Rizwan Asif1*, Hammad Ahmad2, Riffat Yasmin3, Farheen Ansari4, Madiha Mustafa1, Minhas Alam5, and Subtain Shah1
1Department of Eastern Medicine, Qarshi University Lahore, Lahore, Pakistan
2Department of Eastern Medicine, Government College University Faisalabad, Pakistan
3Riphah College of Rehabilitation and Allied Health Sciences, Riphah International University, Faisalabad, Pakistan
4Institute of Molecular Biology and Biotechnology, The University of Lahore, Pakistan
5Department of Virology, Provincial Headquarter Hospital, Gilgit Baltistan, Pakistan
*Corresponding Author: [email protected]
The worldwide growing antibiotic resistance against microbes has shifted the trend towards medicinal plants. Herbs are gaining courtesy for their effectiveness, safety, cheapness, and therapeutic potential. The current study focuses on the antibacterial potential of Mentha piperita (mint), Syzygium cumini (jamun), Citrus limon (lemon), and Punica granatum (pomegranate) extracts against isolated bacterial strains from diabetic foot infections. Diabetic foot samples (n=80) were collected for isolation of bacteria. Samples were run on respective media for isolation of different bacteria, which were further identified through microscopy and biochemical testing. Antibacterial activity was determined by disc and well diffusion methods. Several bacteria like S. aureus (42), P. aeruginosa (41), E. coli (28) K. pneumonia (22), S. epidermidis (15), Bacillus (7), and Proteous mirabilis (7) were isolated. Antibacterial analysis revealed moderate sensitivity of the four selected extracts against isolates, which was higher compared to most synthetic antibiotics.> The lemon extract showed moderate antibacterial activity against S. epidermidis (8mm), P. aeruginosa (10mm) Bacillus (10mm), and P. mirabilis (11mm). Similarly, pomegranate also showed moderate sensitivity against all isolated bacteria. Jamun leaf extract showed antibacterial activity against S. epidermidis (12mm), K. pneumonia (10mm), E. coli (12mm), S. aureus, (11mm) and P. mirabilis (10mm). Hence plants could be used as an alternative to synthetic antibiotics with modifications to achieve better results.
Keywords: antibiotics, antibiotic resistance, diabetes mellitus, diabetic foot, plant extracts.
The prevalence of diabetes mellitus and the complications associated with it continue to rise worldwide. Diabetic patients suffer from various types of complications which result in micro- and macro-vascular anomalies [1]. A cluster of complications like retinopathy, neuropathy, nephropathy, and diabetic foot ulcers was observed in uncontrolled diabetic patients. Diabetic foot ulcer (DFU) is one of the most lethal complications and common causes of hospitalization in diabetic patients which leads to social, psychological, and economic burdens on patients. The death rate is nearly 2.5 times higher in diabetic foot patients compared to those without foot ulcers [2]. Currently, about half of DFUs are clinically infected. Diabetic foot infections are majorly caused by the excessive use of broad-spectrum antibiotics which lead to antibacterial resistance [3].
Various microorganisms worsen wounds and delay the healing of diabetic foot patients with S. aureus, Streptococci, and P. aeruginosa being common causes of skin infections [4]. In Pakistan, the incidence of diabetes is 11.1%, and impaired fasting glucose levels are more common in men (4.2%) than in women (2.3%). Recently, the incidence of diabetes mellitus in Pakistan has increased gradually. In Pakistan, WHO estimates over five million new cases by 2025 [5]. In the case of diabetic foot, patients become vulnerable to microorganisms such as E. coli, K. pneumonia, S. aureus, and P. aeruginosa due to skin breaches. Due to excessive misuse of chemotherapeutic drugs, antibiotics have become resistant against bacteria, known as multi-drug resistant organisms [6].
Different treatment plans are available for diabetic foot ulcers and the most commonly used method is broad-spectrum synthetic antibiotics. However, excessive use of these antibiotics leads to resistance against microbes. There is an urgent need to establish new ways for treatment to reduce the side effects of these synthetic antibiotics, indirectly to reduce the economic burden. Recently medicinal plants and their products have been getting attention for their usage as antimicrobial agents [7].
Medicinal plants are widely used as antimicrobial agents. Recently, the importance of medicinal plants has increased to treat chronic skin wounds. Different plants have diverse medicinal roles
like anti-inflammatory and antimicrobial properties. Due triggering of growth factors like cytokines and chemokines plays an important role regeneration of the skin and wound healing without any adverse effects. Previously, various studies reported the role of medicinal plants, for instance, Aloe vera, Mimosa vulgaris, Angelica sinensis, and Lavanduela stoechas. These medicinal plants were used in different formulations such as ointments, creams, and gels to treat chronic skin wounds [8].
