
| Review | Open Access |
|---|
Knowledge, Attitude, and Practice Related to Renal Diet in Hemodialysis Patients: An Analysis of the Impact of Socioeconomic Status on KAP |

|
|---|
![]() Aiza Talat1*, Ribaha Javaid1, Umm-e-Habiba1, Faiza Kamal2, and Ayesha Jamshaid1
Aiza Talat1*, Ribaha Javaid1, Umm-e-Habiba1, Faiza Kamal2, and Ayesha Jamshaid1
1University of Management and Technology, Lahore, Pakistan
2Avista CLG, Dublin, Ireland
Hemodialysis patients require major modifications in their behavior and dietary pattern for catering to their health complications. Slight inaccuracies in diet and practices can create severe complications for patients including overhydration, hyperkalemia, and phosphorus excess. Patients must have adequate knowledge to maintain the optimum balance of minerals and dry weight. The objective of the study was to assess the dietary knowledge of hemodialysis patients and compare it with their attitudes and practices. Also, to examine the effect of socioeconomic status on knowledge, attitudes and practices (KAP). For this purpose, data was collected from 6 different hospitals across Lahore that include Hijaz Hospital, Jinnah Hospital, Bahria International Hospital, Indus Hospital, Services Hospital, and Skyline welfare trust. The target population included the hemodialysis patients both males and females with no specification regarding race or ethnicity. Convenience sampling was employed to gather data from available dialysis patients. The result’s analysis reported that out of 306 participants, 54.9% were male and 16.1% were female. Gender comparison demonstrated that males exhibited more favorable attitudes than females. Analysis of the KAP questionnaire revealed that 64.4% of patients had good knowledge, while 77.4% demonstrated a positive attitude. In conclusion, the study reveals that the socioeconomic status of most patients marked significant differences in their level of knowledge and attitude, however, practices remain unaffected from socioeconomic status. Education appears to have a strong correlation with good knowledge about renal diet, whereas attitudes and practices are independent of it.
1. INTRODUCTION
Dialysis is an artificial method used to purify the blood of patients suffering from kidney failure, defined as glomerular filtration rate below 15ml per min. It’s is also termed as end stage renal disease. It can be managed only through dialysis or kidney transplantation. Since transplantation is a more complex procedure so more patients opt for dialysis. A decrease in kidney function results in fluid retention, protein-energy malnutrition (PEM), anemia, dyslipidemia, and disturbance of bone metabolism [1].
Studies have revealed that the main causes of end-stage renal disease include hypertension, diabetic nephropathy, glomerulonephritis, ischemic renal disease, Interstitial nephritis, polycystic kidney disease, and obstruction of the urinary tract due to stones, etc. [2]. Hypertension is considered one of the common causes of ESRD, different researches suggest a strong connection between high blood pressure and ESRD [3].
Hemodialysis is an external procedure which purifies the blood by the removal of urinary retention products through a dialyzer. The use of dialyzers in clinical practice has emerged over time and is now controlled by devices with high-performance levels. This method was introduced by Willem Kolff and Belding Scribner in 1943 [4]. In peritoneal dialysis the blood is cleansed inside the body without assistance of the dialyzer. Catheter is inserted in peritoneum (lining of the abdomen). During the procedure, abdomen is filled with dialysate. Dialysate is a purifying fluid that pulls out the waste product and then it is drained out through the catheter. This procedure was first done on patients in 1959 [5].
This research article explored the knowledge, attitudes, and practices (KAP) related to the diet of hemodialysis patients. Adherence to renal diet and liquid limitation is perceived to be a pivotal factor in promoting the well-being of patients who lose amino acids through dialysis. It is compulsory for ensuring survival of the patient [6].
