Zil e huma1, Mehwish Khalid2*, Arooj Fatima1, Hassan bin Akram3, Zehra Zaman1, Mehran Basat4
1Lahore College of Physical Therapy, LMDC, Pakistan
2Department of Physical Therapy, Lahore University of Biological and Applied Sciences
3Department of Physiotherapy Ghurki Trust Teaching Hospital, Lahore, Pakistan
4Inner Mongolia University for The Nationalities, China
* Corresponding Author: [email protected]
To evaluate the changes in the medial longitudinal arch of the foot in the third trimester of pregnancy among multiparous women, A Cross-sectional observational study was conducted. Women of age 18-30 in 34-38 gestational weeks were included. Those women who were nulliparous, primiparous, flat foot prior to pregnancy, and had undergone through abortion were excluded from the study. The sample was collected by using non-probability purposive sampling and analyzed by SPSS (Statistical Package for Social Sciences). Navicular drop test of the left foot was 36.4% negative and 63.6% positive, whereas for the right foot it was 52.7% negative and 47.3% positive. The study results indicated that the changes in the medial longitudinal arch of the left foot were more evident as compared to the right foot.
Keywords: medial longitudinal arch, multiparous, pregnancy, third trimester
The medial longitudinal arch of the foot is formed with the medial part of the calcaneus, talus, and cuneiform, along with the first, second, and third metatarsal bones. It consists of an anterior pillar made up of talus, navicular, and three cuneiforms, along with first, second, and third metatarsal bones, and a posterior pillar formed by the medial half of the calcaneus. The medial longitudinal arch was higher than the other arches of the foot, which has resilience and shock-absorbing properties [1].
The process of changes that take place in women's organs and tissues as a result of developing fetus in utero is called pregnancy. The entire process from fertilization to birth take an average 266-270 days or about nine months [2].
The foot arches are made up of bones, ligaments, and tendons, which are necessary for the production of movement and weight bearing. The foot is composed of three arches, including a transverse arch, medial longitudinal arch, and lateral longitudinal arch. These arches provide stability, flexibility, and propelling forces during weight bearing and gait [3].
Various biomechanical, anatomical, and hormonal changes occur in women's foot structure during the pregnancy. The weight gain during pregnancy can lead to a flat foot due to a decrease in medial longitudinal arch height, which is caused due to additional loading on the planter surface and a shift of the mass toward the rear of the feet to offset mass of the fetus. decrease in arch also occurs due to increased production of the hormone relaxing, which causes an increase in ligamentous laxity [4].
There is an increase in the total length, front length, and width of the foot, and an increase in the angle of inclination of the first and fifth phalanges. These changes can lead to an increase in foot pronation [5]. There is an increase in pressure on the first metatarsophalangeal joint and the height of the head of the talus, which leads to the pronation of the foot and lateralization of gait. Foot pain, increased sagittal pelvic tilt, and a more posterior head position occur due to biomechanical changes that usually occur during pregnancy [6].
The incidence of arch collapse is 9:1 in females and males, respectively. Only 11.1% of non-obese women who were noticed to be pregnant more than once experienced a change in arch of the foot [7].
Musculoskeletal changes are evident in multiparous women, such as weight gain an average of 10 to 12 kg, change in stance width, increase steps time, decrease in stride length, increase laxity of spring ligament, increase in tibial rotation at knee joint, and cramping pain of gastrocnemius complex [8].
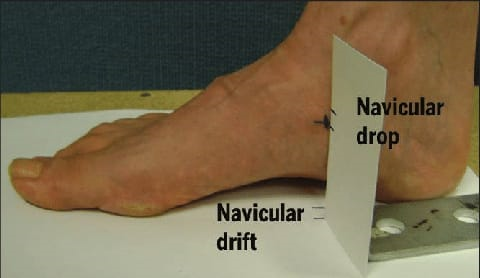
Navicular height was measured to evaluate the drop in the medial longitudinal arch of the foot by using the navicular drop test in both sitting and standing positions. Navicular bone height was measured with respect to the subtalar joint and the observed distance between navicular tuberosity and ground surface in both standing and sitting positions was marked. The difference in both measurements was a drop in the medial longitudinal arch of the foot. Normal difference is 6-8mm, difference > 6-8mm indicated a drop in the medial longitudinal arch of the foot [3].
The prevalence of flat foot in males was 12.8% and for female was 14.4%. The correlation of right navicular drop was significant with height and weight but insignificant with BMI while left navicular drop was insignificant with height, weight and BMI. During pregnancy arch of foot flattens and this persist in puerperium [9].
Arch height and rigidity significantly decreased, with concomitant increase in foot length and arch drop. First pregnancy most significantly have reduction in arch rigidity and arch drop and lead to musculoskeletal changes in women [10].
