
| Review | Open Access |
|---|
Psychological Distress and Coping Styles in Young Adult Women: A Community-Based Correlational Study from Pakistan |
 |
|---|
Kishwar Altaf1*, Muhammad Rizwan2, and Razi Sultan Siddiqui3
1National University of Medical Sciences, Rawalpindi, Pakistan
2University of Wah, Wah Cantt, Pakistan
3DHA-SUFFA University, Karachi, Pakistan
With the increasing social, cultural and environmental demands, women are especially sensitive to psychological distress and thus, the concept of coping should be accompanied by the knowledge of how coping supports mental health and general well-being. It was a comparative cross-sectional study and aimed to establish the level of psychological distress and coping strategies among Pakistani women who were using to cope with the distress It used convenience sampling to recruit 249 women (aged 20-39 years). The Depression Anxiety Stress Scale (DASS-21) was used to measure psychological distress, including depression, anxiety, and stress, whereas the Brief COPE measured coping strategies, including problem-focused, emotion-focused, and avoidant coping. The results showed that a significant percentage of the women had moderate to high levels of psychological distress, and extremely severe anxiety. Results further indicate that maladaptive coping styles, i.e., avoidance coping, plays a significant role in expanding psychological distress among young adult women. Boosting adaptive coping style may therefore be critical for lowering level of distress symptoms. These findings would be useful for policymakers, clinicians, and mental health practitioners to develop relevant interventions that could improve the psychological well-being of women in Pakistan.
1. INTRODUCTION
Psychological distress is a multi-dimensional concept that includes a set of emotional and physical symptoms that usually follow stress, anxiety, and depression, and that may seriously impact the functioning of an individual in everyday life (Matthews, 2007). The psychological distress of women is especially likely to be caused by hormonal changes, psychological vulnerabilities, pressure of social norms, family responsibilities, and other environmental factors (Remes, 2021). Its persistence is additionally preconditioned by maladaptive thinking patterns, cognitive distortions, low distress tolerance, major life changes, traumatic experiences, work stress, family conflicts, financial burdens, and chronic health conditions those may trigger or worsen the level of distress (Cooper et al., 2019; Lawrance et al., 2022; Obrenovic et al., 2020). Negative interpersonal experiences, social isolation, and the absence of support may tighten the knot of distress, exposing people to mental health issues in the long term (Brandt et al., 2022). Psychological distress may have a harmful impact on body-image, decreasing self-esteem, and causes problems with social and interpersonal relations (Alur-Gupta et al., 2019). In this regard, coping skills have a significant role in addressing psychological difficulties and leading to well-being (Dewani et al., 2023).
Coping is defined as the personal style that is used by individuals to face and deal with stress, situations that cause anxiety, or crises. It is a complex phenomenon that focuses on the mental and behavioral mechanisms that human beings employ to re-experience, adjust, and cope with stressful events to reduce emotional stress (Algorani & Gupta, 2023). The styles of coping, relatively stable over time, define the reactions of people to stress and problematic situations (Boer et al., 2017) and indicate the capacity of an individual to adapt to the environmental conditions and stress, and they are shaped by neurophysiological, cognitive, emotional, and social factors that change during the lifespan (Frydenberg, 2014). The coping styles used by individuals to cope with stress are an important aspect of ensuring psychological and emotional well-being because they determine the impact of stress on the evolution of mental disorders (Carron et al., 2017). The high problem-low coping and low maladaptive coping have also been linked with more significant psychological distress (Carron et al., 2017), and the overall quality of life is more likely to be reduced with the rise in the level of psychological distress which is why coping strategies are crucial. Mental health is thus needed to initiate strategies that reduce psychological distress and improve coping mechanisms. The current state of mental health awareness does not solve the problem, and most women in Pakistan continue to struggle with coping with psychological stress and implementing adaptive coping behaviors. Depression and anxiety lead to psychological distress that adversely affects self-esteem and body image and increases the difficulty in coping with everyday stress (Light et al., 2021). This makes it clear that there is a need to study the distribution of psychological distress and coping mechanisms among women to be informed about culturally specific interventions that can be used to improve well-being. The available literature demonstrates that the prevalence of psychological distress is extremely high and that coping strategies are significant in women but the vast majority of the research has been conducted in clinical populations or particular medical conditions. Community-based studies on psychological distress and coping styles in the general Pakistani population of women are limited. Moreover, few studies have jointly examined depression, anxiety, stress, and coping strategies within a single framework. Addressing this gap, the present study investigates psychological distress and coping styles among young adult women in Pakistan, providing contextually relevant evidence to inform mental health interventions.