Energy requirements for dialysis patients vary when considering the health status and the age of the individuals. The energy requirement for dialysis patients under 60 years is 35 kcal/kg per day. However, the energy requirement is reduced to 30 kcal/kg per day for patients above 60 years [7]. Protein requirement is very crucial for the sustenance of the patients which is 1.2 g of protein/kg per day [8]. It is advised to limit the consumption of red meat since it can cause increased acid load and uremic toxins [9]. The recommended ranges for phosphorus are 0.8-1.2g/day, potassium less than 3 g/day, salt less than 2.3g per day, and calcium restriction up to less than 1200mg/day [7]. Water intake should be 750-1000ml per day add urine output.
Researches recommend a low intake of potassium, phosphate, and sodium. However, diet must be balanced to maintain electrolyte balance. Phosphate binders are advised to every patient, as negligence in its intake can cause phosphorus retention as a result of increased intestinal absorption compared to excretion from the kidney [10]. Phosphorus load is a critical parameter in all stages of CKD and dialysis. Patients need to be educated about low phosphorus protein ratio diet [11]. The mechanism to control its overload is based on dietary choices by switching to boiling vegetables, limiting phosphorus-laden foods, and additives having phosphorus [12].
The recommended potassium intake for healthy adults is 4700mg/d, while hemodialysis patients can have 2000-3000 mg per day. Meanwhile, restricting potassium and phosphorus from the diet of dialysis patients can also lead to deficiencies in these essential minerals. For catering to this concern, the limitation of the minerals should be profoundly planned. Additionally, a phosphorus restricted diet can affect the heart health of the patients [13].
2. MATERIALS AND METHODS
Subjects were informed about the study and verbal consent was taken, which included the volunteer's declaration and confidentiality of their details. Verbal consent was taken from all patients before filling out the questionnaires. It took approximately 20-25 minutes to record the responses of each patient. The demographics of these patients were also recorded in an information form.
A cross-sectional study was conducted to evaluate the knowledge, attitude, and practice of hemodialysis patients related to their dietary habits using a validated close ended questionnaire. 306 subjects filled out the questionnaire for research purposes. Data were collected from 6 different hospitals across Lahore, including Hijaz Hospital, Jinnah Hospital, Bahria International Hospital, Indus Hospital, Services Hospital, and Skyline Welfare Trust. The data was collected from dialysis patients of all age groups and genders by using convenience sampling of non-probability.
The target population of the study comprised hemodialysis patients, both males and females with no specification of race or ethnicity. A correlational approach was used for this study that observed whether patients had the knowledge about the renal diet. Moreover, their attitudes and practices of dialysis in relation to the knowledge they had were also assessed. Data collection took place over 2 months (July and August 2021), while the overall study duration was four months.
Tools employed were the KAP questionnaire that was created by following a validated KAP questionnaire for hypertensive patients [14] and the Kuppuswamy scale for socioeconomic scale [15]. Questionnaire subjects were selected by the criteria:
- Diagnosis of Stage III/IV from the past 1 year or before.
- Adults >30yrs of age.
- GFR <15.
306 was the sample size which was calculated by using this method [16]:
S = z2 x p (1 – p) / M2
Where S = sample size, z = z-score = confidence level 92%
P = Population Proportion (50%)
M = Margin of error = 0.05
2.1. Statistical AnalysesStatistical analyses were conducted using standard SPSS software– Statistics Package for Social Science. One-way ANOVA was also performed. Additionally, to analyze the effect of knowledge on attitude, knowledge on practices, and attitude on practices Pearson’s correlation was performed on KAP variables.