Women's foot were assessed by using their foot print and pain intensity by using numerical rating scale.57.2% and 59.9% of pregnant women have low arch height in right and left foot respectively. Lower back pain was more common than knee and foot pain. This study also conclude that there is no relation of foot arch height with foot, knee and back pain [11].
2.1. Study Design and Sample size
A Descriptive cross-sectional study was conducted on 55 multiparous women.
2.2. Study Duration and Sample Calculation Method
The study duration was six months after approval of the title (from July 2022 to December 2022).
2.3. Sample Calculation Method
Sample size was calculated by the census method.
2.4. Study Settings
The study settings were Ghurki Trust Teaching Hospital and Lady Wallington Hospital, Lahore.
2.5. Ethical Approval
It was approved by the Ethical Review Committee of LCPT (Lahore College of Physical Therapy).
Multiparous women of gestational weeks 34-38, of age 18-30 were included and the confidentiality of every patient was maintained.
2.6. Sampling Technique
It was non-probability purposive.
2.7. Exclusion Criteria
Women who were nulliparous, primiparous, obese, had persistent bleeding, trauma, and congenital foot deformity that were excluded from this study.
2.8. Test for Data Collection
Standard navicular drop test was used to measure the medial longitudinal arch. Navicular drop test's intra-rater reliability is 0.94 and inter-rater reliability is 0.91[12].
2.9. Statistical Analysis
Data analysis was done by using SPSS v.26. The study variables were presented in the form of descriptive statistics, such as tables, graphs, and percentages.
The details can be seen in the table below, which represent the frequency and percentage of the right foot navicular drop test.
Table1. Navicular Drop Test of Right Foot
|
Frequency |
Percentage |
|
|
Negative |
29 |
52.7 |
|
Positive |
26 |
47.3 |
|
Total |
55 |
100 |
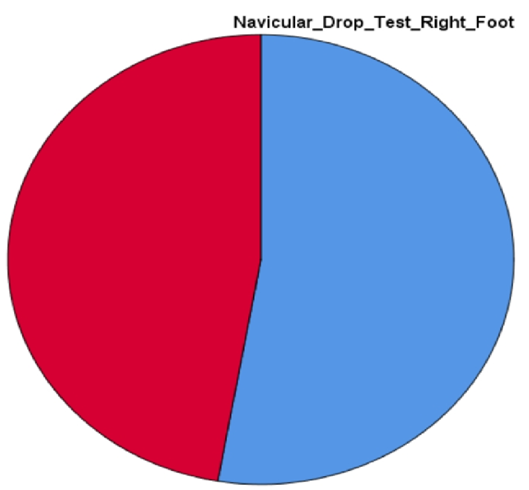
Figure 1. Pie Chart of Right Foot Navicular Drop Test
Detailed Table-2 of the left foot navicular drop test shows 36.4%, which were tested negative and 63.6%, which were tested positive.
|
Frequency |
Percentage |
|
|
Negative |
20 |
36.4 |
|
Positive |
35 |
63.6 |
|
Total |
55 |
100 |
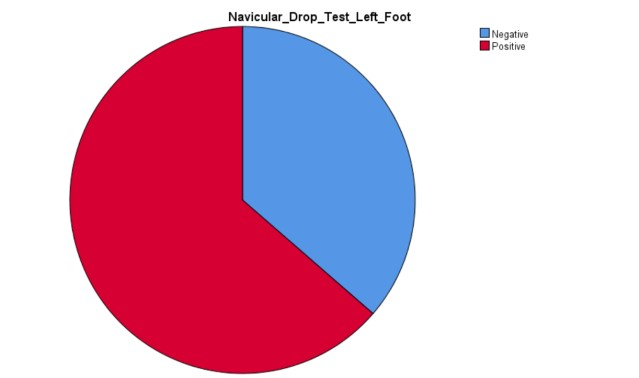
Table 2. Navicular Drop Test of Left Foot
The minimum age noticed among all the pregnant women was 20 years and the maximum age was 30 years with a mean age of 25.51 and a standard deviation of 2.96 as shown in Figure-3.
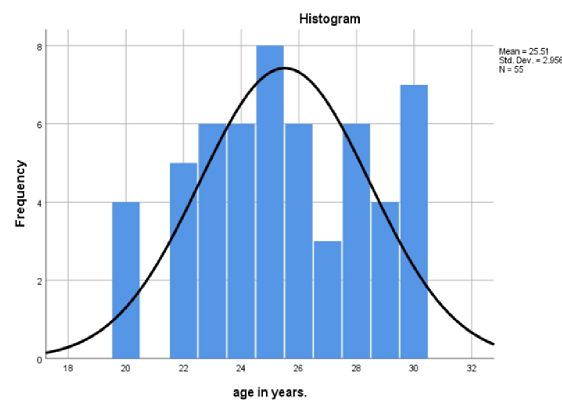
Figure 3. Histogram of Age
Out of 55 pregnant female minimum were 34 gestational weeks, maximum in 38 weeks. Notably, the mean of gestational weeks was 36.29 and the standard deviation was 1.436 as shown in Table-3 below.
