Effect of Clomiphene Citrate on Fertility Hormones in Women with Polycystic Ovarian Syndrome
Asma Arshad1, Kashif-Ur-Rehman1, Hamama Islam Butt2, Shahzad Bashir1, Fatima Umar1, Zahida Yaseen3, Kashish Zahra4, Ahmad Bakhsh1*
1School of Biochemistry, Minhaj University, Lahore, Pakistan
2School of Medical Lab Technology, Minhaj University, Lahore, Pakistan
3Center for Research and Development (CRD), Minhaj University, Lahore, Pakistan
4Department of Chemistry, Superior University, Lahore, Pakistan
Abstract
This study aims to investigate the positive effect of Clomiphene Citrate (CC) in inducing ovulation in women with PCOS. Clomiphene Citrate is a non-steroidal drug that primarily affects estrogen production. CC also has pronounced effects on balancing of the female hormones, normal ovulation process, and overcoming the PCOS-based infertility issues. Hormonal profile evaluation including follicle stimulating hormone (FSH), luteinizing hormone (LH), progesterone, and estrogen was performed at Clinical Laboratory, Services Hospital, Lahore. Serum volume of the aforementioned hormones were determined in PCOS-suffering infertile women (n=50) and healthy fertile women (n=50) by using a commercially available ELISA kit manufactured by Calbotech lnc. Serum luteinizing hormone (LH), follicle stimulating hormone (FSH), progesterone, and estrogen mean values in PCOS patients before the use of CC were evaluated as 5.74±0.939 (IU/L), 3.804±1.163 (IU/L), 2.098±1.233 (ng/ml), and (51.458±7.091 pg/ml respectively, while after management with CC the mean value of serum LH, FSH, Progesterone, and Estrogen were 3.716±0.513 (IU/L), 5.644±1.130 (IU/L), 10.704±2.313 ng/ml and 37.72±4.969 pg/ml respectively, which indicated a significant differences in hormonal pattern. The current study demonstrates that Clomiphene Citrate (CC) has positive effects in ovulation process in females with polycystic ovarian syndrome (PCOS), within the local population.
1. Introduction
The Polycystic ovarian syndrome (PCOS) is an important endocrinal disarray found in females during their reproductive period, with a prevalence rate of 20 percent [1]. The main cause of PCOS is hormonal imbalance, which includes hyperandrogenemia (HA), high release of luteinizing hormone, estrogen and follicle stimulating hormone (FSH). It is also a source of multiple pathological abnormalities including anovulation, polycystic ovaries, menstrual disorders, infertility as well as increased insulin resistance, diabetes type 2 and obesity [2]. A recent study suggests that PCOS can be developed due to malfunction in human gut microbiota (GM), which can be manifested in chronic inflammation and diabetes [3]. Moreover, molecular investigations revealed a low level of miRNA-592 and hypomethylation of LHCGR regions that could interrupt LH hormone release and ovarian follicle development which leads to PCOS [4].
Major focus in PCOS treatment includes changes in hormonal regulation (including LH, FSH, estrogen and progesterone) and infertility due to anovulation. The release of luteinizing hormone (LH) from anterior pituitary gland, accentuates the production of ovum and formation of ovarian steroid especially estrogen, progesterone and FSH. Moreover, in females FSH produced via anterior pituitary gland, in turn stimulates the follicular growth inside the ovaries that formulates ovarian follicles under the action of luteinizing hormone (LH), moreover it results in LH induced estrogen secretion.
Progesterone is mainly synthesized from circulating cholesterol and by nature is a C21 steroid. Cholesterol conversion to progesterone is attained via a combined mechanism of dehydrogenase and isomerase enzymes. The primary role of progesterone is exhibited mainly by the reproductive organs, whereas in males it is a crucial intermediate for the production of corticosteroids and androgens. While, in women it stay relatively persistent throughout the follicular period of the menstrual cycle. The plasma levels of progesterone stay elevated for 4-6 days, with a decline to initial levels within 24 hours before the onset of menstruation. Estradiol E2 is a potent naturally produced Estrogen by the placenta and ovary, additionally a smaller amount is secreted by the adrenal cortex. Estradiol secrete into blood stream via binding to sex hormone binding globulin (SHBG). Whereas, Estradiol receptor complex greatly affects estrogenic activity, that further triggers a appropriate response. Clomiphene Citrate (CC) therapy is a straightforward, affordable and successful technique for induction of ovulation with fewer side effects and it has been frequently used as a first line management for anovulatory PCOS [5, 6]. Women with polycystic ovarian syndrome have a metabolic syndrome prevalence of 33% [7]. Weight loss helps to recover not only metabolic syndrome but also increase PCOS resolution up to 3 to 8 fold [8]. Poverty is one of the major social issues that greatly impacts the healthy women and leads to polycystic ovarian syndrome condition.