3. RESULTS
Table 1. Frequency and Percentages of Males and Females Participated in Research
|
|
Frequency |
Percent |
Cumulative Percent |
|
|---|---|---|---|---|
|
Male |
168 |
54.9 |
54.9 |
|
|
Female |
138 |
45.1 |
100.0 |
|
|
Total |
306 |
100.0 |
|
|
Table 2. Frequency and Percentages of Education of Patients Participated in Research
|
|
Frequency |
Percent |
Cumulative Percent |
||
|---|---|---|---|---|---|
|
Illiterate |
28 |
9.2 |
9.2 |
||
|
Primary school |
7 |
2.3 |
11.4 |
||
|
Middle school |
22 |
7.2 |
18.6 |
||
|
High school |
36 |
11.8 |
30.4 |
||
|
Intermediate/ Diploma |
61 |
19.9 |
50.3 |
||
|
Graduate |
77 |
25.2 |
75.5 |
||
|
Professional degree |
75 |
24.5 |
100. |
||
|
Total |
306 |
100.0 |
|
||
Table 3. Frequency and Percentages of Occupation of Patients Participated in Research
|
|
Frequency |
Percent |
Cumulative Percent |
|
|---|---|---|---|---|
|
Unemployed |
35 |
11.4 |
11.4 |
|
|
Unskilled worker |
6 |
2.0 |
13.4 |
|
|
Semiskilled worker |
21 |
6.9 |
20.3 |
|
|
Skilled worker |
42 |
13.7 |
34.0 |
|
|
Clerical/Shop/Farm |
53 |
17.3 |
51.3 |
|
|
Semi professional |
81 |
26.5 |
77.8 |
|
|
Professional |
68 |
22.2 |
100.0 |
|
|
Total |
306 |
100.0 |
|
|
Table 3 indicates that the highest percentage of respondents were semi-professional and the least percentage of respondents were unskilled. In addition to semi-professionals, clerical workers and professionals were higher in percentage.
Table 4. Frequency and Percentages of Income of Patients Participated in Research
|
|
Frequency |
Percent |
Cumulative Percent |
|
|---|---|---|---|---|
|
Less than 2390 |
26 |
8.5 |
8.5 |
|
|
Rs.2391-7101 |
9 |
2.9 |
11.4 |
|
|
Rs.7102-11836 |
7 |
2.3 |
13.7 |
|
|
Rs.11837-17755 |
32 |
10.5 |
24.2 |
|
|
Rs.17756-23673 |
60 |
19.6 |
43.8 |
|
|
Rs.23674-47347 |
95 |
31.0 |
74.8 |
|
|
Rs.47348 and above |
77 |
25.2 |
100.0 |
|
|
Total |
306 |
100.0 |
|
|
The scale used for categorization of socioeconomic class is the Kuppuswamy scale. This scale gives scoring related to socioeconomic status of a person based on their relevant education, occupation and income. In this scale, individuals scoring between 25-29 belong to the upper class, whereas those scoring between 16-25 belong to the upper middle class. Individuals with scores of 11-15 have socioeconomic status of lower middle class and those scoring between 5 and 10 are upper lower-class individuals. Below 5 scale shows lower socioeconomic class.
Table 5. Frequency and Percentages of Different Socioeconomic Classes
|
|
Frequency |
Percent |
Cumulative Percent |
|||
|---|---|---|---|---|---|---|
|
lower class |
17 |
5.6 |
5.6 |
|||
|
lower middle |
32 |
10.5 |
16.0 |
|||
|
upper class |
53 |
17.3 |
33.3 |
|||
|
upper lower |
31 |
10.1 |
43.5 |
|||
|
upper middle |
173 |
56.5 |
100.0 |
|||
|
Total |
306 |
100.0 |
|
|||
This table indicates that 5.6% of the participants belonged to the lower class, 10.5% were from the lower middle class, and 17.3% identified as upper class. Additionally, 10.1% were classified as upper lower class and majority of the participants (56.5%) were from upper middle class.
Figure 1 Bar chart showed the frequency of attitude of patients participating in research. When the gender comparison was done it was observed that males exhibited more favourable attitudes than females.
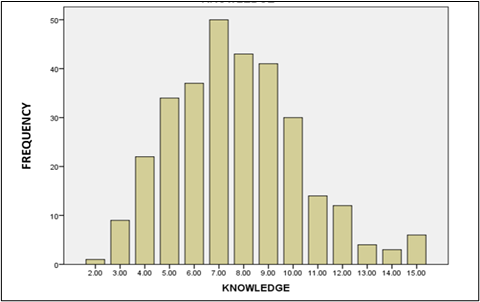
Figure 1. Frequency of Knowledge of Patients
Minimum marks were 0. Maximum marks were 15. Poor scorer: the patient who scored < 7. Good scorer: the patients who scored 7 or > 7.
