| Review | Open Access |
|---|
Premenstrual Symptoms and Sleep Quality among Pakistani Women: The Mediating Role of Interpersonal Relationships and Moderating Role of Emotional Regulation |
 |
|---|
![]() Huma Iqbal1, Hina Rana2, Maryam Hussain3*, and Rabbia Ashraf4
Huma Iqbal1, Hina Rana2, Maryam Hussain3*, and Rabbia Ashraf4
1Lahore School of Behavioral Sciences, University of Lahore, Pakistan
2Department of Clinical Psychology, University of Management & Technology, Lahore, Pakistan
3Department of Psychology, University of Central Punjab, Lahore, Pakistan
4Department of Developmental and Behavioral Pediatrics, The Children's Hospital, Lahore, Pakistan
Research indicates that due to premenstrual symptoms, women experience disturbed interpersonal relationships, adverse emotional regulation, and markedly impaired quality of sleep. The present study aimed to determine the mediating role of interpersonal difficulties and moderating role of emotional regulation between PMS and sleep quality. Urdu translated versions of Premenstrual Syndrome Scale, Emotional Regulation Scale, Interpersonal Difficulties Scale and Pittsburgh Sleep Quality Index were used. Sample size of 115 was selected based on G-Power Analysis. Study found interpersonal difficulties to be partially mediating (β=.02, p<.05) and emotion regulation (suppression) to be moderating (β= -.004, p<.05) between PMS and sleep quality. Furthermore, it was found that the effect of PMS on sleep quality remains significant at lower suppression levels. The study has important implication in understanding the role of psychological factors in improving sleep quality of females experiencing PMS.
1. INTRODUCTION
Premenstrual Syndrome (PMS) was first proposed by Green and Dalton in 1953 as a wide diagnostic concept, characterized by recurring symptoms during the premenstrual or initial days of menstruation in women, which are completely invisible after the menstrual cycle. PMS is one of the most common disorders in the women who are in reproductive age, and it has a negative effect on women’s emotions and performance (Zendehdel & Elyasi, 2018). Women experience mood swings due to hormonal changes during PMS, which may include anger and irritability (Saglam & Basar, 2019). It is a general term which includes a wide array of behavioral, emotional, and physical symptoms that start occurring from several days to several weeks before menses and disappear after the period (Freeman, 2003). PMS includes a mixture of psychological and physical signs that occur before and during menstrual cycle, females who suffer are commonly affected during the luteal phase of their menstrual cycle (1 to 2 weeks), with symptoms diminishing towards the end of menstruation (Biggs & Demuth, 2011; Cheng et al., 2013).
Research indicates that due to premenstrual symptoms, women experience disturbed interpersonal relationships, adverse emotional regulation, psychological issues and markedly impaired quality of sleep which may cause them to be socially isolated (Abay & Kaplan, 2019).
A meta-analysis was conducted on 9147 reproductive-aged women. The study took place in Iran and the overall prevalence of PMS was estimated to be 54.9 % using a random effect model, out of which 80.4 % were school students, and 68.9% university students (Ranjbaran et al., 2017). A study conducted in Kabul, Afghanistan during the year 2021 found that most of the (88.8%) participants screened positive for either moderate or severe PMS (27.1%) or PMDD (61.7%). There was a significant association between lower educational achievement and higher rates of PMS/PMDD (Ezadi et al., 2025). A study by Kalsoom et al. (2018) found the prevalence of PMS in 280 (80%) students. Out of them, (95%) experienced physical changes such as breast tenderness; (75%) experienced psychological changes such as depression; (43%) showed behavioral changes whereas, the most commonly prevailing effect was bon academic performance (76%). Statistically significant association was found between knowledge regarding presence and prevention of PMS.
Emotion regulation, a form of emotional self-control, shares a common neural substrate with motor inhibitory control. It is also a form of self-control, which overlaps and share some common cognitive features (Petersen et al., 2016). Emotional regulation is concerned with three unique aspects of the emotional response, named as: the experiential component, meaning the subjective feeling of the emotion; the behavioral component, meaning behavioral reactions; and the physiological component, meaning physiological responses, such as (heart rate and respiration).