Literature Review
Women experience psychological distress in different regions of the world, which are affected by social, cultural and environmental factors, which also influence coping mechanisms and general psychological wellbeing. Although it has become more enlightened, a significant number of women have limited support in relation to mental health problems, which is why adaptive coping strategies should be fostered to increase resilience and quality of life. The study highlights the high psychological burden that women face, such as low self-esteem, anxiety, and depression, and the need to find effective coping mechanisms to reduce such effects (Alkheyr et al., 2024).
Coping strategies are mostly categorized as either adaptive or maladaptive. Growing psychological outcomes are associated with adaptive strategies (problem-solving, seeking support, and making constructive changes), whereas maladaptive strategies (such as avoidance, denial, and disengagement) can intensify distress (Fischer et al., 2021; Tindle et al., 2022). The mechanisms of coping depend on the experiences of early years, the style of attachment, and the developmental stages, and successful coping depends on the ability to balance the minimization of stressors and the increase in the capacity to deal with them (Schaffner, 2023). The strategies are especially important in reducing the impact of depression, anxiety, and stress which are common among the women and which considerably influence the functional daily life (Albert, 2015).
Hopkins et al. (2019) studied the aspects of psychological distress and coping and pointed out that the perceived inability to control stressful situations is related to the increased prevalence of depression. The instruments used in the study were standardized, such as Coping Inventory of Stressful Situations (CISS), and Beck Depression Inventory (BDI), which were used to measure coping and depressive symptoms. Results indicated that coping measures are very important in alleviating psychological distress and coping with difficult life situations.
Likewise, Ain and Gul (2023) investigated how coping strategies and psychological distress are related in a group of women with a 20 to 35 age range. The study measured problem-focused coping and psychological distress with the help of Brief COPE Scale and a Psychological Distress Scale and discovered that there was a strong correlation between the two variables. Such findings suggest that adaptive coping mechanisms may support in dealing with emotional difficulties, but the individual perception and reaction to stressors also play a role on the outcome of distress.
To bring a wider image, Macahilig (2024) examined the coping capacities and psychological distress among women and found that women employ adaptive and maladaptive coping strategies. This research indicated that the moderate levels of psychological distress, which were associated with symptoms of fatigue, nervousness and depressive symptoms, could be reduced through adaptive coping. However, the maladaptive coping strategies had at least an ability to reduce distress but also present a risk of continuing or even increasing negative psychological outcomes. Such findings reveal that both coping and mental health are rather interdependent and must be substituted by particular interventions that will increase adaptive coping and relieve distress.
All these works, however, lead to a logical conclusion that the state of psychological distress and coping mechanisms are closely interconnected, and adaptive coping is always associated with a more pleasant emotional state and maladaptive coping is always capable of becoming the source of ongoing distress. Notably, there has been some gaps in explaining these dynamics in various cultural settings especially among the women in Pakistan where familial, social, cultural and environmental factors could have additional effect on the psychological outcomes and coping strategies. To fill these gaps, the current study explored the psychological distress and different coping mechanisms among Pakistani women. From a theoretical perspective, the findings of this study align with stress and coping frameworks that emphasize the role of individual coping responses in determining psychological outcomes. According to transactional models of stress, the way individuals appraise stressors and select coping strategies directly influences emotional well-being. Maladaptive coping styles such as avoidance may provide short-term relief but often exacerbate distress over time, whereas adaptive coping strategies support resilience and psychological adjustment.