Diabetic wound healing impairment is a serious health challenge globally for health professionals. To deal with this health challenge, different strategies are developing and medicinal plants are deeply getting attention. Infect medicinal plants possess chains of secondary metabolites or ingredients that have fewer side effects as compared with orthodox therapeutic agents. Therefore, interest in medicinal plants is growing in the wound healing process both in diabetic and non-diabetic conditions [9]. Therefore, the purpose of this study was to evaluate the microbiology profile and susceptibility pattern of selected herbal extracts and their comparison with commercial antibiotics against clinical bacterial isolates.
2.1. Population Size
The population size was n = 80 between 31-85 years of age and having a history of type 2 diabetes mellitus. These patients were admitted to the surgery department of different public and private hospitals in Lahore with a history of Diabetic Foot Infections (DFIs). The following data like age, gender, diabetes duration, DFU duration, history of hospital admissions for the same ulcer, and previous use of antibiotics in the preceding 6-12 months were noted.
2.2. Sample Collection and Transportation
Before taking the samples, the wound was cleaned with normal saline. The sterile cotton swab was used for direct swabbing from the center of the diabetic wound (leg, feet, and amputation of leg). The samples were immediately transported to the Microbiology laboratory of the IMBB department at the University of Lahore, Pakistan according to the procedure adopted by [10].
2.3. Sample Processing, Isolation, and Bacterial Identification
The sample was streaked with cotton swab sticks on Mannitol Salt Agar (MSA), MacConkey agar, Cetrimide, and Blood agar medium. All plates were incubated aerobically at 37ºC for 24 hours and examined for bacterial growth. Different microbial techniques like macro-morphology, microscopy, and biochemical testing were carried out for the identification and confirmation of isolated bacteria [11].
nd Extraction tion and Idene alike gentsrse the wound of diabetic foot patient.
2.4. Plants Collection and Extraction
Fresh leaves of four plants (mint, jamun, lemon, and pomegranate) were collected from Pattoki Nursery Punjab, Pakistan. Leaves were washed thoroughly with running tap water and air dried at room temperature for 3-4 days. The dried leaves were crushed into fine powder in an electric grinder and stored in bottles at room temperature. For extract preparation, 10 g of each plant powdered was dissolved in 100 ml of ethanol separately in a conical flask. The flasks were placed in a shaker incubator at 37 ºC. Liquid extracts were separated from solids by using Whatman filter paper and a rotary evaporator was used to concentrate them [12].
2.5. Antibacterial Sensitivity
Extracts of plants were evaluated for in-vitro antimicrobial activity. The isolated microorganisms were inoculated on Muller Hinton agar plates by the spread plate method and extract-impregnated discs were placed on the agar surface and pressed a little. The plates were kept in an incubator for 24 hours at 37 ºC and examined for ZOI. Gentamycin and DMSO were used as positive and negative controls, respectively. Similarly, the susceptibility of different antibiotics like Penicillin (10 µg), Ampicillin (10 µg), Aminoglycosides (30 µg); Gentamycin (30 µg), Ciprofloxacin (10 µg), Chloramphenicol (30 µg) Azithromycin (15 µg) and Erythromycin (30 µg) was also evaluated against these isolated microbes. Based on ZOI, the bacteria were considered sensitive or resistant. The intermediate zone is considered sensitive for the interpretation of results [13].
All the study data was analyzed by applying the statistical tool of Microsoft Excel 2013 and were tabulated or presented graphically. Microsoft Excel was used for data entry and data analysis. Data was represented as frequencies, percentages, tables, and charts.
3.1. Selection of Diabetic Patients
Diabetic foot ulcer patients were selected from different hospitals in Lahore, Punjab Pakistan for isolation of bacteria. Patients were evaluated by taking the history of illness to consider them for the study.
3.2. Sample Processing
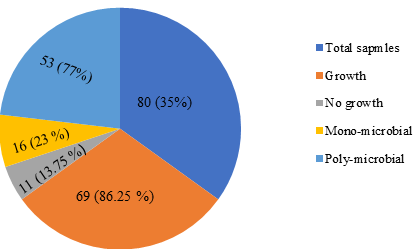
A total of 80 samples were collected and transported to the microbiology laboratory of the University of Lahore, Pakistan. The samples were inoculated on nutrient agar plates and incubated at 37 ͦ ͦC and the bacterial colonies were observed after 24 hrs of incubation. A total of 80 samples with equal in number both male and female were collected; 7 samples did not show any growth while 73 samples showed the growth of either mono-microbial or poly-microbial as shown in Fig 1.