Evidence shows that during PMS or PMDD, women had mood issues, depression and irritability as compared to the premenstrual phase. Habitual emotion regulation may have an influence on an individual’s well-being and performance in emotion experience task whereas opposite and positive effects were found due to habitual use of reappraisal (Wu et al., 2016). Hormonal changes (notably in estrogen and progesterone) affect neurotransmitters like serotonin and GABA, which are central to mood stability and emotional control. Women with PMS often experience increased emotional reactivity and difficulty regulating emotions (e.g., impulsivity, sadness, irritability). These emotional dysregulations are more pronounced in Premenstrual Dysphoric Disorder (PMDD), a severe subtype of PMS.
Further literature reveals that complexity with emotion regulation may be related to the severity of PMDD symptoms. Women with PMDD are more impulsive, with greater problem in regulating emotion and in socioemotional functioning (Petersen et al., 2016).
Interpersonal relationships are defined as social relations, connections, or affiliations between two or more persons. Interpersonal relationships vary in their degree of closeness, but also in their duration, and in their power distribution, to name only a few dimensions. Familial relationships, friendships, and marriage, as well as relationships with associates, employment, neighborhoods, and places of religion form the basis of social groups and of society (Ye & Ye, 2020).
Interpersonal relationships may be disrupted by the physical, psychological, and behavioral aspects of premenstrual syndrome (Gümüşsoy et al., 2021). Irritability, emotional lability, headache, anxiety, depression, and physical symptoms such as edema, weight gain, mastalgia, and syncope are all signs of PMS. Distress, interpersonal relationship disruption, and everyday function disruption result from these symptoms (Karimiankakolaki et al., 2019). The last 14 days of the menstrual cycle, from ovulation to the start of menstruation, are severe enough to cause interpersonal relationships to deteriorate and regular activities to be disrupted (Fiebai et al., 2018).
Sleep is necessary for a person’s physical and mental health. Although individual sleep requirements vary, most adults require roughly seven hours of sleep on a regular basis to maintain optimal health (Jehan et al., 2016).
A systematic review (Nexha et al., 2024) in BMC Women’s Health found that during PMS/PMDD women consistently exhibit lower melatonin secretion, elevated nocturnal body temperature, and worse subjective sleep quality. Sleep disturbances are common due to PMS, across the life cycle of women. The quality and quantity of sleep can be impacted by internal hormonal variations in pregnancy, postpartum, perimenopause, vasomotor symptoms. The occurrence of sleep issues related with menstruation was reported as 55% effect on the quality of life of women. Women of all ages 18–50, during the premenstrual week report more disturbed sleep, such as increased sleep onset latency, more awakenings, and lower sleep efficiency. In the luteal phase, compared to the follicular phase, there was a decrease in slow wave sleep and and increase in stage 1 sleep, according to studies (Karaman et al., 2012).
Considering the evidence-based (Gümüşsoy et al., 2021; Nexha et al., 2024) relationships between the aforementioned variables, the current study hypothesized that emotional regulation is likely to moderate while interpersonal relationship is likely to mediate between premenstrual symptoms and quality of sleep in women.
Figure 1
Hypothesized Model of Mediation and Moderation
Method
Research DesignCross sectional research design was employed.
Sample SizeSnowball sampling was used for data collection. Sample size was calculated through G-Power Analysis and existing literature, which gave a sample size of 115. The mode of data collection was online, using Google forms.
Participant CharacteristicsMean age of the study participants was 24.26 (SD = 2.22). 96.5% participants were sampled through the province of Punjab and 3.5% from the province of KPK, Pakistan. 59.1% participants belonged to nuclear family system whereas 40.9% lived in a joint family system. The education of the participants was divided into the following four categories: Under matric, matric, Intermediate, BA/BS, and MA/MPhil. The frequency (percentages) of the participants was: 1(.9), matric 3(2.6), Intermediate, 12(10.4), BA/BSc, 35(30.4), MA/MSc/BS (Hons.), 49(39.1), and MS/MPhil, 18(15.7). The duration of PMS experienced by participants was divided into three categories, which were 1 - 6 months, 7 - 12 months and 1-3 years. Their frequency and percentages are 51(44.3), 21(18.3) and 18(15.7) respectively.