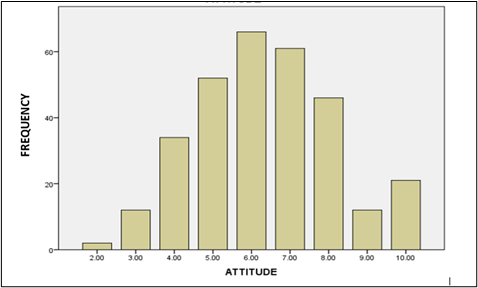
Figure 2. Frequency of Attitude of Patients
Minimum marks were 0. Maximum marks were 15. Poor scorer: the patient who scored < 7. Good scorer: the patients who scored 7 or > 7.
Figure 2 represents a bar chart illustrating the frequency of practice among patients participating in the research. The analysis indicates that individuals with a strong understanding of a renal-specific diet tend to have positive attitudes, which in turn positively influences their practices.
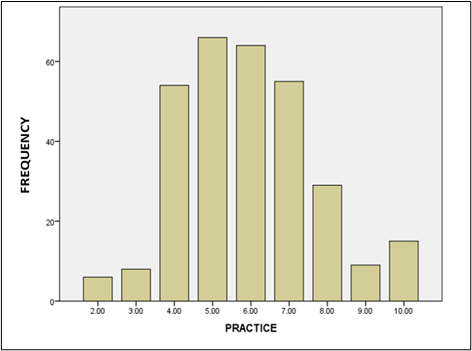
Figure 3. Frequency of Practice of Patients
Minimum marks were 0. Maximum marks were 15. Poor scorer: the patient who scored < 7. Good scorer: the patients who scored 7 or > 7.
Table 6. Correlation between Knowledge, Attitude, and Practice
|
Variable |
Correlation coefficient |
p-value |
|---|---|---|
|
Knowledge-attitude |
0.343 |
0.000 |
|
Knowledge-practice |
0.232 |
0.000 |
|
Attitude-practice |
0.136 |
0.017 |
Table 6 presents Pearson's correlation between knowledge and attitude, showing a significance level of 0.000. Thus, they are positively significant with Pearson's correlation (r) equal to 0.343. Pearson's correlation between knowledge and practice with a significance level of 0.000. So, they have positively correlated with Pearson’s correlation equal to 0.232.
Pearson's correlation between attitude and practice with a significance level of 0.017 shows they are positively correlated with Pearson’s correlation which is equal to 0.136. Hence, it indicates that participants having good knowledge had good attitudes and good practices.
Table 7. Correlation between Knowledge, Attitude, Practice, and Socioeconomic Class
|
Variable |
Correlation coefficient |
p-value |
|---|---|---|
|
Knowledge-socioeconomic class |
0.189 |
0.001 |
|
Attitude- socioeconomic class |
0.056 |
0.331 |
|
Practice- socioeconomic class |
0.038 |
0.512 |
Table 7 indicates that knowledge and socioeconomic class are positively correlated whereas altitude and practice showed no correlation with socioeconomic class. As for socioeconomic class and knowledge, Pearson's correlation is positively significant with a significance level of 0.001. Pearson's correlation of socioeconomic class with attitudes and practices was not correlated and not significant proved by a significance level of 0.33 and 0.512 respectively. This suggests that upper-class patients exhibited high knowledge but attitudes and practices were not correlated to socioeconomic class.