Infertility due to ovulation failure, accounts for about 30% of all infertility cases that were research in current study [9]. CC enhances the follicular growth by inhibiting estrogen's negative feedback mechanism loop and furthermore stimulates the secretion pituitary gonadotropins. As a result, CC has been recommended as a traditional first line medicine to promote fertility in females with polycystic ovarian syndrome (PCOS) , however its anti-estrogenic effect on cervical mucus and endometrial layers, while receptivity resulted in a low pregnancy rates [10]. The metabolic health issues like insulin resistance, compensatory hyperinsulinemia, Type II diabetes and dyslipidemia are all significantly linked to PCOS [11]. Medicinal treatments for anovulation usually includes CC, Letrozole or Metformin treatment [12]. CC is now used as a standard medication for inducing ovulation in polycystic ovarian syndrome (PCOS) patients globally. Insulin resistance (IR) is a foremost metabolic anomaly of PCOS that leads to the hyperinsulinemia and hyperandrogenism [13]. Moreover, treating insulin resistance by using combined drug therapy (like CC and metformin) may trigger normal ovulation especially in obese female with pronounced insulin resistance (IR) [14]. For management of anovulation in women with polycystic ovarian syndrome, the treatment options are offered with special focus. However, there are other co-morbid conditions which exist with PCOS like cardio metabolic syndrome, enhance body mass index (BMI), mental disorders and reduced quality of life [15]. The current study investigated the effect of CC in controlling four hormonal levels (Estrogen, LH, FSH and progesterone) in women with PCOS.
2. MATERIALS AND METHODS
This study was designed and approved by the Ethical Committee of School of Biochemistry, Minhaj University of Lahore, with IRB number MUL/BIOCHEM/87/2018. This clinical trial study was carried out at the Infertility Filter Clinic and Clinical Pathology Laboratory, Services Hospital Lahore. This study included a total 100 female subjects, out of which 50 women were infertile with polycystic ovarian syndrome (PCOS) and 50 were vigorous fertile women that were taken as healthy control group. The study was carried out from November 2018 to January 2019. Inclusion criteria for the study were married, infertile, obese and non-obese females with age range between 20-45 years. Exclusion criteria include diabetes type 2, hypertension and unmarried females. Each individual from experimental group received 50 mg of CC dose. The treatment regimen started with one tablet daily as a starting dose at 3rd day of menstrual series for five days in the 1st month, followed by twice daily in the same pattern in the second month that was finally increased to three times daily following the third month. The levels of serum FSH, LH, estrogen and progesteron were measured by ELISA kit manufactured by (Calbotech lnc, USA). The blood samples (n=100) were collected by the Gynecology and Obstetrics Department of Services Hospital, Lahore. The venous blood samples were collected via disposable syringes (5 ml, BD syringes) and transferred into gel vials that were kept in incubator at 37 ℃ for 30 minutes. The serum were extracted after centrifugation at 3000 rpm for 4 minutes, which were then transferred into labeled serum cups and stored at -20 ℃ for further analysis. Hormonal analysis of each serum samples were performed, that was based on a non-competitive sandwich principle of ELISA.
2.1 Assay for Determination of Luteinizing Hormone
The 96 wells micro-titer wells were coated with streptavidin. The samples and conjugated anti-LH/anti-biotin were added to well, LH in serum was sandwiched between antibodies which was labeled with HRP. Thymol Blue (TMB) was added into the reaction mixture, which was further incubated for 15 minutes at alkaline pH. The appearance of blue color was proportional to the LH concentration and was measured by taking absorbance at 450 nm spectrophotometrically [16].
2.2 Assay for Determination of Follicle Stimulating Hormone
For FSH analysis serum specimen and a diluted conjugate of anti-FSH-HRP were added to 96 micro-well plates coated with FSH beta subunit Monoclonal antibody (Mab). The FSH present in the sample bound with anti-FSH Mab, coated in the well and a secondary antibody anti-FSH-HRP, then attaches with FSH. The HRP conjugate and unbound protein fractions were then subsequently washed by wash buffer. After TMB addition, there was change in yellow to blue color, which was measured after 15 minutes with the addition of stop solution by using spectrophotometer at 450 nm [17].