MeasuresTo ascertain cultural appropriateness, Urdu translated versions of the following scales were used: Premenstrual Syndrome Scale (PMSS) [40 items, α= .81], (Padmavathi et al., 2014); the researchers themselves translated this tool. The translations of the rest of the tools including Emotional Regulation Scale [10 items, α= .73] (Gross & John, 2003), Interpersonal Difficulties Scale [61 items, α= .87] (Saleem et al., 2014) and Pittsburgh Sleep Quality Index (PSQI) [19 items, α= .91] (Buysse et al., 1989) were adapted. It took almost 40 to 45 minutes for participants to fill out the questionnaire protocol. Details of the tools are provided underneath:
Demographic SheetDemographic information sheet was devised by the researcher through a self-design to gather participant’s personal information which includes age, family system (joint or nuclear), religion, city, qualification and other personal information.
Premenstrual Syndrome Scale (PMSS)PMSS was devised by Padmavathi et al. (2014) and consisted of 40 items with three dimensions (physiological, psychological and behavioral symptoms), using 5- point Likert type scale for response and scoring. Inter-rater reliability of that tool lies between .81 and .97. Formal permission was obtained from the author for its usage and translating it in Urdu Language. The reliability of this tool on the current data was .92.
Emotional Regulation Questionnaire (ER)Emotional regulation scale (Gross & John, 2003), is a 10-item scale that assesses a respondents’ ability to regulate their emotions on two sub domains; reappraisal and suppression. Person’s response for every item is calculated on a 7-point Likert-type rating ranging from 1 (strongly disagree) to 7 (strongly agree). Reliability of that scale was 0.73 to 0.82. In present study, Cronbach’s Alpha of that scale was .70 on the current data. Formal permission was obtained from the tool’s original author and also the author who translated this tool (Saeed & Rana, 2019).
Interpersonal Relationships (IR)Indigenous scale of interpersonal relationship scale was developed by Saleem et al. (2014), having a standardized measure in Urdu version (the national language of Pakistan) with Cronbach Alpha (.87). The scale has six factors, which include: dominated by others, low self-confidence, mistrust, lack of assertiveness, lack of boundaries and unstable relationship. Each item is rated on five points Likert scale (from not at all, to always) having 0-4 respectively by the participants. In the present study Cronbach Alpha of that scale was .95.
Pittsburgh Sleep Quality Index (PSQI)The PSQI is a self-administered questionnaire with 19 self-rated questions for subjective sleep quality evaluation. PSQI measures seven sleep quality categories, including subjective sleep quality, sleep latency, length, efficiency, disturbance, medication, and daytime dysfunction, to assess sleep quality of the individuals. Each component is scored from 0 to 3, with higher scores indicating a lower quality of sleep and a global sum of PSQI score greater than “5” indicating a poor sleeper (Daniel, 1989). The original internal consistency reliability of the tool was 0.91 whereas reliability on the current study data was .60. Formal permission was obtained from the tool’s initial author and also the author who translated this tool (Farooq & Rana, 2017).
ProcedureStudy procedures and ethical considerations were approved by the graduate committee of a private university of Lahore, Pakistan. Permission from the authors of the scales was also sorted before data collection. Online Google form was prepared for data collection. This link was spread in the community via different social media sites. Data was collected in 1 ½ month. Total participants (N=115) completed the online Google form who fulfilled the inclusion criteria. It was made sure to avoid any violation of ethical considerations. Formal permission from research ethical committee of Department of the University was taken for conducting the research. Permission to use and translate the tool was taken from their respective authors. All participants provided consent prior to participating. Confidentiality and privacy of participants was maintained. Participants’ volunteered participation was ensured in research.
Results
Pearson product moment correlation shows relationship between all study variables, with reference to subscales and composite scores (see Table 1).
Table 1 highlights that premenstrual syndrome and its subscales show positive relationships with interpersonal relationship and sleep quality indicators, suggesting that increased symptom severity is associated with greater interpersonal difficulties and poorer sleep outcomes. Emotional regulation through reappraisal exhibits weak or negative associations with interpersonal factors and sleep quality, indicating that reappraisal may not strongly influence these outcomes. Similarly, suppression in emotional regulation shows minimal relationships with other variables. Interpersonal relationship factors, such as being dominated by others, low self-confidence, mistrust, and lack of boundaries, are positively related to poorer sleep quality indicators, this showed that interpersonal difficulties may contribute to sleep issues.