Rationale
The biological, familial, social, and environmental factors of psychological well-being in women have a complicated interaction, and disturbances in well-being are directly associated with anxiety, depression, low self-esteem, and poor quality of life (Ligocka et al., 2024). Among all women of reproductive age, 6 to 13 % are exposed to mental health issues that impact their daily functioning quite severely, with notable regional differences, such as South Asia (Bozdag et al., 2016; WHO, 2025). Socio-cultural requirements, stigma of mental illness, and access to psychological care in Pakistan can increase the exposure to psychological distress and maladaptive coping strategies. Although these are the concerns, there is only limited empirical study on how women in the general population can adapt emotionally to the strain and endure the psychological well-being. The current literature is mostly devoted to clinical populations or specific health issues, creating a tremendous gap in the knowledge about the general trends in emotional resilience, coping strategies, and mental health in women living in the community. This gap must be addressed to come up with culturally relevant mental health support systems. The further insight into the prevalence of the psychological distress and the strategies most often employed to overcome the problem, as well as their implications on the level of well-being, can direct the efficacy of intervention, policy creation, and the mental health awareness campaigns adjusted to the needs of women in Pakistan.
Objectives
- To assess the occurrence of high psychological distress (depression, anxiety, and stress) among women in Pakistan.
- To analyze the relationship between psychological distress (depression, anxiety, and stress) and coping strategies among women in Pakistan.
Hypotheses
H1: A substantial proportion of women will exhibit moderate to high levels of psychological distress.
H2: There would be significant relationship between psychological distress (depression, Anxiety, and Stress) and coping styles (emotion focused, problem focused, avoidant coping) among women in Pakistan.
Material and Methods
This study employed a comparative cross-sectional quantitative design to examine psychological distress (Depression, Anxiety, and Stress) and its relationship with coping styles (Emotion focused, Problem focused, Avoidant coping) among adult women in Pakistan. Two hundred and forty-nine women (249 20 39 years old) were selected by convenience sampling out of the general populations. The inclusion criteria included that the participants must fall within the age range of specification and they must have adequate understanding of English so that they can comprehend the questionnaires.
The convenience sampling was chosen because of the feasibility and a lack of access to population registries, and the recruitment of the participants with varied education and socioeconomic backgrounds was done. To prevent confounding variables, exclusion criteria were a diagnosed psychiatric condition, a chronic medical condition or psychiatric treatment that was underway. The level of psychological distress was measured by the Depression, Anxiety, and Stress Scale (DASS-21), with adequate-high levels of internal consistency (a =.70-.90), and coping strategies were assessed using Brief COPE Inventory (emotion focused, problem focused, avoidant coping styles) with reliability of a =.74 to a =.86. Participants signed informed consent form and the NUMS Institutional Review Board granted ethical approval. Participants were assured that the information they share will remain confidential and anonymous. The involvement in the research would be voluntary and if they want, they can withdraw their participation without any negative consequences. This study employed a community-based, cross-sectional quantitative design to examine psychological distress (depression, anxiety, and stress) and its relationship with coping styles among young adult women in Pakistan.
Results
Based on the results of the statistical analyses, the study hypotheses were evaluated as follows. Hypothesis 1 proposed that a substantial proportion of women would exhibit moderate to high levels of psychological distress. This hypothesis was accepted, as a large percentage of participants reported moderate to extremely severe levels of depression, anxiety, stress, and overall psychological distress.
Hypothesis 2 proposed that there would be a significant relationship between psychological distress (depression, anxiety, and stress) and coping styles. This hypothesis was partially accepted. Emotion-focused and avoidant coping styles showed significant positive relationships with all components of psychological distress, indicating that higher reliance on these coping styles was associated with greater distress. However, problem-focused coping did not show a significant relationship with psychological distress and was therefore not supported in this sample.