Table 8. Correlation of KAP Variables with Education, Occupation, and Income
|
Variable |
Correlation coefficient |
p-value |
|---|---|---|
|
Knowledge-education |
0.126 |
0.028 |
|
Knowledge-occupation |
0.138 |
0.016 |
|
Knowledge-income |
0.178 |
0.002 |
|
Attitude-education |
0.022 |
0.700 |
|
Attitude -occupation |
0.103 |
0.072 |
|
Attitude-income |
0.027 |
0.643 |
|
Practice-education |
-0.029 |
0.617 |
|
Practice -occupation |
0.013 |
0.827 |
|
Practice-income |
0.087 |
0.127 |
Table 8 indicates that Pearson's correlation between education and knowledge is positively significant and shown by a significance level of 0.02. Whereas Pearson's correlation of education with attitude and practice is not correlated as shown by the significance level of 0.7 and 0.6 respectively.
Additionally, Pearson's correlation between occupation and knowledge is positively significant and shown by the significance level of 0.01. However, Pearson's correlation of occupation with attitude and practice is not correlated as shown by the significance level of 0.7 and 0.8 respectively.
Pearson's correlation between income and knowledge is also positively significant and shown by the significance level of 0.02. However, Pearson's correlation of occupation with attitude and practice is not correlated as shown by the significance level of 0.643 and 0.12 respectively.
4. DISCUSSION
The results of this study strongly imply that end-stage renal disease is more prevalent in men than in women within the targeted population. In a relevant study in which KAP of renal diet was assessed among hemodialysis patients, the results declared sex of the participants as an independent factor [17].
The results demonstrated that lower socioeconomic status is related to low levels of education which in turn leads to reduced knowledge of dietary practices and increased risk of complications and diseases. When a relevant study about the risks of chronic diseases was checked it was found that out of different parameters of socioeconomic status, education appears to mark a significant difference in knowledge, attitude, and practices, and findings of that study revealed that a lower level of education is linked with a higher risk of chronic diseases [18].
Data analysis revealed that around 21 patients achieved the maximum score of 10 which means their general attitude toward renal diet is much better than others. The results clearly illustrate the patients' attitudes toward dietary guidelines and practices, with most of the population demonstrating a positive attitude toward diet in renal disease. Gender comparisons indicated that males exhibited more favourable attitudes than females. In a comparative study, it was observed that different psychological and physiological factors play a significant role in the attitude of renal patients. These factors are also responsible for the knowledge and adherence of patients to their practices [18].
This research article emphasizes that knowledge has a direct impact on the practices and attitudes of the participants. Likewise, in a corresponding study, it was reported that poor knowledge among participants led to poor practices.
4.1. Limitations- Due to COVID-19 restrictions, dialysis wards were not easily accessible due to various risk factors, resulting in a reduced sample size. For this purpose, the confidence interval was decreased from 95% to 92%. When the confidence interval was 95% the calculated population sample was 395 – 400 patients but later when the confidence interval was 92% the population sample size calculated was 306 dialysis patients. Additionally, the Nephrology department of many hospitals did not permit visits to the dialysis ward.
- Reporting bias also caused hurdles while filling out the questionnaire. Patients heard each other and changed their answers accordingly.
- Many patients refused to cooperate and were reluctant to engage in the study. Family members often attempted to answer questions on behalf of patients, limiting the opportunity for patients to express their own views.
- Access to patient files and necessary information was restricted by ward management, which could have affected the comprehensiveness of the data.
Initially, it was assumed that hemodialysis patients may not have good dietary practices in Lahore. However, the analysis of the results surprisingly revealed that most of the hemodialysis patients have good knowledge of renal diet, maintain a positive attitude towards it, and their practices also fall in the good category. This study also reveals that the socioeconomic status of most patients marked significant differences in their level of knowledge and attitude, however, practices remain unaffected by socioeconomic status. Furthermore, education appears to have a strong relationship with good knowledge about renal diet, whereas attitude and practice are independent of it.
CONFLICT OF INTEREST
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
DATA AVAILABILITY STATEMENT
The data associated with this study will be provided by the corresponding author upon request.
FUNDING DETAILS
No funding has been received for this research.