Figure 1. Growth of Samples from Diabetic Foot Ulcer
3.3. Identification of Bacterial Isolates
The bacterial isolates were confirmed based on colony morphology, gram staining, and biochemical testing. They were sub-cultured on specific media like blood, MacConkey, and mannitol salt agar. Yellow growth was observed for S. aureus and S. epidermidis showed pink on mannitol salt agar as shown in Figure 2. Biochemical tests were performed for further identification of bacteria. A Catalase positive test was performed for the identification of S. aureus as shown in Figure 3.
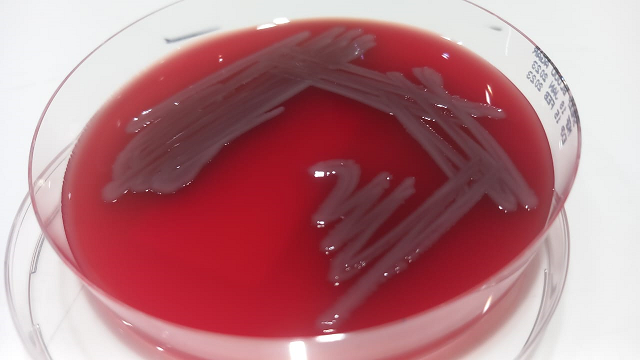
Figure 2. (A) Growth of S. aureus & S. epidermidis on MSA (B) Growth of K. pneumoniae on Blood Agar

Figure 3. Catalase Positive Test of S. aureus
3.4. Prevalence of Isolated Bacterial Strains
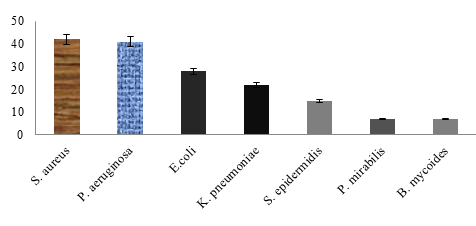
Both gram-positive (28%) and gram-negative (72%) bacteria were isolated from diabetic samples with the prevalence of S. aureus (42), P. aeruginosa (41), E. coli (28) K. pneumonia (22), S. epidermidis (15), Bacillus (7), and Proteous mirabilis (7), respectively as shown in Figure 4.
Figure 4.Bacterial Species Isolated from Diabetic Patients
3.5. Evaluation of Sensitivity against Antimicrobial Agents
After their identification, the antibacterial sensitivity of herbal extracts and synthetic antibiotics was carried out in Table 1 showing the zone of inhibition (mm) of each antimicrobial agent against each isolated bacterial strain from diabetic foot infection and herbal extract, which showed a moderate zone of inhibition against maximum bacterial strain.
Table 1. Zones of Inhibition (mm) by Each Antimicrobial Agent against Isolates

Diabetes mellitus is a global health issue characterized by a raised level of glucose in the blood linked with wide etiology. Long-term raised glucose levels induce multiple complications, including retinopathy, nephropathy, and diabetic foot [14]. The objective of this study is to find the bacteriology load in diabetic ulcers and compare the antibacterial sensitivity effect between commonly used synthetic antibiotics and selected herbal plants. In this study, the prevalence of diabetic foot was found more common in males with a mean age of 71 years, denoting the existence of this condition in the elderly population. Also, both mono-microbial and polymicrobial were associated with diabetic foot. However, the majority of samples were linked with polymicrobial. Similar findings were also observed in developing countries like India and Pakistan [15].
A recent study showed that diabetic foot ulcer prevalence was higher in men approximately 68% as compared to women nearly 32%. Notably, different factors are involved, such as genetic dominance and more time exposure to their foot during outdoor activity. Interestingly, the present study also noted a predominance of polymicrobial infections and this could be related to the severity of the infection like chronic wounds and more complex infections [16]. Several bacteria like S. aureus, P. aeruginosa, E. coli, K. pneumoniae, S. epidermidis, Bacillus, and P. mirabilis were isolated. S. aureus was the most frequent micro-organism linked with P. mirabilis isolation. K. pneumonia and E. coli are the most dominant gram-negative bacteria that exhibit a high resistance profile against common antibiotics. S. aureus had the highest percentage followed by P. aeruginosa and E. coli, respectively. This study completely agrees with the results of the previous study [17, 18]. In conclusion, S. aureus, S. epidermidis gram-positive P. aeruginosa, and E. coli Gram-negative are the major reasons for causing diabetic foot, which may lead to antibiotic resistance rate and 65% of the resultant surgical intervention. The commonly isolated bacteria in this study were S. aureus, P. aerugimosa, E. coli, K.pneumoniae, S.epidermidis, P. mirabilis, and B. mycoids which were also observed in a previous study [19].