Table 1
Frequency and Percentages of Demographic Variables (N = 249)
|
Variables |
f (%) |
|---|---|
|
Education Matriculation Intermediate Undergraduate Postgraduate |
3(1.2) 20(8) 145(58.2) 81(32.5) |
|
Age 20-24 years 25-29 years 30-34 years 35-39 years |
186(74.7) 51(20.5) 8(3.2) 4(1.6) |
|
Family system Nuclear Joint |
188(75.5) 61(24.5) |
|
Occupation Housewife Working women |
28(11.2) 221(88.8) |
|
Financial status of family Upper Upper middle Middle Lower middle |
9(3.6) 91(36.5) 138(55.4) 11(4.4) |
|
Marital status Unmarried Married Divorced |
225(90.4) 23(9.2) 1(.4) |
Table 2
Psychometric Properties of DASS-21 and Brief COPE (N = 249)
|
Variables |
k |
ɑ |
M |
SD |
Range |
Skewness |
Kurtosis |
||
|---|---|---|---|---|---|---|---|---|---|
|
Potential |
Actual |
||||||||
|
Depression, Anxiety & Stress Scale (DASS-21) |
|
||||||||
|
Depression |
7 |
.87 |
15.73 |
10.51 |
0-42 |
0-40 |
.25 |
-.85 |
|
|
Anxiety |
7 |
.79 |
16.73 |
9.64 |
0-42 |
0-38 |
.13 |
-.83 |
|
|
Stress |
7 |
.82 |
16.89 |
9.24 |
0-42 |
0-42 |
.09 |
-.68 |
|
|
Psychological distress |
21 |
.93 |
49.36 |
26.91 |
0-126 |
0-104 |
-.01 |
-1.02 |
|
|
Coping Orientation to Problems Experienced Inventory (Brief-COPE) |
|
||||||||
|
Problem Focused |
8 |
.86 |
2.34 |
.71 |
8-32 |
8-32 |
.33 |
-.59 |
|
|
Emotion Focused |
12 |
.77 |
2.33 |
.56 |
12-48 |
12-48 |
-.27 |
.22 |
|
|
Avoidant Coping |
8 |
.74 |
2.08 |
.57 |
8-32 |
8-24 |
-.03 |
-1.08 |
|
Table 3
Frequency and Percentage of Psychological Distress across Five-Band Categories of Severity Levels (N = 249)
|
Category |
Depression f (%) |
Anxiety f (%) |
Stress f (%) |
Psychological distress f (%) |
|---|---|---|---|---|
|
Normal |
77(30.9) |
42(16.9) |
110(44.2) |
79(31.7) |
|
Mild |
28(11.2) |
22(8.8) |
30(12) |
12(4.8) |
|
Moderate |
61(24.5) |
49(19.7) |
60(24.1) |
32(12.9) |
|
Severe |
45(18.1) |
32(12.9) |
43(17.3) |
19(7.6) |
|
Extremely severe |
38(15.3) |
104(41.8) |
6(2.4) |
107(43) |
The data was analyzed for the distribution of psychological distress among the five severity levels (normal, mild, moderate, severe, and extremely severe) of depression, anxiety, stress, and psychological distress. Determining depression, the ratio of the population within normal scores was 30.9%. Mild and moderate categories were present in 11.2% and 24.5% samples respectively. However, 18.1% of the participants reported severe depression followed by 38% of extremely severe level of depression. In the case of anxiety, 16.9% presented in the normal range of anxiety, 8.8% in the mild range and 19.7% in moderate range. This distribution was followed by 12.9% of respondents in severe and 41.8% in extremely severe range. In case of stress, 44.2% of respondents fell under the normal category, 12% and 24.1% participants were showing mild and moderate stress severity respectively. Among the others, 17.3% respondents reported severe level of stress whereas only 2.4% respondents had extremely severe level of stress. Overall, psychological distress was predominant as extremely severe category (43%), followed by normal (31.7%), moderate (32%), severe (7.6%) and mild (4.8%). The results indicate that a substantial proportion of participants experienced moderate to extremely severe levels of psychological distress, with anxiety emerging as the most prevalent condition. Overall psychological distress was also notably high, suggesting a considerable emotional burden among the sampled women. These findings demonstrate that psychological distress is a significant concern in this population.