2.3 Assay for Determination of Estrogen
The assay mixture consisted of serum and estrogen (E2) peroxidase conjugate to 96 wells ELISA plate, coated with anti-E2 antibodies. Serum estrogen reacted with anti-E2 antibodies on the micro-well plate. The unbounded E2- peroxidase was washed off by wash buffer. After addition of TMB, reaction mixture was incubated for 15 minutes, followed by addition of stop solution and change in color (from yellow to blue) was measured at 450 nm [18].
2.4 Assay for Determination of Progesterone
The Progesterone-enzyme conjugate plus patient serum were added to wells, coated with anti-progesterone Ab. The progesterone in patient’s serum gets bound to anti-progesterone Ab present in the wells. The unbounded progesterone enzyme was washed from wells via wash buffer. After addition of TMB, color changed from yellow to blue at alkaline pH and intensity of color was evaluated at 450 nm, 15 minutes after the addition of stop solution [19].
2.5 Statistical Analysis
The statistical investigation tool SPSS (version 17.0) was used for the data analysis. One-tailed-t-test was used to check the effect of CC on hormonal level in both groups studied data. p value (p≤0.05) was taken as statistically, significant. The analyzed data was represented as mean values with standard deviations.
3. RESULTS
All 100 participants (control and experimental), included in this study completed the CC therapy for the recommended time period of 3 months. All the subjects in control group and experimental groups were initially analyzed for serum hormones level (shown in Table 1).
Table 1. Comparison of the Levels of Luteinizing Hormone, Follicle Stimulating Hormone, Progesteron, Estrogen and BMI between Control and Polycystic Ovarian Syndrome Groups Before Treatment with CC
|
Hormone |
Control (Mean ± SD) |
PCOS (Mean ± SD) |
p-value |
|
LH (lU/L) |
4.672 ± 1.006 |
5.748 ± 0.939 |
<0.001 |
|
FSH (IU/L) |
6.4 ± 0.961 |
3.804 ± 1.163 |
<0.001 |
|
Progesteron (mg/ml) |
11.13 ± 2.352 |
2.098 ± 1.233 |
<0.001 |
|
Estrogen(pg/ml) |
30.06 ± 4.41 |
51.458 ± 7.091 |
<0.001 |
|
BMI (kg/m2) |
21.772 ± 2.960 |
23.842 ± 0.665 |
<0.001 |
*The statistically significant level was (p < 0.05).
**LH = Luteinizing Hormone
***FSH = Follicle Stimulating Hormone
Table 1 shows that levels of LH, estrogen and BMI were increased in women with polycystic ovarian syndrome, while, its assessment remained normal in the healthy females. Levels of serum FSH and progesteron hormone were decreased in PCOS women in comparison to normal controls. It showed that the prominent or decreased altitude of hormone in polycystic ovarian syndrome is due to up regulated pattern of hormones.
To measure the effect of clomiphene citrate among PCOS patients, the hormonal levels along with BMI in experimental subjects were measured, before and after drug administration. The subjects were divided into 2 groups for the analysis. The results are presented in Table II. The statistical analysis revealed significant variation (p<0.05) before and after the use of clomiphene citrate on the hormonal profiles of patients. The p-value <0.05, which revealed statistically significant difference in fertility hormones levels between the two groups.
Table 2. Comparison of Luteinizing Hormone, Follicle Stimulating Hormone, Progesterone and Estrogen in Patients Before and After Treatment with Clomiphene Citrate
|
Hormones |
Infertile Women with PCOS before CC (Mean ± SD) |
Infertile Women with PCOS after CC (Mean ± SD) |
p value |
|
LH (IU/L) |
5.74 ± 0.939 |
3.716 ± 0.513 |
<0.001 |
|
FSH (IU/L) |
3.804 ± 1.163 |
5.644 ± 1.130 |
<0.001 |
|
Progesteron (ng/ml) |
2.098 ± 1.233 |
10.704 ± 2.31 |
<0.001 |
|
Estrogen (pg/ml) |
51.458 ± 7.091 |
37.72 ± 4.969 |
<0.001 |
*LH = Luteinizing Hormone
**FSH = Follicle Stimulating Hormone
Table 2 shows the decrease in LH and estrogen level and an increase in progesterone and FSH level after CC regimen.