Unlike previous studies in which most numbers of samples were polymicrobial. The majority of the samples in this study yield one type of microbe [20]. In comparison most prevalent bacterial isolates were in this case S. aureus followed by Pseudomonas sp. Klebsiella sp, E. coli, and Proteus sp. that was the strongest point of this study [21].
Wounds of diabetic patient's feet were commonly infected by Staphylococcus aureus, Enterococci sp. Pseudomonas aeruginosa, Escherichia coli, Klebsiella sp. and Proteus sp. The same kinds of bacterial isolates were isolated from the samples in this study.
The second objective of this study after their isolation was testing of antibiotic resistance and sensitivity against patent antibiotics and herbal extracts. Present study results show considerable resemblance with the past studies by [22]. The present study showed the prevalence of bacteria involved in diabetic foot ulcers. According to this study S. aureus had the highest prevalence followed by P. aeruginosa. E. coli, K. pneumonia, S.epidermidis, P. vulgaris and B. mycoides. In a previous study S. aureus and P. aerugenosa were found predominant in diabetic foot ulcers [23]. The mint and (black plum) jamun extracts showed a zone of inhibition against Bacillus Sp. was comparable to penicillin and ampicillin antibiotics. While jamun and lemon extracts showed a considerable zone of inhibition against P. mirabilis to which most of the patent antibiotics were resistant. The antibacterial activity of mint was screened against multi-drug resistant bacteria, indicating their effectiveness in both nosocomial and community-acquired infections [24]. In the same way, this study also showed that mint extract can be used to treat multi-resistant cases of diabetic foot infection. Pomegranate and lemon extracts were also sensitive against P. aeruginosa as compared to the results showed by azithromycin, while other standard antibiotics were resistant against all except chloramphenicol.
Citrus fruit peel extract showed considerable results when tested against microbes isolated from diabetic foot infections [25]. The herbal extracts did not show remarkable sensitivity against isolated bacteria as shown by some standard antibiotics. This may be enhanced by dose adjustment and standardizing the herbal extract. So, antimicrobial medicinal plants with minimum cost and side effects may be a suitable alternative to synthetic antibiotics.
4.1. Conclusion
The study's results highlighted the antibacterial activity of different herbal extracts, namely, mint, jamun, lemon, and pomegranate against different bacteria isolated from patients with a diabetic foot infection. Jamun leaves extracted from plants showed a zone of inhibition against S. epidermidis (12mm), K. pneumonia (10mm), E. coli (12mm), S. aureus, Bacillus (11mm), and P. mirabili (10mm). Similarly, the mint extract showed reasonable zoi against S. aureus (10mm), E. coli (11mm), and Bacillus (8mm). The results of this study proved that herbal extracts could be a good antibacterial agent with some changes and a better choice being cheap and safe as compared to chemotherapeutic agents. Lastly, these extracts may be used in the future to formulate antibacterial products for tropical use or can be used in combination with synergistic effects.
1. Shaheen MM, Al Dahab S, Abu Fada M, Idieis R. Isolation and characterization of bacteria from diabetic foot ulcer: amputation, antibiotic resistance and mortality rate. Int J Diabet Develop Count. 2021;42:1–9. https://doi.org/10.1007/s13410-021-00997-7
2. Boulton AJ, Armstrong DG, Kirsner RS, et al. Diagnosis and management of diabetic foot complications. ADA Clinic Compend. 2018;2018(2):1–20. https://doi.org/10.2337/db20182-1
3. Care D. Economic costs of diabetes in the US in 2017. Diabetes Care. 2018;41(5):917–928. https://doi.org/10.2337/dci18-0007
4. Mureithi M, Ngugi N, Otieno F. Diabetic foot ulcers in a kenyan referral and teaching hospital: risk factors, patient characteristics and clinical outcomes. Series Endocrinol Diabet Metabol. 2019;1(2):41–51.
5. Bahadar H, Mostafalou S, Abdollahi M. Growing burden of diabetes in Pakistan and the possible role of arsenic and pesticides. J Diabet Metabol Disord. 2014;13:1–8. https://doi.org/10.1186/s40200-014-0117-y
6. Yan X, Song J-f, Zhang L, Li X. Analysis of risk factors for multidrug-resistant organisms in diabetic foot infection. BMC Endocr Disord. 2022;22:e46. https://doi.org/10.1186/s12902-022-00957-0
7. Permana R, Tosida ET, Suriansyah MI. Development of augmented reality portal for medicininal plants introduction. Int J Global Oper Res. 2022;3(2):52–63.