Table 1
Pearson Product Moment Correlation among Emotion Regulation, Interpersonal Relationship and Quality of Sleep in Women Premenstrual Symptoms (N=115)
|
Variables |
1 |
2 |
3 |
4 |
5 |
|---|---|---|---|---|---|
|
1.Premenstrual syndrome |
- |
-.02 |
.12 |
.67*** |
-.32*** |
|
2. ER Reappraisal |
- |
- |
.51*** |
-.19 |
-.12 |
|
3. ER suppression |
- |
- |
- |
-.07 |
.03 |
|
4 Interpersonal relationship |
- |
- |
- |
- |
.33*** |
|
5.Global sleep |
- |
- |
- |
- |
- |
Note. PMS= Premenstrual Syndrome, ER= Emotional Regulation *p<.05. **p<.01. ***p<.001.
Table 2
Relationship Between Premenstrual Syndrome and Sleep Quality, with Interpersonal Relationship as a Mediator and Suppression as a Moderator Of the path from Premenstrual Syndrome to Interpersonal Relationship
|
Model |
Outcome Variable |
Predictor |
B |
SE |
p |
LLCI |
ULCI |
|---|---|---|---|---|---|---|---|
|
Model 1 |
Interpersonal Relationship |
(Constant) |
-23.5 |
12.76 |
.07 |
-48.91 |
1.73 |
|
|
Premenstrual Syndrome |
1.05 |
0.11 |
.00 |
0.84 |
1.26 |
|
|
R2 |
|
.46 |
|
|
|
|
|
|
F(1, 113) |
|
95.86 |
|
<.001 |
|
|
|
|
Model 2 |
Sleep Quality |
(Constant) |
-6.17 |
4.41 |
.16 |
-14.93 |
2.55 |
|
|
Interpersonal Relationship |
0.02 |
0.02 |
.25 |
-0.02 |
0.06 |
|
|
|
Suppression |
0.58 |
0.26 |
.03 |
0.06 |
1.10 |
|
|
|
Int_1 |
-0.00 |
0.00 |
.03 |
-0.01 |
-0.00 |
|
|
R2 |
|
.17 |
|
|
|
|
|
|
F(4, 110) |
|
5.65 |
|
<.001 |
|
|
|
|
Conditional Effects of Premenstrual Syndrome on Interpersonal Relationship at percentile value of Suppression |
|
|
|
|
|
|
|
|
12.00 |
|
0.04 |
0.02 |
.02 |
0.01 |
0.08 |
|
|
18.00 |
|
-0.01 |
0.02 |
.42 |
-0.05 |
0.02 |
|
|
21.00 |
|
0.00 |
0.02 |
.98 |
-0.04 |
0.04 |
|
|
Indirect Effect |
|
|
0.02 |
0.01 |
|
0.00 |
0.04 |
Note. W values in conditional tables are the 16th, 50th, and 84th percentiles. Int_1 = Premenstrual Syndrome × Suppression (interaction term).
Hayes' Process Model 5, was used to investigate the relationship between Premenstrual Syndrome (PMS) and Sleep Quality, mediated by Interpersonal Relationships and moderated by Suppression.
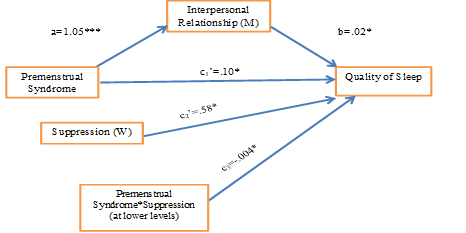
The first step of the analysis revealed that Premenstrual Syndrome significantly positively predicted Interpersonal Relationships. In the second step, both Interpersonal Relationships (B=0.02, p<.001) and Suppression (B=0.58, p<.001) emerged as significant positive predictors of sleep quality. Moreover, the interaction between PMS and Suppression also significantly predicted Sleep Quality, indicating a moderating effect.
Furthermore, the analysis of the conditional effects indicated that the relationship between Premenstrual Syndrome and Interpersonal Relationship was significant and positive only at lower levels of Suppression, specifically, at the 16th percentile of Suppression,
Finally, the indirect effect of Premenstrual Syndrome on Sleep Quality through Interpersonal Relationships was found to be significant. This suggests that Interpersonal Relationship mediates the association between Premenstrual Syndrome and Sleep Quality, although the strength of this mediation is dependent on the level of Suppression (see Figure 2).