Figure 1 shows that the mean levels of serum LH U/ml, FSH U/ml, progesterone ng/ml and estradiol pg/ml in infertile women with PCOS before clomiphene citrate (CC) were 5.74 U/ml, 3.804 U/ml, 2.098 ng/ml and 51.458 pg/ml respectively, while the mean levels of serum LH U/ml, FSH U/ml, progesterone ng/ml and estradiol pg/ml in infertile women with PCOS after clomiphene citrate were 3.716 U/ml, 5.644 U/ml, 10.704 ng/ml and 37.72 ng/ml respectively.
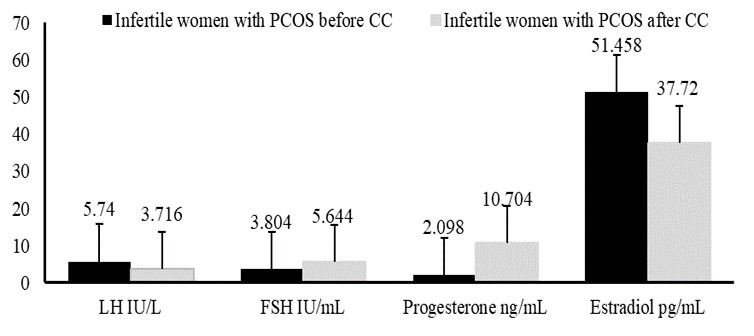
Figure 1. Comparison of serum Luteinizing Hormone, FSH, Progesterone and Estradiol in infertile women before and after management with CC
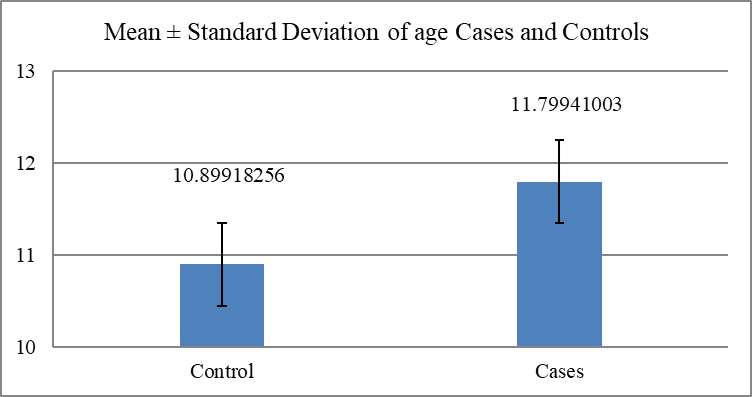
Figure 2. Age wise Mean ± Standard Deviation for both cases and controls groups
4. DISCUSSION
Clomiphene Citrate (CC) is an antiestrogenic drug that reduces the estrogen release [20]. A cohort study by Branigan [21] demonstrated that CC and oral contraceptive pills (OCP) help prevent the hyper-secretion of LH in women. Al-Inany emphasized the cause of CC in dropping luteinizing hormone (LH), levels that have best anti-estrogenic consequence. They also reported that stage of FSH and progesterone were also elevated after 21 days of CC used. Significant changes in hormonal levels have been observed in 50 women that were included in this study with PCOS health issue, as compared to normal control women.
PCOS is a heterogeneous clinical disorder with high prevalence in young female. The CC drug is a non-steroidal discerning estrogen receptor modulator, that constraints the estrogen receptors present in hypothalamus, as well as resulted in a negative feedback impact of estrogen on gonadotropins release which leads to the increased activity of the gonadal, pituitary and hypothalamic axis [22]. Furthermore, clomiphene citrate drug has a high failure probability as a first procession medication for ovulation induction. However, patients were shown to have an increased chance of developing ovarian cancer if they used CC medication for more than six menstrual cycles [23]. The major cause of PCOS is thought to be a decrease in the sympathy of preantral follicles to follicle stimulating hormone or an boost in the follicular activity due to LH, which inhibits the normal pathway of follicle development [24].
The disturbance of the hypothalamic pituitary ovarian axis is the primary cause of ovarian dysfunction in PCOS as demonstrated by increased gonadotropins releasing hormone (GnRH) pulse frequency [25]. Before starting pharmacological induction of ovulation, it is critical to first improve the individual strong by ensuring that one's (BMI) is normalised, or that those who are considerably obese have to lose at least 5–10% of their body weight. Body Mass Index should ideally be fewer than 30 kg/m2, yet it is acknowledged that for numerous women experiencing reproductive issues, age is also a key factor, thus a realistic approach is required in such a situation. Nonetheless, there is a definite link between high BMI and poor pregnancy outcomes, including miscarriage, pre-eclampsia and congenital abnormalities, as well as gestational diabetes [26]. There is probability that in 25% of couples, ovarian illness is the principal reason of infertility and PCOS is furthermost common cause of an-ovulatory infertility, which is nearly 70% of reported cases [27, 28]. Broadly, it can be concluding that obesity, dyslipidemia, IR, hyperinsulinism, type 2 DM and cardiovascular disease are among the prevalent endocrine and metabolic features which are linked to PCOS. Moreover, PCOS can elevate the risk of miscarriages and pregnancy issues including gestational diabetes in women [29, 30].