8. Ramírez-Gómez XS, Jiménez-García SN, Campos VB, Campos MLG. Plant metabolites in plant defense against pathogens. In: Topolovec-Pintaric S, ed. Plant Diseases-Current Threats and Management Trends. BoD - Books on Demand; 2019:49–68.
9. Oguntibeju OO. Type 2 diabetes mellitus, oxidative stress and inflammation: examining the links. Int J Phys Pathophysiol Pharmacol. 2019;11(3):45–63.
10. Karmaker M, Sanyal SK, Sultana M, Hossain M. Association of bacteria in diabetic and non-diabetic foot infection–An investigation in patients from Bangladesh. J Infect Public Health. 2016;9(3):267–277. https://doi.org/10.1016/j.jiph.2015.10.011
11. Aorkwagh M, Wanen I, Alye C, Gberindyer A, Asue U. Isolation and identification of bacteria prevalent among Nigerian currency notes in selected areas in and around Akperan Orshi College Of Agriculture, Yandev. J Sci Indust Stud. 2015;13(3):74–81.
12. Gonelimali FD, Lin J, Miao W, et al. Antimicrobial properties and mechanism of action of some plant extracts against food pathogens and spoilage microorganisms. Front Microbiol. 2018;9:e1639. https://doi.org/10.3389/fmicb.2018.01639
13. Manikandan C, Amsath A. Antibiotic susceptibility of bacterial strains isolated from patients with respiratory tract infections. Int J Pure Appl Zool. 2013;1(1):61–69.
14. Fralick M, Jenkins AJ, Khunti K, Mbanya JC, Mohan V, Schmidt MI. Global accessibility of therapeutics for diabetes mellitus. Nat Rev Endocrinol. 2022;18(4):199–204. https://doi.org/10.1038/s41574-021-00621-y
15. Sekhar SM, Vyas N, Unnikrishnan M, Rodrigues G, Mukhopadhyay C. Antimicrobial susceptibility pattern in diabetic foot ulcer: a pilot study. Ann Med Health Sci Res. 2014;4(5):742–745.
16. Karmakar M, Katsnelson MA, Dubyak GR, Pearlman E. Neutrophil P2X7 receptors mediate NLRP3 inflammasome-dependent IL-1β secretion in response to ATP. Nature Commun. 2016;7(1):e10555. https://doi.org/10.1038/ncomms10555
17. Appapalam ST, Muniyan A, Mohan KV, Panchamoorthy R. A study on isolation, characterization, and exploration of multiantibiotic-resistant bacteria in the wound site of diabetic foot ulcer patients. Int J Lower Extrem Wounds. 2021;20(1):6–14. https://doi.org/10.1177/15347346198844
18. Naeem F, Anjum FR, Arshad MA, et al. Isolation and antibiotic sensitivity pattern of drug resistant bacteria in ulcerative foot of type 2 diabetic patients. Pak J Pharm Sci. 2019;32(4):1843–1848.
19. Saeed S, Tariq P. Antimicrobial activities of Emblica officinalis and Coriandrum sativum against gram positive bacteria and Candida albicans. Pak J Bot. 2007;39(3):913–917.
20. Verma P. A study on isolation of different type of bacteria from pus. Int J Pharm Life Sci. 2012;3(11):2107–2110.
21. Rajalakshmi V, Amsaveni V. Antibiotic susceptibility of bacterial pathogens isolated from diabetic patients. Int J Microbiol Res. 2012;3(1):30–32.
22. Khadir MK, Hasan AY, Salman RM. Inhibitory effect of myrtus communis L. and syzygium aromaticum L. Extracts on the growth of staphylococcus aureus isolated from foot ulcers of diabetic patients. Diyal J Pure Sci. 2018;14(3):108–121.
23. Hena J, Growther L. Studies on bacterial infections of diabetic foot ulcer. Afr J Clinic Exper Microbiol. 2010;11(3):146–149. https://doi.org/10.4314/ajcem.v11i3.57768
24. Al-Sum BA, Al-Arfaj AA. Antimicrobial activity of the aqueous extract of mint plant. Sci J Clin Med. 2013;2(3):110–113. https://doi.org/10.11648/j.sjcm.20130203.19
25. Gopal PV. Evaluation of anti-microbial activity of citrus aurantium against some gram positive and negative bacterial strains. Pharmacia. 2012;1(3):107–109.