Table 3. Descriptive Statistics of Gestational Age
|
N |
Min |
Max |
Mean |
Std. Deviation |
|
|
Gestational weeks |
55 |
34 |
38 |
36.29 |
1.436 |
In the given flow chart of result analysis, a sample size of 55 women was taken, while in the next step positive and negative NDT is sum of both feet of each individual which is 61 and 49 respectively.
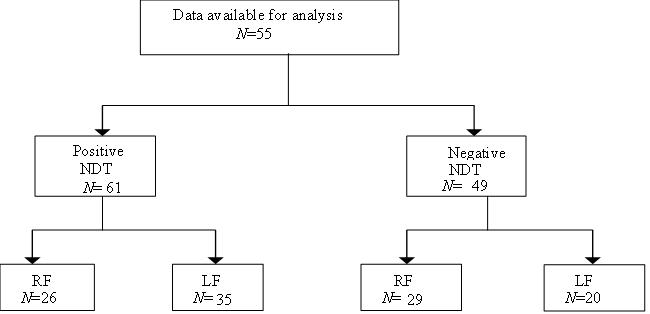
Figure 4. Conceptual Diagram of Result
A study was conducted by Pal et al. [3] to compare the dimensional changes of feet during late gestation between nulliparous, primiparous, and multiparous women. In a likewise manner, this study aimed to identify any physiological changes that occur in pregnancy as pregnancy is a time when many physical and hormonal changes occur, such as an increase in BMI due to increased pressure on the foot which can in return cause the production of relaxin resulting in joint laxity of the foot. These changes will cause a change in the height of the arches of the foot. The study also concluded that there are dimensional changes in the foot that occur during pregnancy more in multiparous women [4]. Additionally, this study also evaluated medial longitudinal arch drop in multiparous women as a prevailing symptom in their third and last trimester of pregnancy.
Structural changes in feet and arch dimensions in the third-trimester of pregnancy were studied by Barczyk-Pawelec et al. [4]. This study concluded that significant changes were observed in planter and arch structures in the final trimester of pregnancy primarily, with the transverse expansion of the left foot than the right. The results of the study also showed anthropometric changes in the last trimester of pregnancy. In the current study, significant number of changes were observed in the left foot medial longitudinal arch than in the right foot, in the last trimester.
In 2016 a study was published in "Cardiovascular Journal of Africa" done by Soma-Pillay et al, have purpose to observe physiological changes in foot during pregnancy and puerperium. In this observational longitudinal study 23 pregnant women were analyzed by using pedograph and BMI at three points during and after pregnancy in weeks 9-13,32-35 of gestation and 4-6 weeks after delivery. Foot length increases in the third trimester and returns to normal in the puerperium. During pregnancy arch of foot flattens and this persist in puerperium [13].
During pregnancy, the center of pressure on the feet shifts posteriorly to compensate for the increased anterior abdominal mass. It may contribute to loss of arch height may predispose to painful musculoskeletal conditions. This study aims to improve arch of the foot in pregnant women primipara's by giving barefoot exercises and maintains the strength of the foot. This single group pre- and post-quasi-experimental study design included 40 samples according to who fulfilled inclusion criteria. Outcomes measured through using navicular drop test, after completing the pre-test measures the subjects were introduced to the interventional procedures and followed regularly, based on the protocol. After 4 weeks of intervention, post-test measures were calculated [14].
The women subjectively complained that their shoes were too tight, resulting in foot discomfort. From the twentieth to the thirty-eighth week of pregnancy, the average increase in foot length, width, and back foot surface was 0.86cm (3.6%), 0.25cm (2.6%), and 18.36cm2(11.9%), respectively. The height of the arch decreased by an average of 0.52cm (&minus24.2%). Body mass accounted for more than 90% of the variation (R2) in foot dimensions during pregnancy and, thus indicated satisfactorypredictive ability [15].
In the current study, the medial longitudinal arch of the foot in the third-trimester among multiparous women was evaluated. Based on the analysis it was hypothesized that this study will be helpful in the future for the prevention of changes in the medial longitudinal arch by taking into account the ergonomic measures in shoes, and by doing therapeutic exercises and orthotic braces for the feet.
4.1. Key Practice Point
4.2. Conclusion
The current study concluded that there was a drop in the medial longitudinal arch of the foot. Indicatively, left foot medial longitudinal arch was shown to be less in height than the right foot medial longitudinal arch as tested by the navicular foot drop test.
4.3. Limitations of the Study
The study was only confined to third-trimester pregnant women residing in Lahore, Pakistan. Apart from that their feet pain was not assessed in the analysis.