Figure 1
Prevalence of Psychological Distress across Five Categories of Severity
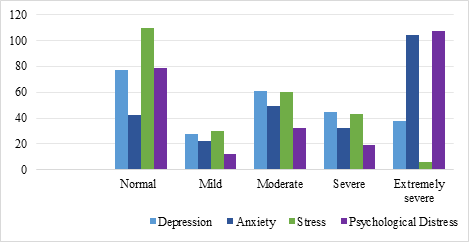
Table 4
Frequency and Percentage of Coping Styles across Three-band Categories of Coping Levels (N = 249)
|
Category |
Problem-focused f (%) |
Emotion-focused f (%) |
Avoidant f (%) |
|---|---|---|---|
|
Low |
21(8.4) |
19(7.6) |
37(14.9) |
|
Moderate |
121(48.6) |
123(49.4) |
128(51.4) |
|
High |
107(43) |
105(42.2) |
84(33.7) |
Figure 2
Frequency of Coping Styles across Three-band Categories of Coping Levels
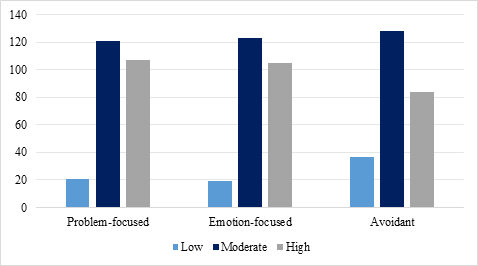
Table 5
Correlation between Psychological Distress and Coping Skills (N = 249)
|
|
Variables |
1 |
2 |
3 |
4 |
5 |
6 |
|---|---|---|---|---|---|---|---|
|
1 |
Depression |
- |
- |
- |
- |
- |
- |
|
2 |
Anxiety |
.70** |
- |
- |
- |
- |
- |
|
3 |
Stress |
.82** |
.76** |
- |
- |
- |
- |
|
4 |
Psychological Distress |
.92** |
.89** |
.93** |
- |
- |
- |
|
5 |
Problem focused coping |
-.07 |
.01 |
-.01 |
-.02 |
- |
- |
|
6 |
Emotion focused coping |
.42** |
.45** |
.53** |
.50** |
.52** |
- |
|
7 |
Avoidant coping |
.62** |
.62** |
.63** |
.68** |
.03 |
.54** |
Note. *p < .05. **p <. 01.
The Pearson product–moment correlation analysis was applied to statistically examine the associations among depression, anxiety, and stress (psychological distress) and the problem-focused, emotion-focused, and avoidant coping styles. Results show that depression, anxiety, and stress were all strongly related with one another (r = .70 to .82, p < .001) and with overall psychological distress (r = .89 to .93, p < .001) in positive direction. Concerning coping styles, emotion-focused style displayed significant positive correlations with depression (r = .42, p < .001), anxiety (r = .45, p < .001), stress (r = .53, p < .001), and overall psychological distress (r = .50, p < .001). Similarly, emotion-focused coping was also positively associated with problem-focused coping (r = .52, p < .001) and avoidant coping (r = .54, p < .001). Furthermore, avoidant coping showed significant positive associations with depression (r = .62, p < .001), anxiety (r = .62, p < .001), stress (r = .63, p < .001), and overall psychological distress (r = .68, p < .001). However, problem-focused coping showed no significant correlations with depression, anxiety and stress (r = -.07; p =.01; –.01) or overall psychological distress (r = -.02), representing that use of problem-focused style was not related with distress in this sample.
Discussion
The current study investigated psychological distress and its relationship with coping strategies among adult women in Pakistan. Findings indicate that a substantial proportion of participants experienced moderate to high levels of psychological distress. Specifically, while normal stress levels were reported by 44.2% of participants, extremely severe anxiety was the most prevalent (41.8%), followed by extreme overall psychological distress (43%). The findings shows that the quantity of emotional difficulties is significant between women. In line with prior studies, Cooney et al. (2017) reported that women quite often highly anxious and depressed, which adversely affects their quality of life. Equally, Tang et al. (2019) have suggested that psychological distress in women is a major influence in coping with illogical stressors, in line with their high rates of anxiety. Ligocka et al. (2024) emphasized that low self-esteem and poor physical image tendencies are the most accepted psychological stressors among women. This is in addition to the fact that the current study has observed that the moderate to high levels of distress were common which implies that the presence of emotional strain can affect the self-perception and coping behaviors in the Pakistani setting. The findings of the present study indicate that psychological distress is prevalent among young adult women in Pakistan, with anxiety and overall distress reported at notably high levels. These results suggest an association between emotional difficulties and coping patterns rather than direct causation. The high levels of distress observed may reflect the combined influence of social pressures, limited mental health resources, and cultural expectations placed on women within the Pakistani context.