REFERENCES
- Iyengar SK, Freedman BI. Renal failure, chronic. In: Lang F, ed. Encyclopedia of Molecular Mechanisms of Disease. Springer; 2009:1823–1828. https://doi.org/10.1007/978-3-540-29676-8_349
- Banaga ASI, Mohammed EB, Siddig RM, et al. Causes of end stage renal failure among haemodialysis patients in Khartoum State/Sudan. BMC Res Notes. 2015;8:e502. https://doi.org/10.1186/S13104-015-1509-X
- Elmorshedy H, Aziz EMA, Elmorshedy HA, Abd-Elkader AS, Haridi MA. Causes of end stage renal disease in patients undergoing regular hemodialysis in Assiut University Hospital. Sapporo Med J. 2021;55(12).
- Ye H, Ding H, Gan W, et al. Hemodialysis. In: Yang J, He W, eds. Chronic Kidney Disease: Diagnosis and Treatment. Springer Nature; 2020:209–231. https://doi.org/10.1007/978-981-32-9131-7_17
- Andreoli MCC, Totoli C. Peritoneal dialysis. Rev Assoc Med Bras. 2020;66(1):s37–s44. https://doi.org/10.1590/1806-9282.66.S1.37
- Hendriks FK, Smeets JSJ, Broers NJH, et al. End-Stage renal disease patients lose a substantial amount of amino acids during hemodialysis. J Nutr. 2020;150(5):1160–1166. https://doi.org/10.1093/jn/nxaa010
- Ikizler TA, Burrowes JD, Byham-Gray LD, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kid Dis. 2020;76(3):S1–S107. https://doi.org/10.1053/j.ajkd.2020.05.006
- Garcia-Torres R, Young L, Murray DP, Kheda M, Nahman NS. Dietary protein source and phosphate levels in patients on hemodialysis. J Ren Nutr. 2020;30(5):423–429. https://doi.org/10.1053/j.jrn.2019.11.006
- Mafra D, Borges NA, Cardozo LFM de F, et al. Red meat intake in chronic kidney disease patients: Two sides of the coin. Nutrition. 2018;46:26–32. https://doi.org/10.1016/j.nut.2017.08.015
- Mahan K, Escott-Stump S, Raymond J. Krause’s Food and the Nutrition Care Process. Elsevier; 2012.
- Li J, Wang L, Han M, et al. The role of phosphate-containing medications and low dietary phosphorus-protein ratio in reducing intestinal phosphorus load in patients with chronic kidney disease. Nutr Diabet. 2019;9(1):1–10. https://doi.org/10.1038/s41387-019-0080-2
- Dwyer JP, Kelepouris E. New directions in phosphorus management in dialysis. J Ren Nutr. 2023;33(1):12–16. https://doi.org/10.1053/j.jrn.2022.04.006
- Sanghavi S, Whiting S, Uribarri J. Potassium balance in dialysis patients. Semin Dial. 2013;26(5):597–603. https://doi.org/10.1111/sdi.12123
- Mahajan H, Kazi Y, Sharma B, Velhal GD. Assessment of KAP, risk factors and associated co-morbidities in hypertensive patients. IOSR J Dent Med Sci. 2012;1(2):6–14.
- Modified Kuppuswamy scale. I Hate PMS Web site. https://ihatepsm.com/blog/modified-kuppuswamy-scale. Accessed December 09, 2023.
- Sample Size Formula. Cuemath Web site. https://www.cuemath.com/sample-size-formula/. Accessed December 9, 2023.
- Kanagarajah S, Velraja S, Arambakkam H. Knowledge, attitude, and practices of renal diets among hemodialysis patients. Biomed Biotechnol Res J. 2022;6(1):86–92. https://doi.org/10.4103/BBRJ.BBRJ_200_21
- Parvan K, Hasankhani H, Seyyedrasooli A, Riahi SM, Ghorbani M. The effect of two educational methods on knowledge and adherence to treatment in hemodialysis patients: clinical trial. J Caring Sci. 2015;4(1):83–93. https://doi.org/10.5681/jcs.2015.009