. https://doi.org/10.51168/sjhrafrica.v3i9.219
Carver, C. S. (1997). You want to measure coping but your protocol's too long: Consider the brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100.
Delelegn, T., & Getachew, Y. (2019). Premenstrual dysphoric disorder and associated factors among female health science students in Wollo University, Ethiopia. Maternal Health, Neonatology and Perinatology, 5(4), 67–78. https://doi.org/10.1186/s40748-019-0112-2
Eshetu, N., Abebe, H., Fikadu, E., Getaye, S., Jemal, S., Geze, S., Mesfin, Y., Abebe, S., Tsega, D., Tefera, B., & Tesfaye, W. (2022). Premenstrual syndrome, coping mechanisms and associated factors among Wolkite University female regular students, Ethiopia, 2021. BMC Women's Health, 22(1), Article e88. https://doi.org/10.1186/s12905-022-01658-5
Eisenlohr-Moul, T. (2019). Premenstrual disorders: A primer and research agenda for psychologists. The Clinical Psychologist, 72(1), Article e5. https://pmc.ncbi.nlm.nih.gov/articles/PMC7193982/
Folkman, S., & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55, 745–774. https://doi.org/10.1146/annurev.psych.55.090902.141456
Gupta, P., De, N., Hati, S., Saikia, C., & Karmakar, R. (2019). The relationship between positive psychological capital and coping styles: A study on young adults. Psychology, 10(12), 1649–1662. https://doi.org/10.4236/psych.2019.1012109
Hameed, M., & Fatima, M. (2022). The effect of perceived stress and body mass index on premenstrual dysphoric disorder among female university students. Life and Science, 3(4), Article e5. https://doi.org/10.37185/lns.1.1.227
Hardy, C., & Hunter, M. (2021). Premenstrual symptoms and work: Exploring female staff experiences and recommendations for workplaces. International Journal of Environmental Research and Public Health, 18(7), Article e3647. https://doi.org/10.3390/ijerph18073647
Ijaz, M. A., Ijaz, A., & Ijaz, M. M. (2023). Prevalence of anxiety, stress and depression symptoms in university students of south Punjab: Its relationship with socioeconomic factors. Pakistan Journal of Medical Research, 62(3), 112–116.
Jones, P. J., Park, S. Y., & LefeSouthvor, G. T. (2018). Contemporary college student anxiety: The role of academic distress, financial stress, and support. Journal of College Counseling, 21(3), 252–264. https://doi.org/10.1002/jocc.12107
Kalsoom, U., Sultana, A., Amjad, T., & Bairam, S. (2018). Prevalence of premenstrual syndrome and knowledge assessment regarding its prevention among medical students of a private medical college of Islamabad. Pakistan Armed Forces Medical Journal, 68(1), 159–164.
Madhavi, P., & Reddy, B. S. (2022). Appraisal-focused coping style among adolescent girls: Role of anxiety, depression and personality. International Journal of Indian Psychology, 7(3), Article e035. https://doi.org/10.25215/0703.035
Ozimek, N., Velez, K. M., Anvari, H., Butler, L., Goldman, K. N., & Woitowich, N. C. (2022). Impact of stress on menstrual cyclicity during the coronavirus disease 2019 pandemic: A survey study. Journal of Women's Health, 31(1), 84–90. https://doi.org/10.1089/jwh.2021.0158
Pal, A. L. (2011). Premenstrual symptoms in Pakistani women and their effect on activities of daily life. Journal of Pakistan Medical Association, 61(8), 23–35.
Shahsavarani, A. M., Abadi, E. A. M., & Kalkhoran, M. H. (2015). Stress: Facts and theories through literature review. International Journal of Medical Reviews, 2(2), 230–241.
Yamamoto, K., Okazaki, A., Sakamoto, Y., & Funatsu, M. (2009). The relationship between premenstrual symptoms, menstrual pain, irregular menstrual cycles, and psychosocial stress among Japanese college students. Journal of Physiological Anthropology, 28(3), 129–136. https://doi.org/10.2114/jpa2.28.129