On coping strategies, the findings indicated that many of the participants used moderate level problem-focused and emotion-focused coping, and moderate to high levels of avoidant coping. This trend shows that women are trying to adopt adaptive coping mechanisms to deal with stress, but avoidant coping may support or even increase distress. Similar results were observed by Carron et al. (2017), who reported that low problem-oriented and high maladaptive coping are associated with psychological distress, which is very consistent with the current results. In reference to adaptive and maladaptive coping strategies, Fischer et al. (2021) have already indicated that proactive coping (problem-solving and emotional regulation) is more likely to positively influence mental health, whereas avoidance or denial might have a negative impact. The results also highlight the contribution of social-cultural and environmental factors to the development of coping responses. The societal pressure, gender-related expectations, and mental health scarcity in Pakistan could be factors that led to the distress rate and avoidance as a problem-solving approach. These findings indicate that culturally sensitive interventions should be implemented to increase adaptive coping skills and decrease the psychological burden.
Overall, the findings highlight the importance of coping styles in understanding psychological distress among women. While problem-focused coping did not show a significant association with distress in this sample, avoidant coping was consistently related to higher levels of emotional difficulties. These results underline the need for mental health initiatives that promote adaptive coping strategies while addressing contextual and cultural factors influencing women’s psychological well-being in Pakistan.
Limitations
Although it makes some contributions, this study has a number of limitations that need to be highlighted. To begin with, convenience-based sampling method restricts the applicability of the research findings to the entire population of women in Pakistan. Second, the cross-sectional and correlational design do not allow to make causal conclusions about the association between coping strategies and psychological distress. Third, the use of self-report measures can result in bias in response, such as social desirability and recall bias.
The future research must use longitudinal and experimental designs to have a better insight into the causal relationship between coping styles and psychological distress. Larger and more diverse samples in the other regions of Pakistan are also suggested in studies. In addition, the qualitative approaches can be included or the clinician-administered tests can help better understand culturally specific coping strategies. The research ought also to be conducted on the usefulness of specific interventions which could be used to encourage adaptive coping skills and decrease maladaptive coping in women.
Conclusion
In conclusion, the research study at hand can contribute to the future studies, interventions and mental health programs to address the psychological issues of women based on the research findings. The findings through the enlightenment of the policymakers and mental health practitioners indicate that culturally sensitive strategies that can ensure adaptive coping and facilitate psychological well-being in the Pakistani setting are necessary.
Conflict of Interest
The authors of the manuscript have no financial or non-financial conflict of interest in the subject matter or materials discussed in this manuscript.
Data Availability Statement
Data supporting the findings of this study will be made available by the corresponding author upon request.
Funding Details
No funding has been received for this research.
REFERENCES
Ain, Q.-U., & Gul, A. (2023). Illness perception, coping strategies, and psychological distress among women with polycystic ovary syndrome. Pakistan Journal of Medical and Health Sciences, 17(2), 261–264. https://doi.org/10.53350/pjmhs2023172261
Albert, P. (2015). Why is depression more prevalent in women? Journal of Psychiatry & Neuroscience, 40(4), 219–221. https://doi.org/10.1503/jpn.150205
Algorani, E. B., & Gupta, V. (2023). Coping mechanisms. StatPearls Publishing.
Alkheyr, Z., Murad, M., Das, P., Aljenaee, K., Kamel, C., Ali Hajji, S., Flood, J., Atkin, S. L., & Ali, K. F. (2024). Self-esteem and body image satisfaction in women with PCOS in the Middle East: A cross-sectional social media study. PLOS ONE, 19(4), Article e0301707. https://doi.org/10.1371/journal.pone.0301707