Figure 2
Emerged Model of Mediation and Moderation
Note. Direct and indirect effect of Premenstrual Syndrome, Interpersonal Relationship and interaction effect of Premenstrual Syndrome and Emotional Regulation (Suppression) on Quality of Sleep.
The findings of this research showed that PMS is one of the most common disorders among women of reproductive age, and it has a negative effect on women's emotions and performance (Zendehdel & Elyasi, 2018). Premenstrual symptoms like sadness, anger, irritability, bloating may appear with hormonal fluctuating. Changes in hormonal level cause an increase in negative emotions and women had difficulty to regulate their mood (Liu et al., 2017). When fluctuation in emotions is resolved, symptoms of PMS decrease (Panahi et al., 2016). Premenstrual symptoms may affect interpersonal relationships and daily life functions (Karimiankakolaki et al., 2019). Sleep trouble was also an issue of premenstrual syndrome according to different studies, due to a decrease in melatonin production owing to hormonal changes during luteal phase of the menstruation. Poor sleep creates the disturbance in circadian rhythm that creates disturbance in women’s moods. Women could have different problems due to poor sleep; they might be sleepy in daytime and have poor concentration in activities (Ghaffarilaleh et al., 2019). Previous studies mostly focused on prevalence rate of premenstrual syndrome in Pakistan. Unfortunately, in Pakistan premenstrual issues have increased in society because women have less awareness about premenstrual symptoms and do not have enough knowledge about how to deal with problem that occur during menstruation period. So, the present study was to determine the relationship among emotional regulation, interpersonal relationship, and quality of sleep in women with premenstrual symptoms.
The present study hypothesized that emotional regulation is likely to moderate while interpersonal relationship is likely to mediate between premenstrual symptoms and quality of sleep in women. Results found significant relationship (mediated and moderated by psychological factors) between premenstrual symptoms and quality of sleep. Recent evidence found that PSQI (high scores show poor sleep quality) has positive relationship with PMSS and its sub domains, showing that changes in sleep pattern as the strong predictor, followed by depressive thoughts and mood, bloating and high score on PMSS (Erbil & Yücesoy, 2020). This paved the path to study the psychological factors that could be responsible in aggravating the relationship so that therapies can be designed targeting specifically those. Literature suggests that interpersonal communication and perception regarding it can be a crucial factor in the model. Similarly, a recent preprint published by Tang et al. (2019) suggests that participants scoring low on sleep quality experienced higher interpersonal sensitivity. Therefore, the present study took interpersonal difficulties as a possible mediator. Our mediation hypothesis showed partial mediation, proving that interpersonal difficulties may play a role, leaving room for other variables to be studied as potential mediators.
PMS symptoms, regardless of any age, are caused by extreme hormonal fluctuation and since hormones play a crucial role in emotional regulation, the age difference will make little to no difference. Our moderation hypothesis proposed that emotional regulation, specifically suppression, will moderate the relationship between premenstrual symptoms and quality of sleep. Study results found that indeed it works as a moderator between the two, confirming the result of prior studies, such as that by Vafapoor et al. (2018). A similar study by Meers et al. (2020) confirm our findings showing that severity of the depressive symptoms significantly predicts higher PMS with poor sleep and inability to regulate emotions as mediator. The cause could be that poor sleep enhance the experience of PMS indirectly effecting physical, cognitive, and/or affective functioning. On the other hand, an inability to regulate emotions may intensify perception and experience of somatic and mood symptoms during the premenstrual period.
Our study brings to light an interesting finding wherein the effect of PMS on sleep quality remains significant at lower suppression levels only. This might be due in part to the fact that the less a person suppresses emotion, the more these emotions engage their thoughts, thereby keeping sleep at bay. However, this is a finding that needs to be confirmed with more scientific evidence to be established as reliable.
Overall, study found significant relationships between PMS and quality of sleep. Results also found that interpersonal relationships partially mediate and emotional regulation moderates the relationship between PMS and quality of sleep.
Implications
There are many girls and women who experience PMS symptoms at least at some point in their lives. This study can help psychologists and general practitioners understand the debilitating quality of life these symptoms can lead to and intervene accordingly. Our study identified two of the most crucial psychological factors as intervening variables, as literature suggested, but their meager relationships show that other psychological factors must be explored in future studies. Furthermore, the data and studies mostly depict the western statistics. More awareness with regards to female hormonal cycle and PMS must be made available indigenously through educational and awareness programs.