4.1 Conclusion
The present study has demonstrated that the clomiphene citrate potentially holds positive effects in inducing fertility in women with PCOS in our general population. Anovulation causes infertility due to defects in the luteal phase, but the use of clomiphene citrate in prescribed manner results in the hormonal balance, increase in fertility levels and relief from the symptoms of PCOS. This study can be helpful for the clinicians and practitioners to overcome the situation of PCOS in females that have various deleterious health impacts on the reproductive life of women.
Conflict of Interest
The author of the manuscript has no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The data associated with this study will be provided by the corresponding author upon request.
Bibliography
- Kolesnikova L, Kolesnikov S, Darenskaya M, et al. Activity of LPO processes in women with polycystic ovarian syndrome and infertility. Bull Exp Biol Med. 2017;162(3):320–322. https://doi.org/10.1007/s10517-017-3605-5
- Corte LD, Foreste V, Barra F, et al. Current and experimental drug therapy for the treatment of polycystic ovarian syndrome. Expert Opin Invest Drugs. 2020;29(8):819–830. https://doi.org/10.1080/13543784.2020.1781815
- Zhao X, Jiang Y, Xi H, Chen L, Feng X. Exploration of the relationship between gut microbiota and polycystic ovary syndrome (PCOS): a review. Geburtshilfe Frauenheilkd. 2020;80(02):161–171.
- Abbott DH, Dumesic DA, Levine JE. Hyperandrogenic origins of polycystic ovary syndrome–implications for pathophysiology and therapy. Expert Rev Endocrinol Metab. 2019;14(2):131–143. https://doi.org/10.1080/17446651.2019.1576522
- Homburg R. Clomiphene citrateend of an era? A mini-review. Hum Reprod. 2005;20(8):2043–2051. https://doi.org/10.1093/humrep/dei042
- Imani B, Eijkemans MJ, te Velde ER, Habbema JDF, Fauser BC. A nomogram to predict the probability of live birth after clomiphene citrate induction of ovulation in normogonadotropic oligoamenorrheic infertility. Fertil Steril. 2002;77(1):91–97. https://doi.org/10.1016/S0015-0282(01)02929-6
- Chandrasekaran S, Sagili H. Metabolic syndrome in women with polycystic ovary syndrome. Obstet Gynaecol. 2018;20(4):245–252. https://doi.org/10.1111/tog.12519
- Greenwood EA, Pasch LA, Shinkai K, Cedars MI, Huddleston HG. Clinical course of depression symptoms and predictors of enduring depression risk in women with polycystic ovary syndrome: results of a longitudinal study. Fertil Steril. 2019;111(1):147–156. https://doi.org/10.1016/j.fertnstert.2018.10.004
- Kini S. Polycystic ovary syndrome: diagnosis and management of related infertility. Obstet Gynaecol Reprod Med. 2012;22(12):347–353. https://doi.org/10.1016/j.ogrm.2012.10.003
- Gadalla M, Huang S, Wang R, et al. Effect of clomiphene citrate on endometrial thickness, ovulation, pregnancy and live birth in anovulatory women: systematic review and meta‐analysis. Ultrasound Obstet Gynecol. 2018;51(1):64–76. https://doi.org/10.1002/uog.18933
- Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS consensus workshop group. Fertil Steril. 2012;97(1):28–38. https://doi.org/10.1016/j.fertnstert.2011.09.024
- Stadtmauer LA, Wong BC, Oehninger S. Should patients with polycystic ovary syndrome be treated with metformin? Benefits of insulin sensitizing drugs in polycystic ovary syndrome—beyond ovulation in Hum Reprod. 2002;17(12):3016–3026. https://doi.org/10.1093/humrep/17.12.3016
- Nafiye Y, Sevtap K, Muammer D, Emre O, Senol K, Leyla M. The effect of serum and intrafollicular insulin resistance parameters and homocysteine levels of nonobese, nonhyperandrogenemic polycystic ovary syndrome patients on in vitro fertilization outcome. Fertil Steril. 2010;93(6):1864–1869. https://doi.org/10.1016/j.fertnstert.2008.12.024