Alur-Gupta, S., Chemerinski, A., Liu, C., Lipson, J., Allison, K., Sammel, M. D., & Dokras, A. (2019). Body-image distress in women with polycystic ovary syndrome and its association with depression and anxiety. Fertility and Sterility, 112(5), 930–938. https://doi.org/10.1016/j.fertnstert.2019.06.018
Boer, S. F. de, Buwalda, B., & Koolhaas, J. M. (2017). Untangling the neurobiology of coping styles: Neural mechanisms underlying individual differences in disease susceptibility. Neuroscience & Biobehavioral Reviews, 74, 401–422. https://doi.org/10.1016/j.neubiorev.2016.07.008
Bozdag, G., Mumusoglu, S., Zengin, D., Karabulut, E., & Yildiz, B. O. (2016). The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Human Reproduction, 31(12), 2841–2855. https://doi.org/10.1093/humrep/dew218
Brandt, L., Liu, S., Heim, C., & Heinz, A. (2022). The effects of social isolation stress and discrimination on mental health. Translational Psychiatry, 12(1), 1–11. https://doi.org/10.1038/s41398-022-02178-4
Carron, R., Kooienga, S., Boyle, D. K., & Alvero, R. (2017). Coping in women with polycystic ovary syndrome: Implications for practitioners. The Journal for Nurse Practitioners, 13(10), 700–707. https://doi.org/10.1016/j.nurpra.2017.08.004
Cooney, L. G., Lee, I., Sammel, M. D., & Dokras, A. (2017). High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: A systematic review and meta-analysis. Human Reproduction, 32(5), 1075–1091. https://doi.org/10.1093/humrep/dex044
Cooper, S., Hutchings, P., Butterworth, J., Joseph, S., Kebede, A., Parker, A., Terefe, B., & Van Koppen, B. (2019). Environmental associated emotional distress and the dangers of climate change for pastoralist mental health. Global Environmental Change, 59, Article e101994. https://doi.org/10.1016/j.gloenvcha.2019.101994
Dewani, D., Karwade, P., & Mahajan, K. S. (2023). The invisible struggle: The psychosocial aspects of polycystic ovary syndrome. Cureus, 15(12), Article e51321. https://doi.org/10.7759/cureus.51321
Fischer, R., Scheunemann, J., & Moritz, S. (2021). Coping strategies and subjective well-being: Context matters. Journal of Happiness Studies, 22, 3413–3434. https://doi.org/10.1007/s10902-021-00372-7
Frydenberg, E. (2014). Coping research: Historical background, links with emotion, and new research directions. Australian Journal of Psychology, 66(2), 82–92. https://doi.org/10.1111/ajpy.12051
Hopkins, C. S., Kimble, L. P., Hodges, H. F., Koci, A. F., & Mills, B. B. (2019). Coping and depression in adolescent girls with polycystic ovary syndrome: A mixed-methods study. Journal of the American Association of Nurse Practitioners, 31(3), 189–197. https://doi.org/10.1097/JXX.0000000000000125
Lawrance, E. L., Thompson, R., Newberry Le Vay, J., Page, L., & Jennings, N. (2022). The impact of climate change on mental health and emotional wellbeing: A narrative review. International Review of Psychiatry, 34(5), 443–498. https://doi.org/10.1080/09540261.2022.2128725
Light, R. S., Chilcot, J., & McBride, E. (2021). Psychological distress in women living with polycystic ovary syndrome: The role of illness perceptions. Women's Health Issues, 31(2), 177–184. https://doi.org/10.1016/j.whi.2020.11.003
Ligocka, N., Chmaj-Wierzchowska, K., Wszołek, K., Wilczak, M., & Tomczyk, K. (2024). Quality of life of women with polycystic ovary syndrome. Medicina, 60(2), Article e294. https://doi.org/10.3390/medicina60020294
Macahilig, M. (2024). Psychological distress and coping styles of women living with polycystic ovarian syndrome. Journal of Pregnancy and Child Health. Advance online publication. https://doi.org/10.4172/2376-127x
Matthews, G. (2007). Distress. In G. Fink (Ed.), Encyclopedia of stress (pp. 838–843). Academic Press.
Obrenovic, B., Jianguo, D., Khudaykulov, A., & Khan, M. A. S. (2020). Work–family conflict and psychological well-being. Frontiers in Psychology, 11, 475. https://doi.org/10.3389/fpsyg.2020.00475/
Remes, O. (2021). Biological, psychological, and social determinants of depression: A review. Brain Sciences, 11(12), 1633. https://doi.org/10.3390/brainsci11121633
Schaffner, A. K. (2023, September 19). Unhealthy coping mechanisms. PositivePsychology.com. https://positivepsychology.com/unhealthy-coping-mechanisms/
Tang, R., Luo, M., Li, J., Peng, Y., Wang, Y., Liu, B., Liu, G., Wang, Y., Lin, S., & Chen, R. (2019). Anxiety and depression among women transitioning through menopause. Fertility and Sterility, 112(6), 1160–1171. https://doi.org/10.1016/j.fertnstert.2019.08.005
Tindle, R., Hemi, A., & Moustafa, A. A. (2022). Social support, psychological flexibility, and coping in psychological distress. Scientific Reports, 12(1), 1–12. https://doi.org/10.1038/s41598-022-12262-w