Suggestions and Future Recommendations
While studies have taken into account many psychological factors playing a crucial role in the relationships between PMS and sleep, however, future researchers are encouraged to study on the same lines to determine the precise role of interpersonal difficulties and emotion regulation as intervening variables. The present study also considers that the relationship difficulty is largely ‘perceived’ in nature, therefore some tool around relationship sensitivity or perceived difficulty can be incorporated in future research.
Conflict of Interest
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability
The data associated with this study will be provided by the corresponding author upon request.
Funding Details
No funding has been received for this research.
Abay, H., & Kaplan, S. (2019). Current approaches in premenstrual syndrome management. Bezmialem Science, 7(2), 150–156. https://doi.org/10.14235/bas.galenos.2018.2358
Biggs, W. S., & Demuth, R. H. (2011). Premenstrual syndrome and premenstrual dysphoric disorder. American Family Physician, 84(8), 918–924.
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213. https://doi.org/10.1016/0165-1781(89)90047-4
Cheng, S. H., Shih, C. C., Yang, Y. K., Chen, K. T., Chang, Y. H., & Yang, Y. C. (2013). Factors associated with premenstrual syndrome—A survey of new female university students. The Kaohsiung Journal of Medical Sciences, 29(2), 100–105. https://doi.org/10.1016/j.kjms.2012.08.017
Erbil, N., & Yücesoy, H. (2020). Relationship between premenstrual syndrome and sleep quality among nursing and medical students. Perspectives in Psychiatric Care, 58(2), 448–455. https://doi.org/10.1111/ppc.12628
Ezadi, Z., Ramozi, M., Barati, H., Hosseini, M., Hakimi, S., Mohammady, N., Ozaki, A., Kotera, Y., Kaneda, Y., Ramozi, P., & Bek, B. (2025). Prevalence and associated factors of premenstrual syndrome among female university students of the reproductive age group in Kabul, Afghanistan: A cross-sectional study. Women's Health Reports, 6(1), 403–411. https://doi.org/10.1089/whr.2024.0106
Fiebai, P., Ukueku, A. O., & Ogu, R. (2018). Pre-menstrual syndrome. In O. I. Lutsenko (Ed.), Menstrual cycle (pp. 43–66). IntechOpen.
Farooq, A., & Rana, H. J. (2017). Sensitivity, fatigue, sleep disturbance and quality of life in Migraine Sufferer (Unpublished master thesis). University of Lahore, Pakistan.
Freeman, E. W. (2003). Premenstrual syndrome and premenstrual dysphoric disorder: Definitions and diagnosis. Psychoneuroendocrinology, 28, 25–37. https://doi.org/10.1016/s0306-4530(03)00099-4
Ghaffarilaleh, G., Ghaffarilaleh, V., Sanamno, Z., Kamalifard, M., & Alibaf, L. (2019). Effects of yoga on quality of sleep of women with premenstrual syndrome. Alternative Therapies in Health and Medicine, 25(5), 40–47.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
Gümüşsoy, S., Dönmez, S., & Keskin, G. (2021). Investigation of the relationship between premenstrual syndrome, and childhood trauma and mental state in adolescents with premenstrual syndrome. Journal of Pediatric Nursing, 61, Article e65–e71. https://doi.org/10.1016/j.pedn.2021.04.022
Jehan, S., Auguste, E., Hussain, M., Pandi-Perumal, S. R., Brzezinski, A., Gupta, R., Attarian, H., Jean-Louis, G., & McFarlane, S. I. (2016). Sleep and premenstrual syndrome. Journal of Sleep Medicine and Disorders, 3(5), Article e1061.
Kalsoom, U., Sultana, A., Amjad, T. & Bairam, S. (2018). Prevalence of premenstrual syndrome and knowledge assessment regarding its prevention among medical students of a private medical college of Islamabad. Pakistan Armed Forces Medical Journal, 68(1), 159–64.