- Morishita M, Endo T, Baba T, et al. Pioglitazone is effective for multiple phenotyepes of the Zucker fa/fa rat with polycystc ovary morphology and insulin resistance. J Ovarian Res. 2018;11(1):1–8. https://doi.org/10.1186/s13048-018-0395-y
- Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602–16018. https://doi.org/10.1093/humrep/dey256
- Soldin OP, Hoffman EG, Waring MA, Soldin SJ. Pediatric reference intervals for FSH, LH, estradiol, T3, free T3, cortisol, and growth hormone on the DPC IMMULITE 1000. Clin Chim Acta. 2005;355(1-2):205–210. https://doi.org/10.1016/j.cccn.2005.01.006
- Qiu Q, Kuo A, Todd H, et al. Enzyme immunoassay method for total urinary follicle-stimulating hormone (FSH) beta subunit and its application for measurement of total urinary FSH. Fertil Steril. 1998;69(2):278–285. https://doi.org/10.1016/S0015-0282(97)00475-5
- Williamson M, Viau V. Androgen receptor expressing neurons that project to the paraventricular nucleus of the hypothalamus in the male rat. J Comp Neurol. 2007;503(6):717–740. https://doi.org/10.1002/cne.21411
- Tietz N. Clinical guide to laboratory tests. WB Sannders, Co. Phila. 1995.
- Al-Inany H, Azab H, El-Khayat W, Nada A, El-Khattan E, Abou-Setta AM. The effectiveness of clomiphene citrate in LH surge suppression in women undergoing IUI: a randomized controlled trial. Fertil Steril. 2010;94(6):2167–2171. https://doi.org/10.1016/j.fertnstert.2010.01.069
- Kawwass JF, Loucks TL, Berga SL. An algorithm for treatment of infertile women with polycystic ovary syndrome. Middle East Fertil Soc J. 2010;15(4):231–239. https://doi.org/10.1016/j.mefs.2010.07.010
- Ainehchi N, Khaki A, Ouladsahebmadarek E, et al. The effect of clomiphene citrate, herbal mixture, and herbal mixture along with clomiphene citrate on clinical and para-clinical parameters in infertile women with polycystic ovary syndrome: a randomized controlled clinical trial. Arch Med Sci. 2020;16(6):1304–1318. https://doi.org/10.5114/aoms.2020.93271
- Ayaz A, Alwan Y, Farooq MU. Metformin—clomiphene citrate vs. clomiphene citrate alone: Polycystic ovarian syndrome. J Hum Reprod Sci. 2013;6(1):15–18. https://doi.org/10.4103/0974-1208.112372
- Dupont J, Scaramuzzi RJ. Insulin signalling and glucose transport in the ovary and ovarian function during the ovarian cycle. Biochem J. 2016;473(11):1483–1501. https://doi.org/10.1042/BCJ20160124
- Porter DT, Moore AM, Cobern JA, et al. Prenatal testosterone exposure alters GABAergic synaptic inputs to GnRH and KNDy neurons in a sheep model of polycystic ovarian syndrome. Endocrinology. 2019;160(11):2529–2542. https://doi.org/10.1210/en.2019-00137
- Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687–708. https://doi.org/10.1093/humupd/dmw025
- The Royal College of Obstetricians and Gynaecologists. Fertility: assessment and treatment for people with fertility problems. https://www.ncbi.nlm.nih.gov/books/NBK247932/pdf/Bookshelf_NBK247932.pdf. Published 2013. Accessed December 6, 2023.
- ESHRE Capri Workshop Group. Health and fertility in World Health Organization group 2 anovulatory women. Hum Reprod Update. 2012;18(5):586–599. https://doi.org/10.1093/humupd/dms019
- Rees DA, Jenkins-Jones S, Morgan CL. Contemporary reproductive outcomes for patients with polycystic ovary syndrome: a retrospective observational study. J Clin Endocrinol Metab. 2016;101(4):1664–1672. https://doi.org/10.1210/jc.2015-2682
- Bruyneel A, Catteau-Jonard S, Decanter C, et al. Polycystic ovary syndrome: what are the obstetrical risks? Gynecol Obstet Fertil. 2014;42(2):104–111. https://doi.org/10.1016/j.gyobfe.2014.01.001