Karaman, H. I. O., Tanriverdi, G., & Degirmenci, Y. (2012). Subjective sleep quality in premenstrual syndrome. Gynecological Endocrinology, 28(8), 661–664. https://doi.org/10.3109/09513590.2011.650769
Karimiankakolaki, Z., Mahmoodabad, S. S. M., Heidari, F., Gerayllo, S., & Khabiri, F. (2019). The relationship between premenstrual syndrome and women's marital satisfaction. Journal of Midwifery and Reproductive Health, 7(2), 1630–1635. https://doi.org/10.22038/jmrh.2019.33287.1361
Liu, Q., Wang, Y., van Heck, C. H., & Qiao, W. (2017). Stress reactivity and emotion in premenstrual syndrome. Neuropsychiatric disease and treatment, 13, 1597–1602. https://doi.org/10.2147/NDT.S132001
Meers, J. M., Bower, J. L., & Alfano, C. A. (2020). Poor sleep and emotion dysregulation mediate the association between depressive and premenstrual symptoms in young adult women. Archives of Women's Mental Health, 23(3), 351–359. https://doi.org/10.1007/s00737-019-00984-2
Nexha, A., Caropreso, L., de Azevedo Cardoso, T., Suh, J. S., Tonon, A. C., & Frey, B. N. (2024). Biological rhythms in premenstrual syndrome and premenstrual dysphoric disorder: A systematic review. BMC Women's Health, 24(1), Article e551. https://doi.org/10.1186/s12905-024-03395-3
Padmavathi, M. P., Sankar, D. R., Kokilavani, D. N., Dhanapal, K., & Ashok, B. (2014). Validity and reliability study of Premenstrual Syndrome Scale (PMSS). International Journal of Advances in Nursing Management, 2(1), 4–10. https://doi.org/10.5958/2454-2652
Panahi, F., & Faramarzi, M. (2016). The effects of mindfulness-based cognitive therapy on depression and anxiety in women with premenstrual syndrome. Depression Research and Treatment, 2016, Article e9816481. https://doi.org/10.1155/2016/9816481
Petersen, N., London, E. D., Liang, L., Ghahremani, D. G., Gerards, R., Goldman, L., & Rapkin, A. J. (2016). Emotion regulation in women with premenstrual dysphoric disorder. Archives of Women's Mental Health, 19(5), 891–898. https://doi.org/10.1007/s00737-016-0634-4
Ranjbaran, M., Samani, R. O., Almasi-Hashiani, A., Matourypour, P., & Moini, A. (2017). Prevalence of premenstrual syndrome in Iran: A systematic review and meta-analysis. International Journal of Reproductive BioMedicine, 15(11), 679–686.
Saeed, F., & Rana, H. (2019). Emotional regulation, conflict regulation and quality of life in doctors (Unpublished master thesis). University of Lahore, Pakistan.
Saglam, H. Y., & Basar, F. (2019). The relationship between premenstrual syndrome and anger. Pakistan Journal of Medical Sciences, 35(2), 515–520. https://doi.org/10.12669/pjms.35.2.232
Saleem, S., Ihsan, Z., & Mahmood, Z. (2014). Development of interpersonal difficulties scale for university students. Pakistan Journal of Psychological Research, 29(2), 277–297. https://doi.org/10.1037/t54691-000
Tang, H., Guo, B. & Lang, Y. (2019). Research between sleep quality and interpersonal sensitivity of Chinese college students. Research Square. https://doi.org/10.21203/rs.3.rs-73546/v1
Vafapoor, H., Zakiei, A., Hatamian, P., & Bagheri, A. (2018). Correlation of sleep quality with emotional regulation and repetitive negative thoughts: A casual model in pregnant women. Journal of Kermanshah University of Medical Sciences, 22(3), Article e81747. https://doi.org/10.5812/jkums.81747
Wu, M., Liang, Y., Wang, Q., Zhao, Y., & Zhou, R. (2016). Emotion dysregulation of women with premenstrual syndrome. Scientific Reports, 6(1), 1–10. https://doi.org/10.1038/srep38501
Ye, J., & Ye, X. (2020). Adolescents' interpersonal relationships, self-consistency, and congruence: Life meaning as a mediator. Social Behavior and Personality: An International Journal, 48(11), 1–11. https://doi.org/10.2224/sbp.9428
Zendehdel, M., & Elyasi, F. (2018). Biopsychosocial etiology of premenstrual syndrome: A narrative review. Journal of Family Medicine and Primary Care, 7(2), 346–356. https://doi.org/10.4103/jfmpc.jfmpc_336_17